
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Isolated hepatomegaly revealing visceral toxocariasis:
A unique case report
I Fetoui1*; S Abbassi2; A Bourahouat1; R Elqadiry1; H Nassih1; R Moutaj2; I Aitsab1
1Service de Pédiatrie B, hôpital mère et enfant, Centre hospitalier universitaire Mohammed VI, Marrakech, Morocco.
2Service de parasitologie- mycologie, Hôpital militaire Ibn Sina, Marrakech, Morocco.
*Corresponding Author : Imane Fetoui
Service de Pédiatrie B, hôpital mère et enfant, Centre hospitalier universitaire Mohammed VI, Marrakech, Morocco.
Email: imanefetoui4@gmail.com
Received : Apr 21, 2023
Accepted : May 18, 2023
Published : May 25, 2023
Archived : www.jcimcr.org
Copyright : © Fetoui (2023).
Citation: Fetoui I, Abbassi S, Bourahouat A, Elqadiry R, Nassi H, et al. Isolated hepatomegaly revealing visceral toxocariasis: A unique case report. J Clin Images Med Case Rep. 2023; 4(5): 2429
Introduction
Toxocariasis is a zoonotic helminth infection secondary to the infestation of humans by larvae of Toxocara sp. These are nematodes of the Ascaridae family: Toxocara canis (dog parasite) and Toxocara cati (cat parasite) [1,2]. Multiple sero-epidemiological surveys have demonstrated that human toxocariasis is one of the most common cosmopolitan helminthiasis. The highest seroprevalence rates were observed in Africa (average 37.7%) and the lowest in the Eastern Mediterranean region (average 8.2%). The low socio-economic level, life in a rural environment, young age, the notion of geophagia, close contact with dogs and cats as well as poor environmental hygiene, are all factors potentially correlated with seropositivity at the toxocariasis [3-5]. In humans, the larvae from the hatching of embryonated eggs perforate the intestinal wall and migrate to the liver where the majority of them find themselves sequestered at a maturation deadlock within eosinophilic granulomas [6-8]. Different spectra of clinical presentation have been described for this affection, they vary from asymptomatic carriage to serious organic damage. Thus, 4 clinical forms are currently described: Visceral Larva Migrans Syndrome (VLM), ocular toxocariasis, common toxocariasis and neuro-toxocariasis. Ocular toxocariasis manifests primarily as decreased visual acuity without eosinophilia or systemic symptoms. The common form is characterized by abdominal pain, irritability and growth delay associated with hyper eosinophilia and high levels of anti-toxocara antibodies. Finally, neuro-toxocariasis is unusual in children and is manifested by neurological symptoms that can lead to headaches and epilepsy [9].
Observation
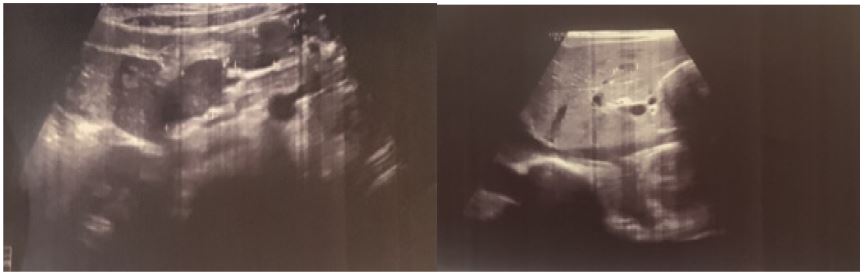
We report here the case of a child aged 2 years and 9 months, living in a rural area, with no particular pathological history, consulting for abdominal distension evolving for 2 months in a context of prolonged fever amounting to 38.5-39°C. The patient also complained of transit disorders consisting of alternating episodes of diarrhea and constipation, with no other associated signs, in a context of conservation of general condition. The clinical examination had objectified a child afebrile, pale, hemodynamically and respiratory stable, with on the abdomino-pelvic examination, a firm hepatomegaly, with a soft border, painless (hepatic arrow = 10 cm) without signs of acute liver failure nor heart failure. Examination of the lymph nodes did not reveal any palpable lymphadenopathy. As part of the etiological assessment, an abdominopelvic ultrasound was performed, showing heterogeneous hepatomegaly seat of multiple nodules, the largest of which measured 6.5 x 8.4 mm (Figure 1), associated with deep abdominal latero-caval lymphadenopathy. A complementary thoraco-abdomino-pelvic scan had objectified the same observation. The initial biological assessment had shown on the hemogram a microcytic hypochromic anemia as well as a hyperleucocytosis made of a massive hyper eosinophilia, with: WBC at 32530/mm3. Eosinophils (65%) absolute value at 21307/mm3; Platelets: 419,000. CRP was 27.3 mg/L. In addition, the rest of the biological assessment did not find hepatic cytolysis: ALT at 23 IU/L and AST at 40 IU/L nor biological cholestasis syndrome: GGT at 20 IU/L, ALP at 352 IU/L or signs of hepatocellular failure with a TP at 72.6%. Faced with the massive eosinophilia, amyelogram was performed showing a 35% hyper eosinophilia with no other abnormalities. Amoebic and hydatid parasite serologies were negative. Stool cultureand parasitological stool examinations were also negative.
