
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 4
Iliopsoas hematoma, a complication of low-molecular-weight heparin use: About 2 cases
Mariem Mediouni*; Emna Allouche; Faten Boudiche; Habib Ben Ahmed; Wejdene Ouechtati; Leila Bezdah
Cardiology Department, Charles Nicolle Hospital, Tunisia.
*Corresponding Author : Mariem Mediouni
Cardiology Department, Charles Nicolle Hospital, Tunisia.
Email: mediounimariem@outlook.fr.
Received : Apr 26, 2023
Accepted : May 22, 2023
Published : May 29, 2023
Archived : www.jcimcr.org
Copyright : © Mediouni M (2023).
Abstract
Iliopsoas hematoma is an uncommon entity that may develop with Low-Molecular-Weight Heparin (LWMH) use. Here we report the cases of 2 patients who developed this complication. Both patients were admitted for an acute coronary syndrome and received antiplatelet therapy and subcutaneous low-molecular-weight heparin. A few days after their admission, they both developed iliopsoas hematomas revealed by sudden pain and acute anemia. One of these patients developed an infection of the hematoma. In both cases we opted for a conservative treatement under a close monitoring of vitals and biological parameters. Resolution of the hematomas was spontaneous.
These two cases highlight the importance of close monitoring of patients under LWMH therapy especially in association with antiplatelet therapy.
Keywords: Iliopsoas hematoma; Low-molecular-weight heparin; Anticoagulation; Coronary angiography.
Citation: Mediouni M, Allouche E, Boudiche F, Ahmed HB, Ouechtati W, et al. Iliopsoas hematoma, a complication of low-molecular-weight heparin use: About 2 cases. J Clin Images Med Case Rep. 2023; 4(5): 2433.
Introduction
Iliopsoas hematoma is a rare complication that may occur in association with anticoagulation treatment, coagulopathies or hemodialysis [1]. Heparin and vitamin K antagonists are the most commonly involved drugs. It can remain localized in the muscle or diffuse into the peritoneal or retroperitoneal space. Depending on its extension, it can be a life-threatening condition and sometimes fatal.
Here, we report the cases of two patients who developed iliopsoas hematoma during anticoagulant therapy.
Case presentations
Patient 1
A 51-year-old woman with a medical history of diabetes and hypertension was admitted in the ICU for a non-ST segment elevation Acute Coronary Syndrome (ACS). She has no personal or family history of coagulopathy, troke or trauma. Her initial systemic examination was unremarkable. She received a pretreatment with a loading dose of Clopidogrel, Aspirin and subcutaneous enoxaparin (1 mg/kg/12h). At day 4 past admission, she complained of sudden pain in the left flank and functional impotence of the left lower limb. She became febrile (39°C) with an altered general status and developed a biological inflammatory syndrome. A diverticular sigmoiditis was initially suspected. A CT angiography was performed showing an iliopsoas hematoma of 11.5 x 4 cm. Vital signs remained stable but a laboratory test showed that the hemoglobin levels had dropped from 13.2 g/dl to 9 g/dL within 24 hours. She needed a blood transfusion with red blood cells and anticoagulation was suspended. A control CT angiography was performed after 21 days showing a regression of the hematoma measuring 6 x 3.4 cm with signs of superimposed infection. The patient was treated with antibiotics.
Coronary angiography was performed 3 weeks after resolution of the hematoma showing a three-vessel disease and the patient underwent a coronary artery bypass graft.
Patient 2
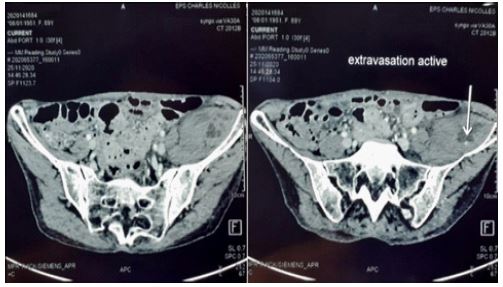
A 59-year-old smoker woman with medical history of chronic obstructive pulmonary disease was admitted to the emergency department for prolonged chest pain and EKG changes showing anterior myocardial infarction. She received a pretreatment with a loading dose of Clopidogrel, Aspirin and subcutaneous enoxaparin (30 mg IV bolus). We opted for a non-invasive reperfusion strategy because primary percutaneous coronary intervention could not be performed in a timely manner. The patient received successful fibrinolytic therapy. Coronary angiography with radial access was performed later showing a non-significant stenosis of the left ascending coronary artery and a cardiac MRI was scheduled. LMWH at the dose of 1 mg/kg/12h was continued for 5 days. At the fifth day, the patient started complaining of abdominal pain. The left groin and flank were painful at palpation. The passive motion of her hip aggravated the pain. Abdominal computed tomography scan revealed a left iliopsoas hematoma of 14 x 15 mm with active bleeding (Figure). Laboratory investigation revealed a hemoglobin level of 8.3 g/dl. Packed red blood cells were administered and LMWH was discontinued. The hematoma resolved spontaneously after a few days.
