
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A 7-year-old child presented with eosinophilic cystitis as the manifestation of hypereosinophilic syndrome: A case report
Neda Azin1; Mahsa Geravandi2; Mohammad Rasoul Golabchi2; Ali Hajihashemi2; Shokouh Sadeghizade2*
1Department of Radiology, Imam Hussein Children Hospital, Isfahan University of Medical Sciences, Isfahan, Iran.
2Department of Radiology, Isfahan University of Medical Sciences, Isfahan, Iran.
*Corresponding Author : Shokouh sadeghizade
Department of Radiology, Isfahan University of Medical Sciences, Isfahan, Iran.
Email: shokouhsadeghizade@gmail.com
Received : Apr 25, 2023
Accepted : May 19, 2023
Published : May 26, 2023
Archived : www.jcimcr.org
Copyright : © Sadeghizade S (2023).
Abstract
Background: Eosinophilic Cystitis (EC) is a rare condition in which the infiltration of eosinophils in the bladder wall causes transmural inflammation. The most common symptoms that occur as a result of mucosal injury consist of frequency, hematuria, dysuria, and suprapubic pain. We report a patient with EC as a manifestation of Hypereosinophilic Syndrome (HES) who is 7 years old girl with urinary symptoms and a mass-like lesion in the ultrasonography of the bladder.
Case presentation: A 7-year-old girl presented to the children’s hospital with sudden onset of dysuria and suprapubic tenderness accompanied by gross hematuria. Ultrasonography evaluation revealed marked, focal, and mass-like wall thickening. Cystoscopy revealed diffusely edematous and hyperemic mucosa without any focal mass. Biopsy showed infiltration of eosinophils mucosa and submucosa layers. Bone marrow aspiration revealed mildly hypocellular marrow and marked eosinophilia but was negative for malignancy. Subsequently, the patient was treated with prednisolone and Eosinophilia was dramatically reduced to 10%. After two weeks of admission, the patient was discharged with steroid slow tapering regimen. Follow-up after 6 months showed no evidence of any other organ involvement.
Conclusion: This is a rare bladder disorder that may be caused by HES. Children presenting with unexplained eosinophilia and urinary symptoms should be evaluated for EC, which may require a bladder biopsy for diagnosis, and HES should be considered in the workup of EC.
Keywords: Eosinophilic cystitis; Hypereosinophilic syndrome; Eosinophilia; Cystitis.
Citation: Azin N, Geravandi M, Golabchi MR, Hajihashemi A, Sadeghizade S, et al. A 7-year-old child presented with eosinophilic cystitis as the manifestation of hypereosinophilic syndrome: A case report. J Clin Images Med Case Rep. 2023; 4(5): 2431.
Background
Eosinophilic Cystitis (EC) is a rare condition in which the infiltration of eosinophils in the bladder wall causes transmural inflammation. fibrosis with or without muscle necrosis can also be seen in pathology specimens. This pathological condition was first described by Brown et al in 1960 [1]. EC is considered a localized form of systemic hypereosinophilic syndromes and allergic diseases [2]. Although it has been associated with various etiological factors such as allergy, bladder tumor, bladder trauma, parasitic infections, and chemotherapeutic agents, the definite cause of EC has remained unclear. EC is probably caused by the antigen-antibody reaction, which leads to the production of various immunoglobulins that cause the activation of eosinophils and initiate the inflammatory process [3]. The most common symptoms consist of frequency, hematuria, dysuria, and suprapubic pain [4]. Al though irregular wall thickening or tumor-like lesion is presented in ultrasonography [5], no imaging modalities are yet suggested for the definite diagnosis of EC. Inflamed, ulcerated, or necrotic mucosa, and sometimes polypoid areas or mass-like lesions may be seen in cystoscopy in suspected cases [6,7]. The main diagnostic tool for EC is the pathology, in which transmural infiltration of predominant eosinophils in the urinary bladder wall is seen [8]. However, involvement of the urinary bladder is relatively rare in both children and adults, we report a patient with EC as a manifestation of HES who is 7 years old girl with urinary symptoms and a mass-like lesion in the ultrasonography of the bladder.
Case presentation
A 7-year-old girl previously a healthy child presented to the children’s hospital. She reported sudden onset of dysuria and suprapubic tenderness accompanied by gross hematuria. No history of renal colic was present. She had no complaints of respiratory symptoms.
Her drug history was negative. Her parents denied any history of food or drug allergy.