Questioning was redone with the family showing a notion of geophagy and close contact with dogs suggesting visceral toxocariasis. In this sense, the serology of toxocariasis was carried out by ELISA method proving positive with an index of 59. This result was confirmed by Western blot highlighting the presence of specific anti-Toxocara canis antibodies: Ac anti p24, Ac anti p28, Ac anti p30 and Ac anti p35 positive. The diagnosis of toxocariasis in its Visceral Form (VLM) was set. The patient was put on albendazol at a rate of 20mg/kg/d for 5 days associated with symptomatic treatment (paracetamol and antispasmodic) as well as a martial treatment for his iron deficiency anemia.
The short-term evolution was marked by the apyrexia and the normalization of transit with a clear decrease in eosinophil levels to 216/mm3 within 5 days of starting treatment. The patient was seen again one month later, the clinical examination then objectified the disappearance of the hepatomegaly. The ultrasound control carried out noted a liver of normal size with persistent multinodular appearance.
Discussion
Visceral larva migrans (VLM) syndrome was first described in 1952 by Beaver et al. They reported the case of children presenting hepatomegaly with granulomatous lesions associated with a very important blood eosinophilia and identified the larvae found in the liver as belonging to the species T. canis [3]. VLM syndromes correspond to all the symptoms caused by the migration and survival in the body of toxocara larvae in a parasitic deadlock [10]. The larvae permanently reject soluble antigens known as “Excretory-Secretory” (TES Ag), of a glycoprotein nature. The host immune response, directed almost exclusively against these TES Ag, has been of crucial importance in the development of the immunological diagnosis of zoonosis [11]. The diagnosis of toxocariasis in humans is difficult because of the clinical polymorphism and the lack of specific signs of the disease.
The disease usually occurs in children 1 ± 4 years old with a history of pica syndrome, but can occur in older children or even in adulthood. The clinical manifestations of toxocariasis vary considerably and are determined by the size of the inoculum, the degree of host allergic response and the frequency of reinfections [12]. Common symptoms of VLM associated with hepatic and pulmonary or neurological larval migration often include abdominal pain, hepatomegaly, restlessness, fever, cough, wheezing, paleness, malaise, irritability, decreased appetite and weight loss [13]. Mild infections, making the most frequent picture, are usually asymptomatic and may not manifest as isolated hyper eosinophilia. In rare cases, the picture can be more severe, combining pneumonia, myocarditis, convulsions and even encephalitis [14]. Our patient’s clinical picture was rather benign with an acute fever revealing on examination an isolated hepatomegaly without any other associated signs. He had no ocular involvement but when it comes to ocular toxocariasis, the children do not complain. It is the parents who will notice eye changes, including strabismus, leucocoria or eye redness. Children may present with reduced visual acuity or unilateral blindness in severe forms [15], convulsions and further encephalitis [14].