Discussion
Spontaneous iliopsoas hematoma is a rare but potentially life threatening complication of anticoagulant therapy [1,2]. Clinical presentation may include abdominal, back or groin pain, positive psoas sign, the presence of a palpable iliac mass, femoral nerve palsy or hemodynamic instability [3]. It may cause reversible or permanent damage to the femoral nerve as reported by multiple cases [1,4,5]. The infectious complication of this hematoma worsens its prognosis. Risk factors for bleeding under LMWH are the elderly, hemodialysis, coagulopathies and concomitant use of antithrombotic therapy [4]. Both our patients were under dual antiplatelet therapy and LMWH.
The diagnosis may be confirmed by echography but Computed Tomography (CT) is the most used tool [6-8]. MRI may also provide better visualization of the iliac psoas compartment.
The optimal treatment remains controversial. The initial steps consist of discontinuation of anticoagulant agents, transfusion therapy, volume resuscitation and supportive measures in hemodynamically unstable patients. Treatment options mainly include conservative therapy, ultrasound or CT guided percutaneous drainage and decompression, embolization, surgical incision and drainage, and retroperitoneal laparoscopy [9,10]. In our cases, a conservative treatment was successfully adopted with a full recovery.
Conclusion
Iliopsoas hematoma is a rare complication of anticoagulation. It can be a fatal condition. Therefore, patients undergoing treatment with heparin should be closely monitored and early diagnosis of the hematoma is very important for an optimal management.
References
- Wada Y, Yanagihara C, Nishimura Y. Bilateral iliopsoas hematomas complicating anticoagulant therapy. Intern Med Tokyo Jpn. 2005; 44: 641-643.
- Türk EE, Verhoff MA, Tsokos M. Anticoagulant-related iliopsoas muscle bleeding leading to fatal exsanguination: Report of two autopsy cases. Am J Forensic Med Pathol. 2002; 23: 342-344.
- Guivarc’h M. [Hematoma of the iliac psoas muscle. 29 cases]. J Chir (Paris). 1997; 134: 382-389.
- Llitjos JF, Daviaud F, Grimaldi D, Legriel S, Georges JL, et al. Ilio-psoas hematoma in the intensive care unit: A multicentric study. Ann Intensive Care. 2016; 6: 8.
- Marquardt G, Barduzal Angles S, Leheta F, Seifert V, et al. Spontaneous haematoma of the iliac psoas muscle: A case report and review of the literature. Arch Orthop Trauma Surg. 2002; 122: 109-111.
- Lenchik L, Dovgan DJ, Kier R. CT of the iliopsoas compartment: Value in differentiating tumor, abscess, and hematoma. AJR Am J Roentgenol. 1994; 162: 83-86.
- Conesa X, Ares O, Seijas R. Massive psoas haematoma causing lumbar plexus palsy: A case report. J Orthop Surg Hong Kong. 2012; 20: 94-97.
- Weiss JM, Tolo V. Femoral nerve palsy following iliacus hematoma. Orthopedics. 2008; 31: 178.
- Murakami T, Nobukawa Y, Tabata M, Ueda M, Yasuda Y, Suzuki H, et al. [Two cases of atraumatic iliopsoas hematoma]. Masui. 2007; 56: 1214-1216.
- Won DY, Kim SD, Park SC, Moon IS, Kim JI, et al. Abdominal compartment syndrome due to spontaneous retroperitoneal hemorrhage in a patient undergoing anticoagulation. Yonsei Med J. 2011; 52: 358-361.