In the physical exam, the general appearance was normal. Heart rate and respiratory rate were 85 beats/min and 15 breaths/min respectively. The temperature was 37°c and the blood pressure was 110/80 mmHg. There were no skin lesions or lymphadenopathy. Ears, nose, and throat were unremarkable. Pulmonary and cardiac examination revealed normal. The abdomen was soft without palpable masses. Suprapubic tenderness was present. An examination of other systems showed no abnormalities.
The complete blood count test findings were hemoglobin of 14.5 g/dl, white blood cell count of 12.4 × 103/μl with 13% eosinophils (0.75 × 103/μl), and platelet count of 28.7 × 104/μl. Blood Urea Nitrogen and serum Creatinine levels were in the normal range. The peripheral blood lymphocyte subpopulation showed 20% CD10+ cells, 4% CD34+ cells, 0.5% CD14+ cells, and 45% CD45+ cells. Urinalysis showed hematuria (Blood 2+ and red blood cell 40-50/HPF) without casts. The urinary culture was negative. Urine fluid cytology showed semi-turbid clearance with few eosinophils. The stool examination was negative for parasites or ova. Radioallergosorbent Test was negative for pollen, house dust mites, and animal dander.
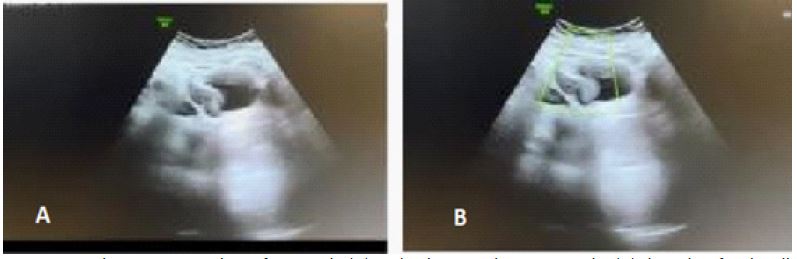
No pulmonary infiltration was detected in the chest X-Ray. Ultrasonography evaluation revealed marked, focal, and mass-like bladder wall thickening (Figure 1). Neither splenomegaly nor lymphadenopathy was detected. According to these data, Magnetic Resonance Urography was considered to evaluate the urinary system and congenital abnormalities.
It showed both kidneys in the renal fossa without evidence of parenchymal loss/infection, dysplasia, and cysts. Also, in the evaluation of upper urinary tracts no hydronephrosis, narrowing, or obstruction was detected. The shape of the bladder was irregular.
Irregular circumferential wall thickening of the bladder including submucosa and muscularis propria was seen with a maximum thickness of 14 mm with the abutment of both ureureterovesical junctions. (Figure 2) which had homogenous low signal intensity on T1/T2 (signal intensity same as muscle).
After contrast administration and Dynamic MRU in 3 minutes and 15 minutes revealed homogenous enhancement of the urinary bladder wall thickening the same as muscles, there was no obvious pathologic enhancement (Figure 3).
So, the next step was cystoscopy and tissue sampling of the bladder wall.
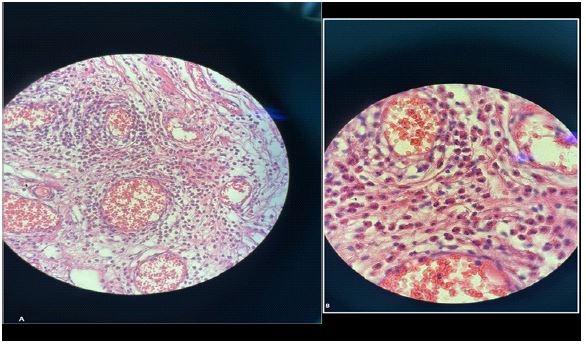
Cystoscopy revealed diffusely edematous and hyperemic mucosa without any focal mass. Biopsy showed mucosa and submucosa infiltration of eosinophils (Figure 4).
For more evaluation and to rule out malignancies, bone marrow aspiration was done. It revealed mildly hypocellular marrow and marked eosinophilia but was negative for malignancy.
According to the patient’s histopathologic findings and clinical presentation, she was diagnosed as having EC.
Due to the patients’ reflux, Upper gastrointestinal endoscopy was considered. It revealed active esophagitis with many eosinophilic infiltrations, also mild chronic inflammation with severe eosinophilic infiltrations in the stomach wall, and focal reactive gastropathy was detected. It showed negative for H. pylori bacteria.
Subsequently, the patient was treated with prednisolone. Eosinophilia was dramatically reduced to 5%. After two weeks of admission, the patient was discharged with steroid slow tapering regimen. Follow-up after 6 monthsshowed normal eosinophils count, urinary symptoms resolved, and no evidence of any other organ involvement.