On the radiological level, diagnostic imaging has improved remarkably over the past few decades. It can now provide information on the location of larvae andthe extent of the disease in the different organs of infected patients. The liver is the visceral organ most commonly affected by VLM. Typical hepatic granulomas are multinucleated giant cells and epithelioid cells surrounding necrotic debris or amorphous eosinophilic material [16]. Liver abscess is a condition rarely associated with Toxocariasis. On ultrasound, liver lesions present as multiple small oval hypoechoic lesions in the liver parenchyma. Lesions differ from metastatic nodules in that they have fuzzy margins, are uniform in size, non-spherical in shape, and are best seen at the portal vein stage [17]. These ultrasound findings are not specific and do not allow differentiation between lesions of other types of granuloma, inflammatory lesions or infarction. On CT or MRI, liver lesions appear as multiple well-defined oval lesions measuring 1.0 to 1.5 cm in diameter. Sometimes the lesion can be angular or trapezoidal [18]. On control imaging, the lesions may improve, or sometimes change position, reflecting the migration of the larvae into the liver, favoring the phenomenon of visceral larva migrans. For neurological involvement, the diagnosis of neuro toxocariasis is difficult because there is no distinct clinical syndrome. Various brain imaging findings have been reported including CT and MRI which were all suggestive, but none of them can be considered specific for neuro-toxocariasis, and most of these results can be seen in many other infectious or inflammatory conditions. These include: single or multiple hyper intense subcortical, cortical or white matter lesions, better visualized on FLAIR and T2-weighted imaging, generally isointense or hypo intense on T1 related to encephalitis or myelitis [19]. Three types of B-mode ocular toxocariasis have been reported, including peripheral or posterior pole granulomas and chronic endophthalmitis. The most consistent sonographic finding in the eye was a retinal mass with high reflectivity, located in the posterior pole or periphery, which may be calcified, and which has as its main characteristic the adhesion of vitreous membranes. A vitreous fold is a characteristic sign [20]. The radiological findings of pulmonary toxocariasis can be classified into four categories: GMO with or without solid part, solid nodules, uneven consolidations and focal linear opacity. Lung lesions primarily involve the sub pleural region and almost always involve the lower lung area. This distribution can be explained by larval migration from the peritoneal space to the lung via the pleural cavity [21]. In our case, the patient had performed a hepatic ultrasound concurring with the data in the literature with heterogeneous nodular hepatomegaly with hypoechoic lesions supplemented by a CT scan which had shown lesions that did not make it possible to distinguish between the other differential diagnoses, in particular the malignant origin. Hence the interest of integrating all the data, in particular epidemiological-clinical and biological.
Laboratory diagnosis can be guided by blood hyper eosinophilia (20 to 80G/L), especially massive in VLM, associated with hyper leukocytosis (20 to 100G/L) as well as an elevation of total IgE frequently found in patients presenting with common toxocariasis [2,22]. A biological inflammatory syndrome is common in VML and rare in common toxocariasis [22]. The absence of exteriorization of the parasite, in parasitic deadlock in humans, complicates direct diagnosis. Thus the search for toxocara larvae in the stool is always negative. Definitive diagnosis is based on the detection of these larvae in the CSF [23] or in the aqueous humor [24]. Larval debris can also be found in the histological examination of organ biopsies [25]. However, the benefit/risk ratio of these examinations strongly limits their use. Thus serology plays its full role in the diagnosis of toxocariasis. It is based on screening for the presence of serum antibodiesIgG: anti Toxocariasis Excretory-Secretory Antigens (TES) by Immuno-Enzymatic Method (ELISA). At this time, many kits are marketed offering good performance in terms of sensitivity varying between 80 and 91% and specificity between 86 and 93% [2]. However, the likelihood of cross-reactions, particularly with trichinae and eelworms, impacts the specificity of this method [26]. Thus, the immunoblot technique or western blot [2]. Reinforces this specificity and is used as a confirmation test in the event of positivity by ELISA technique. Patients with toxocariasis present a characteristic western-blot profile made up of 4 Low Molecular Weight (LMW) bands of 24, 28, 30 and 35 kDa, and a group of 3 High Molecular Weight (HMW) bands of 132, 147 and 200 kDa. Only the 4 low molecular weight bands are specific for toxocariasis [27]. In our patient, a positive screening for IgG-type anti-TES antibodies by ELISA technique was confirmed by western blot where the 4 LMW bands (24, 28, 30 and 35 kDa) were found. The significant seroprevalence of the carriage of residual antibodies indicating cured infections makes it difficult to interpret a positive result and does not provide the confirmation of an ongoing toxocariasis. Indeed, the negativation of anti-toxocara antibodies generally takes several years [28]. Thus the diagnosis of toxocariasis can only be conceived within the framework of a bundle of epidemiological, clinical, radiological and biological arguments. It is on this basis that the diagnosis was made in our patient.
