
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Differentiating gout and calcium pyrophosphate
deposition disease: Role of imaging
Farah Nadiah Sulaiman*; Nurul Aulia Zakaria; Tan Chou Luan; Ng Boon Han; Surendran Ramasamy; Wan Rosmaiza Wan Musa; Liza Mohd Isa; Nor Shuhaila Shahril
Division of Rheumatology, Department of Internal Medicine, Hospital Putrajaya, Malaysia.
*Corresponding Author : Farah Nadiah Sulaiman
Division of Rheumatology, Hospital Putrajaya, Jalan P9, Presint 7, 62250 Wilayah Persekutuan Putrajaya, Malaysia.
Email: farahnadiah84@gmail.com
Received : Apr 28, 2023
Accepted : May 23, 2023
Published : May 30, 2023
Archived : www.jcimcr.org
Copyright : © Sulaiman FN (2023).
Abstract
75-year-old Chinese lady with diabetes mellitus, hypertension and history of bilateral knee arthroplasty was diagnosed with gouty arthritis for 14 years following recurrent ankle and knee pain and had normal serum uric acid level. She was given low dose allopurinol, colchicine and non-steroidal anti-inflammatory drugs and the disease controlled with only intermittent flare episodes. She was referred to rheumatology clinic after an acute gout flare precipitated by infection. She had arthritis at both wrists and left third Proximal Interphalangeal (PIP) joint with tenderness over the left wrist. No tophi were found. There were calcifications noted in the hand and knee radiographs while ultrasound showed hyperechoic deposits. No double contour sign seen. Joint aspiration for crystal confirmation was not feasible. The patient was treated for acute Calcium Pyrophosphate (CPP) arthritis with colchicine and Etoricoxib. She had complete resolution of symptoms and was subsequently able to taper off allopurinol.
Keywords: Calcium pyrophosphate deposition disease; Pseudo-gout; Calcinosis; Hyperechoic deposits.
Citation: Sulaiman FN, Zakaria NA, Luan TC, Han NB, Ramasamy S, et al. Differentiating Gout and Calcium Pyrophosphate Deposition Disease: Role of Imaging. J Clin Images Med Case Rep. 2023; 4(5): 2435.
Introduction
Calcium Pyrophosphate (CPP) crystal arthritis or Calcium Pyrophosphate Deposition (CPPD) disease is known for its similarity with gout in terms of its clinical presentation. However, it can be differentiated on imaging through plain radiograph or ultrasound. We demonstrate a case of an elderly lady who was treated initially as gouty arthritis in whom the diagnosis had been revised to polyarticular CPP-related arthritis, highlighting the imaging findings in this condition.
Case presentation
A 75-year-old Chinese lady was referred to rheumatology clinic for an acute gout flare after an episode of right leg cellulitis. Further history revealed that she was diagnosed with gouty arthritis for past 14 years when she presented with recurrent bilateral ankle and knee joint pain which usually resolved after three to five days with colchicines. These attacks were not precipitated by high purine diet. She had undergone bilateral knee arthroplasty one year prior to the onset of the joint pain. Serum uric acid level was recorded as 225 μmol/L upon diagnosis of gout at the primary care clinic. She was commenced on allopurinol 150 mg od and colchicine. Over the years, there was intermittent episodes of joint pain over the knees, ankle and wrist which improved with non-steroidal anti-inflammatory drugs or colchicine despite maintaining serum uric acid level of less than 360 μmol/L. Past medical history included diabetes and hypertension, and was treated with metformin, vildagliptin, losartan and amlodipine.
Musculoskeletal examination revealed warmth and swellingof both wristsand left third PIP joint withtender left wrist. Bilateral lower limbs demonstrated genu varus (Figure 1) with crepitus both knees. No tophi were found.
Investigations revealed raised erythrocyte sedimentation rate 43 mm/hr (1-10 mm/hr) while C-reactive protein was normal. Her serial serum uric acid level was 266 μmol/L. Her serum creatinine, calcium, magnesium and thyroid function test were normal.

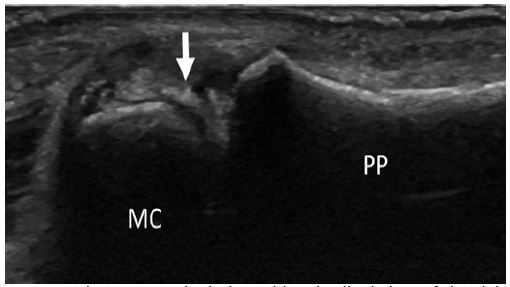
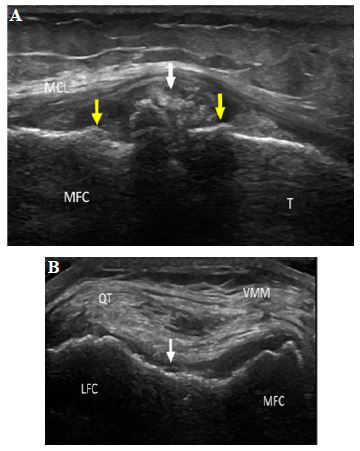
Hand radiograph showed calcifications over right second Metacarpophalangeal (MCP) joint, left fifth MCP joint, and Triangular Fibrocartilage Complex (TFCC) bilaterally. Both radiocarpal and proximal intercarpal joint spaces were narrowed. Knee radiograph revealed meniscal calcification (Figure 2). Ultrasound showed hyperechoic deposits of the bilateral wrist joints and right second MCP joint (Figure 3). There were hyperechoic linear aggregates within the cartilage both knee joints, but no double contour sign seen (Figure 4A-B). Joint aspiration for crystal confirmation was not performed as the effusion was minimal.