Discussion
Hyper Eosinophilic Syndrome (HES) is a rare disease known as eosinophilia and multiple organ damage secondary to the release of eosinophilic mediators [9].
Hyper Eosinophilic Syndrome (HEs) criteria are:
Eosinophil count in complete blood count greater than 1.5 × 109/L (1500 cells/microL) in two distinct tests at least one month apart and/or tissue involvement by eosinophils in histopathology [10,11].
HES is a rare disease and is more common in males. Most patients are between 20-50 years [12].
We discuss a child girl who fulfills the diagnostic criteria of HES marked as eosinophilia and Eosinophilic Cystitis (EC).
So, we should consider other conditions that induce hypereosinophilia and similar symptoms. These include parasitic infections, allergic diseases, cancers, autoimmune diseases, and drug reactions. We should exclude these conditions before the final diagnosis of HEs [13].
Six classifications of HES are: myeloproliferative HES, lymphocytic HES, overlap HES, associated HES, familial HES, and idiopathic [14,15].
Overproduction of eosinophil causes the release of toxic granules products, lipid mediators such as sulfidopeptid leukotrienes, and cytokines like GM_CSF. Cytokines and chemokines, such as interleukins IL-5, IL-3, and granulocyte-macrophage colony-stimulating factor (GM-CSF) can induce degranulation and activation of Eos and organ damage [16-18].
The most common organs that HES can involve are the skin, GI, and respiratory tract [12].
The involvement of the urinary bladder is rare.
Eosinophilic Cystitis is a rare disorder that is difficult to diagnose because of the lack of specific symptoms or signs. The primary symptom is urinary tract infections, accompanied by dysuria and hematuria, and maybewith eosinophilia [19].
The etiology of EC is still unknown, but recent reports suggest a possible association between EC and allergic or hypersensitivity reactions [20].
Ultrasonography in eosinophilic cystitis showed irregular bladder wall thickening, mimicking mass so; the diagnosis of EC is typically made by histopathological examination of bladder biopsy specimens, revealing eosinophil infiltration in bladder wall stroma or mucosal tissue [21].
In similar studies, cross-sectional imaging such as CT scans has been used for more evaluation. However, in our case, due to the child patient and prevented exposure to radiation, MRU was used.
Our case report highlights the rarity and complexity of HES and EC. In the literature, we found reports of other cases with similar symptoms and diagnostic criteria to our patient. One case described a 56-year-old male with HES and EC who presented with hypereosinophilia, dysuria, and hematuria [22].
Another case report documented a 27-year-old male presenting with urinary symptoms and tetralogy Fallot was later diagnosed with HES and EC [23]. In contrast, our case report documents a 7-year-old girl with HES and EC, highlighting the range of ages at which HES can present.
In another article, a 4-year-old child with asthma and HES and EC; in contrast, our case doesn’t have a history of allergy and asthma [24].
Overall, the rarity and complexity of HES and EC highlight the need for further research in this area. Accurate and timely diagnosis and treatment are crucial in managing this condition and preventing organ damage.
Conclusion
In conclusion, EC is a rare bladder disorder, characterized by eosinophilic infiltration of the bladder wall, and may be caused by HES. Children presenting with unexplained eosinophilia and urinary symptoms should be evaluated for EC, which may require a bladder biopsy for diagnosis, and HES should be considered in the workup of EC.
Declarations
Acknowledgments: Not applicable.
Disclosures: The author(s) declared no potential conflicts of interest.
Authors’ contributations: All the authors have read and approved the final manuscript.
Funding: The author(s) received no financial support.
Availability of data and materials: Data sharing does not apply to this article as no datasets were generated or analyzed during the current study, but details from the clinical records are available from the corresponding author upon reasonable request.
Ethics approval and consent to participate: Ethics approval and patient consent were obtained.
Consent for publication: Consents was obtained.
References
- Brown EW. Eosinophilic granuloma of the bladder. J Urol. 1960; 83: 665-668.
- Sparks S, Kaplan A, DeCambre M, Kaplan G, Holmes N, et al. Eosinophilic cystitis in the pediatric population: a case series and review of the literature. J Pediatr Urol. 2013; 9: 738-744.
- Mosholt KS, Dahl C, Azawi NH. Eosinophilic cystitis: three cases, and a review over 10 years. BMJ Case Rep. 2014; 2014.
