
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Diagnosis of congenital bronchobiliary fistula in children by
bilirubin crystallization in the bronchoalveolar lavage fluid:
A case report and literature review
Guangli Zhang1; Chongjie Wang1; Zhil Wang1; Xiaoyin Tian1; Yuanyuan Li1; Qinyuan Li1; Xiujuan Xu1; Hao Ding2; Jin Zhu3; Jian Luo1; Zhengxiu Luo1*
1Department of Respiratory Medicine, Children’s Hospital of Chongqing Medical University, National Clinical Research Center for Child Health and Disorders, Ministry of Education Key Laboratory of Child Development and Disorders, Chongqing Key Laboratory of Pediatrics, Chongqing 400010, China.
2Department of Radiology, Children’s Hospital of Chongqing Medical University, China.
3Department of Pathology, Children’s Hospital of Chongqing Medical University, China.
*Corresponding Author : Zhengxiu Luo
Department of Respiratory Medicine, Children’s Hospital of Chongqing Medical University, National Clinical Research Center for Child Health and Disorders, Ministry of Education Key Laboratory of Child Development and Disorders, Chongqing Key Laboratory of Pediatrics, Chongqing 400010, China.
Email: luozhengxiu816@hospital.cqmu.edu.cn
Received : May 01, 2023
Accepted : May 25, 2023
Published : Jun 01, 2023
Archived : www.jcimcr.org
Copyright : © Luo Z (2023).
Abstract
Background: Congenital Bronchobiliary Fistula (CBBF) is a rare disease with abnormal connection between the biliary tract and the bronchus. The misdiagnosis rate of CBBF is high, delayed surgery may induce poor outcome.
Case presentation: We reported a girl with CBBF who was confirmed via bronchoscopy and chest Computed Tomography (CT). The girl was 7-month-old admitted to the hospital with “recurrent pneumonia”. Bilirubin crystallization detection was positive in the Broncho Alveolar Lavage Fluid (BALF). CT images showed the abnormal traffic between the biliary tract and the right main bronchus, the girl was diagnosed with CBBF and recovered after surgical operation.
Literature search: A total of 27 cases were collected, 14 (51.8%) cases were diagnosed in the neonatal period, 9 (33.3%) patients were diagnosed in infancy. CBBF was more common in female (19/27, 70.3%). The specific manifestations were bilious sputum (24/27, 88.9%) and bilious vomiting (7/27, 22.2%). Recurrent pneumonia (9/27, 33.3%) was common clinical manifestations. The most abnormal fistula originates different location around the carina was right main bronchus (21/27, 77.8%). There were 23(85.2%) cases recovered after surgical operation and 4(14.8%) cases with severe comorbidities/complications died.
Conclusions: CBBF should be suspected in infants with bilious sputum. Bronchoscopy plays crucial role in preoperative evaluation and postoperative follow-up. With early diagnosis and surgery, the prognosis is quite well for CBBF patients without severe biliary malformation and/or severe postoperative complications.
Keywords: Congenital Bronchobiliary Fistula (CBBF); bronchoalveolar lavage fluid; bilirubin crystallization; children; case report.
Citation: Zhang G, Wang C, Wang Z, Tian X, Luo Z, et al. Diagnosis of congenital bronchobiliary fistula in children by bilirubin crystallization in the bronchoalveolar lavage fluid: A case report and literature review. J Clin Images Med Case Rep. 2023; 4(6): 2438.
Background
Congenital Bronchobiliary Fistula (CBBF) refers to the abnormal traffic between the biliary system and the bronchial tree. CBBF is a rare disease and easily misdiagnosed as pneumonia or other diseases in clinical practice, which resulting in delayed treatment and worse outcomes [1,2]. Few studies have reported the role of bilirubin crystallization detection in the Broncho Alveolar Lavage fluid (BALF) for diagnosis CBBF [3]. Here, we reported an infant with recurrent pneumonia who admitted to Children`s hospital, Chongqing Medical University. She was diagnosed with CBBF combined positive bilirubin crystallization detection in BALF with related chest CT images and recovered after surgery. The detection of bilirubin crystallization in BALF plays important diagnostic value in patients suspected with CBBF [3,4]. Surgery is the first choice for CBBF patients [3-6]. Next, we collected literature about patients with CBBF so as to further improve the recognition and early intervention.