With regard to the treatment of VLM, current recommendations are based on clinician experience and very few studies due to the relatively small number of patients identified with toxocariasis. Both albendazol and mebendazol are recommended, although albendazol has greater tissue penetration than mebendazol. The dose of albendazol is 10 mg/kg/day divided into two doses for five days. Ivermectin and diethylcarbamazine have also been tested and found to be equally useful [29]. Also, prednisone is often a complement to anthelmintics when there is an ocular involvement and surgery is reserved for the most serious cases.
The prognosis for VLM is generally good. However, the disease can affect cognitive development; potential correlations with epilepsy have been proven [30]. Other children may develop blindness, myocarditis, or even Henoch Schönlein’s purpura [31].
Thus, toxocariasis is preventable. Healthcare professionals should be aware of the symptoms of toxocariasis in order to educate patients and parents on all the ways to avoid infection [29]. Families who own dogs or cats should be encouraged to take their animals to the vet regularly for deworming, as these animals usually do not show symptoms of illness despite shedding Toxocara eggs. It is also important to encourage the community to collect and dispose of their pets’ excrement [30]. Children diagnosed with pica syndrome will require proper investigation and treatment of an underlying cause to decrease the risk of Toxocara infection. At last, promoting proper hand hygiene and teaching children not to eat dirt are all measures that will reduce the risk of ingesting Toxocara eggs [31].
Conclusion
Despite the remarkable progress made over the past two decades, toxocariasis continues to pose a significant challenge to public health. Toxocara infections in humans may remain clinically inapparent but may also induce serious disease. Research can advance understanding of toxocariasis in order to prevent its severe pictures and minimize their impact on society by acting on risk factors and on more advanced therapies.
References
- Fillaux J, Magnaval JF. Laboratory diagnosis of human toxocariasis. Vet Parasitol. 2013; 193: 327-336.
- Biomnis. Toxocarose. Précis de biopathologie. Analyses médicales spécialisées. Ivry sur Seine: Biomnis; 2013.
- Beaver PC, Snyder CH, Carrera GM, et al. Chronic eosinophilia due to visceral larva migrans; Report of three cases. Pediatrics. 1952; 9: 7-19.
- Rostami A, Ma G, Wang T, Koehler AV, Hofmann A, et al. Human toxocariasis - A look at a neglected disease through an epidemiological ‘prism’. Infect Genet Evol. 2019; 74: 104002.
- Thompson DE, Bundy DA, Cooper ES, et al. Epidemiological char acteristics of Toxocara canis zoonotic infection of children in a Caribbean community. Bull World Health Organ. 1986; 64: 283-290.
- Magnaval JF, Michault A, Calon N, et al. Epidemiology of human toxocariasis in La Réunion. Trans R Soc Trop Med Hyg. 1994; 88: 531-533.
- Marty AM. Toxocariasis. In: Meyers WM, Neafie RC, et al. editors, Pathology of infectious diseases. Washington, DC, Armed Forces Institute of Pathology. 2000; 411-421.
- Fan CK, Holland CV, Loxton K, Barghouth U. Cerebral toxocariasis: Silent progression to neurodegenerative disorders? Clin Microbiol Rev. 2015; 28: 663-686.
- Patel S, Kazura J. Toxocariasis. En Behrman R, Kliegman R, Jenson H (eds.). Nelson Tratado de Pediatría. 17.ª ed. Madrid: Elsevier; 2006:1164.
- Association française des enseignants de parasitologie et mycologie. Syndrome de Larva migrans. Lille: Université médicale virtuelle francophone; 2014.