- He J, Ning F, Tu L, Hu J, Chen W, et al. Eosinophilic cystitis in children: A case report. Exp Ther Med. 2018; 16: 2978-2984.
- Li G, Cai B, Song H, Yang Z. Clinical and radiological character of eosinophilic cystitis. Int J Clin Exp Med. 2015; 8: 533-539.
- Hasan A, Abdel-Al I, Nafie K, Rashad MF, Abozied H, et al. Clinicopathological characteristics and outcomes of eosinophilic cystitis: A retrospective study. Ann Med Surg (Lond). 2021; 68: 102626.
- Popert RJ, Ramsay JW, Owen RA, Fisher C, Hendry WF, et al. Eosinophilic cystitis mimicking invasive bladder tumour: discussion paper. J R Soc Med. 1990; 83: 776-778.
- van den Ouden D. Diagnosis and management of eosinophilic cystitis: a pooled analysis of 135 cases. Eur Urol. 2000; 37: 386-394.
- Kojima K, Maeda J, Mikami S, Yamagishi H, Ide H, et al. Eosinophilic cystitis presented as a manifestation of hypereosinophilic syndrome: a case report and review of the literature. Nephron extra. 2013; 3: 30-35.
- Protheroe C, Woodruff SA, De Petris G, Mukkada V, Ochkur SI, et al. A novel histologic scoring system to evaluate mucosal biopsies from patients with eosinophilic esophagitis. Clinical Gastroenterology and Hepatology. 2009; 7: 749-755. e11.
- Nair P, Ochkur SI, Protheroe C, Simms E, Lee NA, et al. The identification of eosinophilic gastroenteritis in prednisone-dependent eosinophilic bronchitis and asthma. Allergy, Asthma & Clinical Immunology. 2011; 7: 1-5.
- Roufosse F, Klion AD, Weller PF. Hypereosinophilic syndromes: clinical manifestations, pathophysiology, and diagnosis. UpToDateUpToDateInc, Waltham http://www uptodate com Accessed. 2017; 17.
- Roufosse FE, Goldman M, Cogan E. Hypereosinophilic syndromes. Orphanet journal of rare diseases. 2007; 2: 1-12.
- Klion AD. How I treat hypereosinophilic syndromes. Blood, The Journal of the American Society of Hematology. 2015; 126: 1069-1077.
- Klion AD. Eosinophilia: A pragmatic approach to diagnosis and treatment. Hematology 2014, the American Society of Hematology Education Program Book. 2015; 2015: 92-97.
- Makiya MA, Herrick JA, Khoury P, Prussin CP, Nutman TB, et al. Development of a suspension array assay in multiplex for the simultaneous measurement of serum levels of four eosinophil granule proteins. Journal of immunological methods. 2014; 411: 11-22.
- Cardoso P, Elias C, Medas R, Cardoso L, Peixoto A, et al. Eosinophilic Colitis, an Uncommon Cause of Diarrhea: Case Report and Literature Review. GE-Portuguese Journal of Gastroenterology. 1-5.
- Valent P, Klion AD, Horny H-P, Roufosse F, Gotlib J, et al. Contemporary consensus proposal on criteria and classification of eosinophilic disorders and related syndromes. Journal of Allergy and Clinical Immunology. 2012; 130: 607-612. e9.
- Popescu OE, Landas SK, Haas GP. The spectrum of eosinophilic cystitis in males: case series and literature review. Archives of pathology & laboratory medicine. 2009; 133: 289-294.
- Hidoussi A, Slama A, Jaidane M, Zakhama W, Youssef A, et al. Eosinophilic cystitis induced by Bacillus Calmette-Guerin (BCG) intravesical instillation. Urology. 2007; 70: 591. e9-. e10.
- Mosholt KSS, Dahl C, Azawi NH. Eosinophilic cystitis: three cases, and a review over 10 years. Case Reports. 2014; 2014: bcr2014205708.
- Jiang P, Wang C, Jin B, Lin Y, Chen S, et al. Eosinophilic cystitis in a patient with hypereosinophila syndrome: A case report. Experimental and Therapeutic Medicine. 2014; 8: 49-51.
- Kojima K, Maeda J, Mikami S, Yamagishi H, Ide H, et al. Eosinophilic cystitis presented as a manifestation of hypereosinophilic syndrome: a case report and review of the literature. Nephron extra. 2013; 3: 30-35.
- Makol R, Hassoun Y, Abonia J. Eosinophilic cystitis as the first manifestation of hypereosinophilic syndrome. Annals of allergy, asthma & immunology. 2022; 129: s108.