Case presentation clinical data
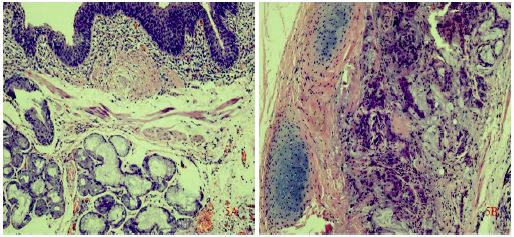
A 7-month-old girl was admitted to respiratory department with persistent wet cough and recurrent wheezing. She was diagnosed with recurrent pneumonia and treated with antibiotics, bronchodilators and glucocorticoids empirically when symptoms worsen. She was full-term with normal manifestation during perinatal period. She occasionally expectorated bright-yellow sputum when drinking breast or milk (Figure 1). Chest Computed Tomography (CT) images showed an abnormal bronchial bifurcation originated from the right main bronchus (Figure 2A). Both transverse (Figure 2B) and anamorphic (Figure 2C) chest CT indicated gas shadow anterior to the esophagus at the diaphragm level. Yellow, serous secretions emerging from an anomalous orifice located at the right main bronchus via bronchoscopy (Figure 3). The bright-yellow BALF was obtained and tested for bilirubin with positive detection. The contrast agent meglumine was injected through the anomalous orifice via flexible bronchoscope. Chest CT examination showed the contrast agent entered the abnormal bronchus and traveled downward, passing through the left hepatic duct, the common hepatic duct and common bile duct (Figure 4). The girl was diagnosed with Congenital Broncho Biliary Fistula (CBBF) based on these findings. She had operation to remove the anomalous fistula. During the ten months following-up, the girl was absent from wet cough, wheezing and pneumonia. Chest computed tomography examination demonstrated that the anomalous orifice and lung shadow disappeared (Figure 2D). Bronchoscopy showed an anomalous diverticulum (Figure 3C) and the BALF was colorless with no bilirubin presented. Pathological examination showed tubular structure of cartilage and muscle, lined with stratified squamous epithelium, pseudostratified columnar ciliated epithelium and submucosal glands (Figure 5).

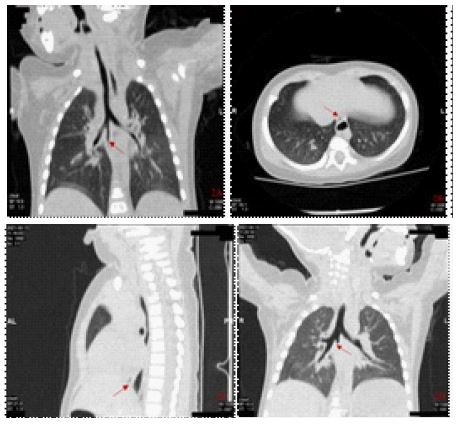
B: Transverse view showed a gas shadow in front of the esophagus at the level of the diaphragm (red arrow);
C: Loss of shape showed the diaphragm with gas shadow in front of the esophagus (red arrow);
D: Airway reconstruction showed tubular shadow disappeared with a blind end after surgery (red arrow)
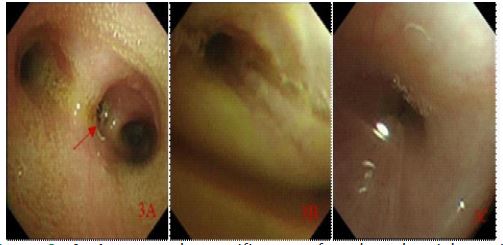
B: Yellow secretions from the anomalous orifice (before surgery);
C: an anomalous diverticulum after surgery.
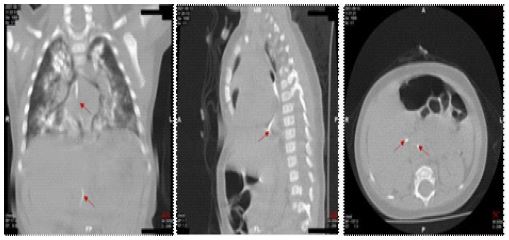
B: The contrast agent entered the abnormal bronchus and traveled down through the diaphragm (red arrow).
C: Cross-sectional view showed the inflow of contrast agent into the common bile duct and common hepatic duct (red arrows).
Literature review
Information sources and search key words
Using the search terms “congenital bronchobiliary fistula” OR “bronchobiliary fistula”, Medline (via PubMed), Embase and web of science databases, China National Knowledge Infrastructure (CNKI) and Wan fang were searched. We also searched Chinese Medical Care Repository, searches for relevant articles were performed with the following items: “congenital bronchobiliary fistula” OR “bronchobiliary fistula. Searches were limited to articles published in English till March 31, 2022.