The patient was treated as acute flare of CPP arthritis with colchicine 0.5 mg twice daily and Etoricoxib 120 mg daily for 5 days which led to complete resolution of symptoms. Allopurinol was subsequently stopped. There were no further flares on subsequent clinic visits.

Discussion
This case presentation illustrates an elderly lady diagnosed and treated as gouty arthritis but had recurrent symptoms despite normal serum uric acid. The diagnosis was revised to CPPD disease based on chondrocalcinosis from radiographs and musculoskeletal ultrasound findings.
CPPD disease is a crystal arthritis that is due to deposition of calcium pyrophosphate in the articular tissue, most commonly hyaline cartilage, or fibrocartilage [1]. It has slight predominance in male with age prevalence higher as it increases, reaches almost 50% in patients age of more than 84 years old [2,3].
Symptoms of CPPD disease is almost similar to gouty arthritis, however the joint pain in CPPD disease is less intense compared to acute gout. CPPD disease is associated with medications such as bisphosphonate infusion and intraarticular hyaluronic acid injection, metabolic condition such as hypercalcemia, hypomagnesemia, haemochromatosis, hyperparathyroidism, and previous trauma [4]. This patient had history of arthroplasty prior to onset of pain which can be a precipitating factor for acute CPP arthritis.
The similarity between gouty arthritis and CPP arthritis frequently leads to misdiagnosis, and it was proven in a study done by Wolfe et al in 1991 [9]. In this study, from 9,108 new patients in rheumatology clinic, 1.8% had been incorrectly diagnosed as having gout in the community which revised diagnosis mainly psoriatic arthritis and pseudogout. From the incorrectly diagnosed patients, 76% of them received allopurinol.
Definitive diagnosis of CPPD is by identification of CPP crystals in synovial fluid, or occasionally in biopsied tissue [1]. However, this weakly positive birefringent crystal is not easily recognized under the microscope due to low concentrations of crystals, or because of the very small size of the crystal which easily missed in the microscope [5].
Conventional radiographic features in CPPD disease differ from gouty arthritis as it involves mostly articular tissue such as hyaline cartilage, fibrocartilage, synovium, capsule, and ligament while gout mostly affect para-articular structures such as tendons, ligaments and bursae [6]. The most common feature is chondrocalcinosis, which can have mono- or polyarticular distribution, mostly detected in the knee joint followed by wrist, hip, and symphysis pubis [3,7]. Nevertheless, chondrocalcinosis cannot be used as a sole criterion for CPPD diagnosis without clinical arthritis.
Chondrocalcinosis on ultrasound may appear as punctate or linear aggregates, described as hyperechoic linear deposits in the middle layer of synovium or meniscus. In contrast, double contour sign which occur due to deposition of Monosodium Urate (MSU) crystal on top of the hyaline cartilage have been described in gout [5,8]. Chondrocalcinosis in CPPD disease however does not generate posterior acoustic shadow as in gout [8]. The typical hyperechoic deposits of CPPD disease over the knee joint, TFCC and metacarpophalangeal joints were demonstrated on musculoskeletal ultrasound of this patient.
Conclusion
The similarities of CPPD disease with gouty arthritis can pose a challenge in the diagnosis and management in primary care setting. Imaging via radiographs or musculoskeletal ultrasound may aid in diagnosis of the two conditions.
Conflict of interest: There is no conflict of interest to disclose in this study.
References
- Zhang W, Doherty M, Bardin T, Barskova V, Guerne PA, Jansen T, et al. EULAR evidence-based recommendations for calcium pyrophosphate deposition. Part I: Terminology and diagnosis. Ann Rheum Dis. 2010; 69: 93.
- Hameed M, Turkiewicz A, Englund M, Jacobsson L, and Kapetanovic MC. Prevalence and incidence of non-gout crystal arthropathy in southern Sweden. Arthritis Res Ther. 2019; 21: 291.
- Rosenthal AK, Ryan LM. Calcium Pyrophosphate Deposition Disease. N Engl J Med. 2016; 374: 2575-2584.
- Brown SR, Cohen AM. Pseudogout: Uncommon and Under-Recognized. Osteopathic Family Physician. 2019; 6: 11.
- Swan A, Amer H, Dieppe P. The value of synovial fluid assays in the diagnosis of joint disease: A literature survey. Ann Rheum Dis. 2002; 61: 493-498.
- Omoumi P, Zufferey P, Malghem J, So A. Imaging in Gout and Other Crystal-Related Arthropathies. Rheum Dis Clin N Am. 2016; 42: 621–644.
- Abhishek A, Doherty S, Maciewicz R, Muir K, Zhang W, Doherty M, et al. Chondrocalcinosis is common in the absence of knee involvement. Arthritis Res Ther. 2012; 14: R205.
- Jung MY, Kim HR. Ultrasonographic Assessment in Crystal-induced Arthritis.Korean J Med. 2015; 89: 632-643.
- Wolfe F, Cathey MA. The misdiagnosis of gout and hyperuricemia. J Rheumatol. 1991; 18: 1232-1234.