- Jean-François Magnaval, Judith Fillaux, Richard Fabre, Diagnostic biologique de la toxocarose humaine,Revue Francophone des Laboratoires. 2014; 2014: 61-69.
- Shetty AK, DH Aviles. Nephrotic syndrome associated with Toxocara canis infection. Annals of tropical paediatrics. 1999; 19: 297-300.
- Dhayalini, Raj et al. Visceral Toxocariasis Presenting as Systemic-Onset Juvenile Idiopathic Arthritis.” Journal of tropical pediatrics. 2021; 67: fmab067.
- Hartleb M, Januszewski K. Severe hepatic involvement in visceral larva migrans. Eur J Gastroenterol Hepatol. 2001; 13: 1245–1249.
- Gupta A, Tripathy K. Ocular Toxocariasis. [Updated 2022 Feb 21]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022.
- Ubinsky-Elefant G, et al. “Human toxocariasis: Diagnosis, worldwide seroprevalences and clinical expression of the systemic and ocular forms.” Annals of tropical medicine and parasitology. 2010; 104: 3-23.
- Lim, J.H. Toxocariasis of the liver: Visceral larva migrans. Abdom Imaging. 2008; 33: 151–156. https://doi.org/10.1007/s00261-007-9325-y
- Azuma K, Yashiro N, Kinoshita T, Yoshigi J, Ihara N, et al. Atteinte hépatique de larva migrans viscérale due à Toxocara canis : Un rapport de cas - CT et MR résultats. Rayonner. Méd. 2002; 20: 89–92.
- Deshayes S, Bonhomme J, de La Blanchardière A. Neurotoxocariasis: A systematic literature review. Infection. 2016; 44: 565–574. https://doi.org/10.1007/s15010-016-0889-8
- Arevalo, J Fernando, et al. “Ocular toxocariasis.” Journal of pediatric ophthalmology and strabismus. 2013; 50: 76-86.
- Lee, Jin Young, et al. “The Prevalence of Toxocariasis and Diagnostic Value of Serologic Tests in Asymptomatic Korean Adults.” Allergy, asthma & immunology research. 2015; 7: 467-475.
- Magnaval JF, Glickman LT, Dorchies P. La toxocarose, une zoonose helminthique majeure. Rev Med Vet (Toulouse). 1994; 145: 611-627.
- Vidal JE, Sztajnbok J, Seguro AC. Eosinophilic meningoencephalitis due to Toxocara canis: Case report and review of the literature. Am J Trop Med Hyg. 2003; 69: 341-343.
- De Souza EC, Nakashima Y. Diffuse unilateral subacute neuroretinitis. Report of transvitreal surgical removal of a subretinal nematode. Ophthalmology. 1995; 102:1183-1186.
- Marty AM. Toxocariasis. In: Meyers WM, Neafie RC, et al. editors, Pathology of infectious diseases. Washington, DC, Armed Forces Institute of Pathology. 2000: 411-421.
- Jacquier P, Gottstein B, Stingelin Y, et al. Immunodiagnosis of toxocarosis in humans: Evaluation of a new enzyme-linked immunosorbent assay kit. J Clin Microbiol. 1991; 29:1831-1835.
- Roldán WH, Espinoza YA. Evaluation of an enzyme-linked immunoelectrotransfer blot test for the confirmatory serodiagnosis of human toxocariasis. Mem Inst Oswaldo Cruz. 2009; 104: 411-418.
- Magnaval JF, Glickman LT, Dorchies P, et al. Highlights of human toxocariasis. Korean J Parasitol 2001; 39: 1-11.
- Lee, Rachel M, et al. Toxocariasis in North America: A systematic review. PLoS neglected tropical diseases. 2014; 8: 8 e3116.
- Skulinova K, Novak J, Kasny M, Kolarova L. Seroprevalence of Larval Toxocarosis in the Czech Republic. Acta Parasitol. 2020; 65: 68-76.
- Fakhri, Y et al. Toxocara eggs in public places worldwide - A systematic review and meta-analysis. Environmental pollution (Barking, Essex : 1987). 2018; 242: 1467-1475.