Eligible criteria
Inclusion
Congenital bronchobiliary fistula patients, not restricted by age, gender, disease course, race, region and other factors;
Exclusion:
1) Secondary bronchobiliary fistula patients;
2) Article not published in Chinese or English;
3) In vitro and in vivo studies;
4) Conference abstracts;
5) Full-text or data cannot be extracted Searching results
Searches of literatures initially identified 1149 potentially relevant records. Following review of the title and abstract, 1051 records were excluded, and a further 73 duplicated records were excluded, 25 records were included. Therefore, 19 English articles and 6 Chinese articles were included, a total of 26 cases [4-28]. Combined with 1 case in this article, a total of 27 cases of CBBF were enrolled. The clinical data summary table is shown in Table 1.
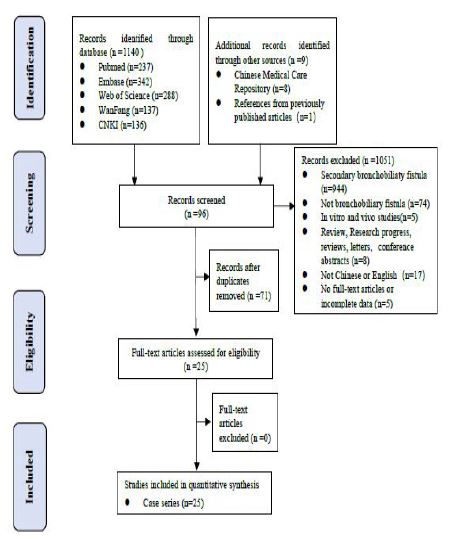
Table 1: All cases of congenital bronchobiliary fistula reported to data.
| N | Year | Author | Type of fistula | Age | Sex | Diagnositc method | Comorbidity | Operative method | Therapeutic effects |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 2021 | Meng EY et al | Right main bronchus | 3d | F | Bronchoscopy and CT | biliary atresia | Surgical excision and ligation + Roux En-Y anastomosis | Survived |
| 2 | 2021 | Wang Q et al | Right intermediate bronchus | 7 yr 6 mo | F | Bronchoscopy and MRI | None | Surgical excision and ligation | Survived |
| 3 | 2019 | Wu XM et al | Right intermediate bronchus | 3 yr 5 mo | F | Bronchoscopy and CT and SPECT | None | Surgical excision and ligation | Survived |
| 4 | 2018 | Chen X et al | Right main bronchus | 3 yr 7 mo | F | Bronchoscopy and MRCP | None | Bioadhesive occlusion | Followed for 4 yr 3 mo, normal |
| 5 | 2013 | Li K et al | Right main bronchus | 27 d | F | Bronchoscopy and CT | Extrahepatic biliary atresia | Surgical excision and ligation +Fistula distal- jejunal Roux En-Y anastomosis | Followed for 3 mo, normal |
| 6 | 2010 | Ge Y et al | Right main bronchus | 51 yr | F | CT | None | Surgical excision and ligation | Survived |
| 7 | 2021 | Bing Z et al | Right main bronchus | 2 yr | M | Bronchoscopy and CT | None | Surgical excision and ligation | Followed for 2 yr 6 mo, normal |
| 8 | 2021 | Thuong Vu et al | Right main bronchus | 2 m | F | Bronchoscopy and CT | None | Surgical excision and ligation | Survived |
| 9 | 2019 | Li TY et al | Right main bronchus | 5 d | F | Bronchoscopy and CT and ultrasound | None | Surgical excision and ligation | Followed for 4 mo, normal |
| 10 | 2016 | Na KJ et al | Right main bronchus | 17 yr | M | Bronchus examination and CT and MR imaging | None | Laparoscopic resection and ligation | Followed for 10 mo, normal |
| 11 | 2009 | Günlemez et al | Left main bronchus | 9 d | F | CT | Extrahepatic biliary atresia | Surgical excision and ligation | Followed for 9 mo, Normal |
| 12 | 2004 | Hourigan et al | Right main bronchus | 13 d | M | MRI | Biliary Dysplasia | Right thoracotomy + Kasia procedure | Survived |
| 13 | 2002 | DiFiore et al | Right main bronchus | < 28 d | M | Intuition intraoperatively | Right diaphragmatic hernia | Surgical removal +right diaphragmatic hernia repair | Survived |
| 14 | 1994 | Ferkol et al | Left main bronchus | 23 d | M | Bronchus examination | Biliary dysplasia | Surgical excision and ligation | Died |
| 15 | 1993 | Gauderer et al | Bilateral main bronchus | 3 w | F | Bronchoscopy and angiography | None | 3 times thoracotomy (fistula clipping et al) + the hepatic left lobe resection | Followed for 8 yr, survived |
| Left main bronchus | 1 y | F | Bronchoscopy and hepatobiliary scintigraphy | None | Surgical excision and ligation and Roux En-Y anastomosis | Followed for 6y, normal | |||
