
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A case report with imaging features of labyrinthitis
ossificans in an adult male
Avantika Singh1*; Vishal Gupta2; Saurav Bhagat3; Ashita Gupta4; Parnit Kalra1
12nd year Junior Resident, Department of Radiology, School of Medical Science and Research, Sharda University, Greater Noida, Uttar Pradesh, India.
2Professor & Head, Department of Radiology, School of Medical Science and Research, Sharda University, Greater Noida, Uttar Pradesh, India.
3Assistant Professor, Department of Radiology, School of Medical Science and Research, Sharda University, Greater Noida, Uttar Pradesh, India.
41st year Junior Resident, Department of Radiology, School of Medical Science and Research, Sharda University, Greater Noida, Uttar Pradesh, India.
*Corresponding Author : Avantika Singh
Room no 911, PG hostel, Sharda University, Greater Noida, Uttar Pradesh, India.
Tel: 8652403796;
Email: avantika238@gmail.com
Received : Apr 21, 2023
Accepted : May 17, 2023
Published : May 24, 2023
Archived : www.jcimcr.org
Copyright : © Singh A (2023).
Abstract
Labyrinthitis Ossificans (LO) is a pathological condition that results in the ossification of the inner ear structures. It occurs mainly due to infection and inflammation with the former being a more common cause. It may occur in patients having tumor, hemorrhage, or trauma of the temporal bone. Inflammation disrupts the neurosensory signal transmission pathway to the brain. We present a case report of a 36-year-old male with left-sided hearing loss, discharge, positional vertigo, and nystagmus from 10 years with the review of his CT and MRI findings.
Abbreviations: CT: Computed Tomography; MRI: Magnetic Resonance Imaging; HRCT: High Resolution Computed Tomography; NCCT: Non-Contrast Computed Tomography; LO: Labyrinthitis Ossificans; DM: Diabetes Mellitus; HTN: Hypertension.
Citation: Singh A, Gupta V, Bhagat S, Gupta A, Kalra P, et al. A case report with imaging features of labyrinthit is ossificans in an adult male. J Clin Images Med Case Rep. 2023; 4(5): 2427.
Introduction
Ossification of structures inside the endosteum of the otic capsule of the inner ear is known as labyrinthitis ossificans [1]. Patients typically have Sensorineural Hearing Loss (SNHL) in the ear that is affected [4]. With a reported frequency of just 2%, LO is extremely uncommon [1]. Numerous etiologies have been noted, such as contiguous spread from the auditory canal, hematogenous spread, post-traumatic, surgical (labyrinthectomy, stapedectomy), etc. [6]. Beginning at the cochlea’s basal turn (the Scala tympani), LO advances to the cochlear apex [3]. Generally, the vestibule is least significantly affected while the semicircular canals are more significantly affected [5]. Knowing the site of involvement and the level of ossification is crucialfor preoperative counselling and postoperative education of the patient [1]. For hearing preservation, early detection of LO is needed [6].
Case report
A 36-year-old male patient presented with a history of left-sided progressive hearing loss and discharge for 10 years. There was a history of vertigo and nystagmus. No history of facial nerve palsy was seen. No history of meningitis. No history of DM or HTN. On examination, there was foul-smelling discharge from the left ear.
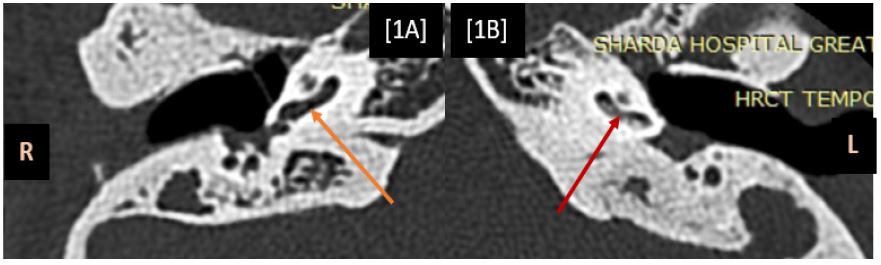
The HRCT was done on 128 slice CTGEOPTIMA. It shows ossification and sclerosis of varying degrees, involving the cochlea and vestibule on the left side. Middle ear cholesteatoma was noted on both sides. The superior, posterior, and lateral semi-circular canals were not visualized on the left side.
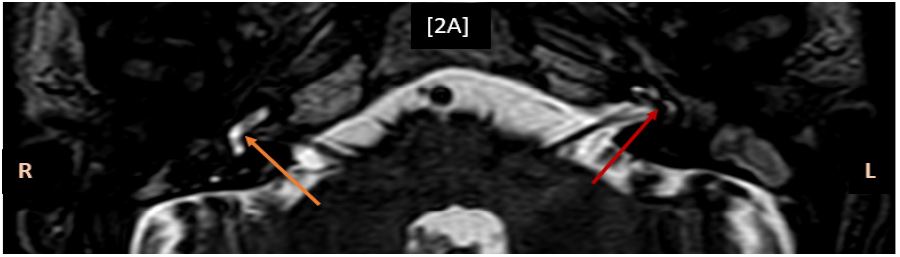
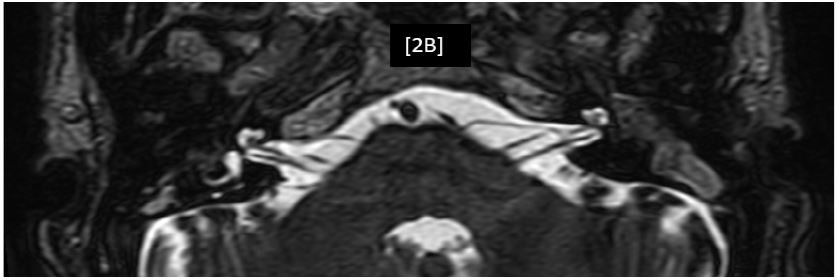
The MRI was done on PHILIPS3 Tesla ACHIVA. MRI images demonstrated partial loss of normal T2 hyperintense fluid signal in the basal turn of the cochlea with non-visualization of superior, posterior, and lateral semi-circular canals on the left side. There was middle ear cholesteatoma in both ears.