| 16 | 1990 | Yamaguchi et al | Right main bronchus | 32 yr | M | Bronchus examination | None | Surgical excision and ligation | Survived |
| 17 | 1988 | de Carvalho et al | Right main bronchus | 32 yr | F | CT | None | Surgical excision and ligation | Followed for 1 yr, normal |
| 18 | 1986 | Lindahl et al | Right main Bronchus | 15 d | F | Bronchus examination | None | Surgical excision and ligation | Survived |
| 19 | 1985 | Chang et al | 12 h | M | Bronchus examination | None | Surgical excision and ligation | Survived | |
| 20 | 1984 | Chan et al | Right main bronchus | 4 d | F | Not mentioned | Biliary Dysplasia | Surgical excision and ligation | Died |
| 21 | 1976 | Kalayoglu et al | Right main bronchus | 4 d | F | Surgical findings | Esophageal atresia Tracheoesophageal fistula | Surgical excision and ligation | Died |
| 22 | 1971 | Sane et al | Right main bronchus | 4 wk | F | Bronchus examination | None | Surgical excision and ligation | Survived |
| 23 | 1970 | Wagget et al | Left main Bronchus | 3 wk | F | Bronchus examination | None | Surgical excision and ligation | Survived |
| 24 | 1968 | Weitzman et al | Right main Bronchus | 2 yr 9 mo | M | Bronchus examination | None | Surgical excision and ligation | Survived | 25 | 1952 | Neuhauser et al | Right main bronchus | 5 mo | F | Bronchus Examination and CT | None | No surgery | Died |
Discussion
CBBF is a rare disease with congenital abnormal connection between the hepatic duct and trachea or bronchus. The age of onset and severity of symptoms depend on the diameter of the fistula.
Therefore, the symptoms appear at any age from newborn to adults [9,10,29]. Typical clinical feature of CBBF is bilious sputum or bile-stained sputum in tracheal intubation. Patients usually have chronic wet coughing, recurrent wheezing, shortness of breath and growth retardation [12]. CBBF has usually been misdiagnosed as an esophagotracheal fistula, gastroesophageal reflux, aspiration pneumonia, tracheoesophageal fistula or high intestinal obstruction [30,31].
In 1952, Neuhauser et al [29] reported the first case of CBBF. Up to now, 27 cases have been enrolled in English and Chinese (Table 1). Among them, fourteen (51.8%) cases were diagnosed in the neonatal period, nine (33.3%) were diagnosed in infancy, four (14.8%) were diagnosed in puberty or adulthood. The common manifestations were biliary sputum (24/27, 88.9%), recurrent pneumonia (9/27, 33.3%) and bilious vomiting (7/27, 22.2%). CBBF was more common in female (19/27, 70.3%). The abnormal fistula originates different location around the carina: right main bronchus (21/27, 77.8%), left main bronchus (3/27, 11.1%), right intermediate bronchus (2/27, 7.4%), and bilateral main bronchus (1/27, 3.7%).
The mechanism of CBBF formation is not clearly clarified. However, there are two possible speculated mechanisms. One is considered as the duplication of the upper gastrointestinal tract, which growing between the laryngotrachea and hepatic diverticulum; the other is believed to be the fusion between abnormal bronchial buds and abnormal bile ducts [20,26]. The pathological results in our case consistent with the latter pathogenesis.
The detection of bilirubin crystallization in sputum or/and BALF plays crucial role in CBBF diagnosis [4,5,11-14,29,31]. Furthermore, abnormal fistula was easily found via bronchoscopy. In this case, the bilirubin detection was positive in the BALF and the location of the fistula connection was confirmed via bronchoscopy and fistula angiography, which provided more comprehensive information and was verified intraoperatively.
Chest CT and airway reconstruction, MRI or isotope examination can find an abnormal fistula from the trachea, through the diaphragm, into the abdominal cavity, and liver lobes communicate with each other [15]. Intraoperative management of fistula could base on preoperative isotope examination [32]. Liu AH et al [31] indicated gas accumulation in the lumen of the right hepatic duct and the gallbladder lumen by hepatobiliary B-ultrasound, which provided clues for clinical diagnosis of BBF.
Patients with CBBF are ineffective to routine treatment and require operation to remove the fistula. If the bile drainage is normal, only thoracic fistula resection can be performed [33,34]; there also has reports of resection of thoracic and abdominal fistulas [13]. Fistula-jejunostomy Roux-en- Y anastomosis, hilar-jejunostomy, or Cholecystojejunostomy can be performed to fully drain bile so as to avoid fistula recurrence for cases with biliary malformation, such as absence of common bile duct, abnormal bile-intestinal drainage [14].
As surgery has higher cost and more damage, interventional therapy is alternative for CBBF patients without severe biliary malformation. The bronchial occlusion with biological glue has achieved good results in the treatment of adult respiratory diseases [35,36]. Tissue glue occlusion via bronchoscopy also have been used in the treatment of adult secondary bronchobiliary fistulas [36-38]. Chen X et al [7] successfully cured the pediatric patient with congenital brachobiliary fistula for the first time via bronchoscopy. The interventional treatment via bronchoscopy in patients with bronchobiliary fistula requires respiratory intervention doctors to achieve further breakthroughs in future.
Combined this case and literature review, twenty-three (85.2%) patients recovered after operation, four (14.8%) patients died from severe comorbidities (biliary dysplasia (n=1), biliary atresia (n=1), congenital diaphragmatic hernia (n=1), esophageal atresia and/or tracheoesophageal fistula (n=1)). Two cases had complications (pneumothorax (n=1), septicemia (n=1)). One case with no surgery. CBBF patients with delayed or no operation, severe biliary malformation, or severe postoperative complications have poor prognosis [17,23,24,28].
Conclusion
In conclusion, CBBF should be suspected in infants with bilious sputum. Besides, bronchoscopy plays crucial role in preoperative evaluation and postoperative follow-up. With early diagnosis and surgery, the prognosis is good for CBBF patients without severe biliary malformation and/or severe postoperative complications.
Declarations
Authors’ contributions: Conception and design: GL Z, ZX L; Administrative support: ZX L, J L; Bronchoscopy and bronchoscopic figures: CJ W, GL Z; Provision of study materials or patients: ZL W, XY T, YY L, QY L, XJ X; Imaging and pathological figures: H D, J Z; Manuscript writing: GL Z, ZX L; Final approval of manuscript: All authors.
Funding: No founding sources.
Availability of data and materials: Not applicable.
Declarations Ethics: All procedures performed in studies involving human participant was in accordance with the ethical standards of the Children’s Hospital of Chongqing Medical University research committee. Consent for publication.
Consent form: An informed consent was signed by the patient’s mother who agreed to publish this case.
Competing interests: No competing interests for all authors.
References
- Cheng AC, Chen HW, Chen PJ, Huang TY, Lin JC, et al. Bronchobiliary Fistula. Intern Emerg Med. 2021; 16: 1093-1094.
- Huang ZM, Zuo MX, Gu YK, Lai CX, Pan QX, et al. Bronchobiliary fistula after ablation of hepatocellular carcinoma adjacent to the diaphragm: Case report and literature review. Thorac Cancer. 2020; 11: 1233-1238.
- Zhang N, Chen Y, Tang L, Zhou D, Hou T, et al. Diagnosis of bronchobiliary fistula by bilirubin crystallization in the alveolar lavage fluid case reports and literature review. Ann Pallliat Med. 2021; 10: 7121-7125.
- Meng EY, Xia L, Shang HL, Dong HF, Shang LH, et al. A Case of neonatal congenital broncho-biliary fistula with biliary atresia and literature review. He Nan Medical Research. 2021; 30: 4842-4847.
- Wang Q, Chen M, Jin R, Sun YF, Xu H, et al. Case report of congenital broncho- bileduct fistula. Clin J Appl Clin Pediatr. 2021; 36: 67-69.
- Wu XM, Chen YJ, Pang WB, Huang JS, et al. A case report of congenital bronchobiliary fistula and miss diagnosis [ J] . J Clin Ped Surg. 2019; 18: 429-431.