CT findings


MRI findings
Discussion
Several etiologies can lead to labyrinthine ossification. The most frequent type, tympanogenic labyrinthitis, frequently results from cholesteatoma or chronic otitis media problems. The inflammatory process usually starts from the fenestrae (round window or oval window) or from fistulae at the level of the lateral (horizontal) semicircular canal. Secondary to meningitis, meningogenic labyrinthitis is frequently bacterial in nature. The internal acoustic meatus and the cochlear aqueduct are the most well-known routes of spread. The norm is bilaterality. Another suggested etiology is a labyrinthine fracture with meningitic consequences. Often, the process is conducted alone. It is extremely uncommon for hematogenic labyrinthitis to develop as a result of blood-borne illnesses like measles or the mumps and cause labyrinthine ossification. The cause may be secondary endosteal proliferation brought on by inner ear hemorrhage and post-traumatic labyrinthine ossification. The labyrinthectomy itself leads to the development of labyrinthine ossification as well. The neo-osteogenesis brought on by the vascular compromise may be a contributing factor in the pathogenesis [2]. 6-37% of meningitis patients have hearing loss, with an estimated 5% having significant deafness, according to reports. Up to 80% of significant post meningitic deafness patients have labyrinthine ossification to a certain extent. A poor prognosis for residual hearing is linked to complete ossification. While being more prevalent in those in their 30s to 50s, it affects people of all ages. Females are 1.5 times as sensitive as males [5]
The basal turn of the cochlea close to the round window is where LO normally begins, followed by the involvement of the cochlear apex [3]. Regardless of the side, the semicircular canals are generally more severely impacted than the cochlea and vestibules. The vestibule is least adversely affected on both sides [5]. Knowing the site of involvement and the level of ossification is crucial for preoperative counseling and postoperative education of the patient [1]. Patients have progressive sensorineural hearing loss clinically. For hearing preservation, early detection of LO is crucial. The placement of a cochlear implant may be hampered or possibly made impossible by cochlea ossification [6].
Although MRI is more effective at spotting early fibrous changes in the membranous labyrinth, CT and MRI are believed to be complementary in the diagnosis of LO [4]. The membranous labyrinth shows high-density bone deposition on CT. Cochlea, semicircular canals, or vestibule sclerosis, irregularities, or obliteration with varying degrees of involvement is seen in LO [5]. At the end-stage LO, where the ossific material is visible clearly, NCCT is helpful. In the early stages of LO when CT imaging remains normal, MRI can play a critical role in the diagnosis [3]. Loss of the typical T2 hyperintense fluid signal in the inner ear is one of the MRI findings. Ossifications may appear as hypointense foci within the T2 hyperintense fluid of the inner ear [5].
The effective treatment for sensorineural hearing loss is cochlear implantation. Nevertheless, membranous labyrinth ossification might make electrode implantation challenging [5]. Permanent hearing loss in the patient is a terminal complication.
Labyrinthine or cochlear aplasia and otosclerosis are differential diagnoses. The labyrinth’s contour and shape are retained in LO. Nevertheless, labyrinthine aplasia can be identified by the absence of bilaterally distinct inner ear components. Another differential is otosclerosis, an osteodystrophy of the otic capsule that affects the cochlea in the “retro-fenestral” subtype as well as the oval window and stapes in the “fenestral” subtype.
Conclusion
The structures of the inner ear ossify in a condition called labyrinthitis ossificans. Clinically, the individuals have severe, irreversible hearing loss. It can be diagnosed on CT and MRI. On CT, the membranous labyrinth shows high-density bone deposition. On MRI, loss of the T2 hyperintense fluid signal in the inner ear is seen.
Imaging findings are crucial for prognostication as well as therapy recommendations (selection of suitable patients for cochlear implantation) [5].
If labyrinthine ossification is found on a CT scan, the observer should look for signs of a labyrinthectomy and look into the patient’s medical history, especially if there has been trauma, meningitis, or persistent otitis media [1].
References
- Buch K, Baylosis B, Fujita A, Qureshi MM, Takumi K, et al. Etiology-Specific Mineralization Patterns in Patients with Labyrinthitis Ossificans. AJNR Am J Neuroradiol. 2019; 40: 551-557.
- JD Swartz, DM Mandell, EN Faerber, GL Popky, JM Ardito, et al. Labyrinthine ossification: Etiologies and CT findings. Radiology. 1985; 157: 395-398.
- John C Benson, Matthew L Carlson, and John I Lane. MRI of the Internal Auditory Canal, Labyrinth, and Middle Ear: How We Do It. Radiology. 2020; 297: 252-265.
- Cody Larson, Scott A. Jorgensen, Alexander J. Towbin, and Richard Towbin, Labyrinthine ossificans.
- Taxak P, Ram C. Labyrinthitis and Labyrinthitis Ossificans - A case report and review of the literature. J Radiol Case Rep. 2020; 14: 1-6.
- Ignacio Soriano Aguadero, Alba Cristina Igual Rouilleault, Alberto Paternain Nuin, Manuel Manrique Rodríguez, María Reyes García de Eulate Ruiz, et al. Labyrinthitis ossificans: The earlier diagnosed, the better outcome.10.35100/eurorad/case.17108.