- Chen X, Yan YQ, Deng WH, Ren JH, Shu JH, et al. Congenital tracheobiliary fistula treated with biological glue plugging under bronchoscopic guidance: A case report and literature review. Clin J Appl Clin Pediatr. 2018; 33: 839-841.
- Li K, Zheng S, Xiao XM, Cao Y, Wang LS. Neonatal congenital broncho-biliary fistula- A case report and literature review. Clin J Pediatr Surg. 2013; 34: 447-449.
- Ge Y, Wu JL, Zhang TT, Tan QW, Zheng B, et al. A case of ongenital biliary bronchial fistula. 2010; 44: 556.
- Bing Z, Chen R, Xing P, et al. Congenital Bronchobiliary Fistula A Case Report and Literature Review [J]. Front Pediatr. 2021; 9: 686827.
- Thuong Vu L, Minh Duc N, Tra My TT, Tan Lien Bang M, Tuan Linh L, et al. Congenital bronchobiliary fistula a case report and literature review. Respirol Case Rep. 2021: 9: e00731.
- Li TY, Zhang ZB. Congenital bronchobiliary fistula A case report and review of the literature. World J Clin Cases. 2019; 7: 881-890.
- Na KJ, Jung JC, Hwang Y, Lee HJ, Park IK, et al. Minimally Invasive Surgical Repair for Congenital Bronchobiliary Fistula in an Adult. Ann Thorac Surg. 2016; 101: 1584- 1587.
- Günlemez A, Tugay M, Elemen L, Türker G, Gürcan NI, et al. Surgical experience in a baby with congenital broncho-biliary fistula. Ann Thorac Surg. 2009; 87: 318-320.
- Hourigan JS, Carr MG, Burton EM, Ledbetter JC. Congenital bronchobiliary fistula: MRI appearance. Pediatr Radiol. 2004; 34: 348-350.
- DiFiore JW, Alexander F. Congenital bronchobiliary fistula in association with right-sided congenital diaphragmatic hernia. J Pediatr Surg. 2002; 37: 1208-1209.
- Ferkol T, Mc Dowell KM, Gauderer MW, Alpert SE. Sinopulmonary manifestations of congenital bronchobiliary fistula. Clin Pediatr (Phila). 1994; 33: 181-184.
- Gauderer MW, Oiticica C, Bishop HC. Congenital bronchobiliary fistula: Management of the involved hepatic segment. J Pediatr Surg. 1993; 28: 452-455.
- Yamaguchi M, Kanamori K, Fujimura M, Watanabe Y, Matsuda T, et al. Congenital bronchobiliary fistula in adults. South Med J. 1990; 83: 851-852.
- de Carvalho CR, Barbas CS, Guarnieri RM, de Campos JR, Filomeno LT, et al. Congenital bronchobiliary fistula: First case in an adult. Thorax. 1988; 43: 792-793.
- Lindahl H, Nyman R. Congenital bronchobiliary fistula successfully treated at the age of three days. J Pediatr Surg. 1986; 21: 734-735.
- Chang CC, Giulian BB. Congenital bronchobiliary fistula. Radiology. 1985; 156: 82.
- Chan YT, Ng WD, Mak WP, Kwong ML, Chow CB, et al. Congenital bronchobiliary fistula associated with biliary atresia. Br J Surg. 1984; 71: 240-241.
- Kalayoğlu M, Olcay I. Congenital bronchobiliary fistula associated with esophageal atresia and tracheoesophageal fistula. J Pediatr Surg. 1976; 11: 463-464.
- Sane SM, Sieber WK, Girdany BR. Congenital bronchobiliary fistula. Surgery. 1971; 69: 599-608.
- Wagget J, Stool S, Bishop HC, Kurtz MB. Congenital bronchobiliary fistula. J Pediatr Surg. 1970; 5: 566-569.
- Weitzman JJ, Cohen SR, Woods LO, Chadwick DL. Congenital bronchobiliary fistula. J Pediatr. 1968; 73: 329-334.
- Neuhauser EB, Elkin M, Landing B. Congenital direct communication between biliary system and respiratory tract. AMA Am J Dis Child. 1952; 83: 654-659.
- Pathak S, Jethi S, Saoji R. Isolated congenital tracheobiliary fistula. Indian Pediatr. 2018; 55: 995-996.
- Wilson NA, Douglas ZH, Briden K, Witt R, Lodhi HS, et al. Video-assisted Thoracoscopic Resection of a Congenital Tracheobiliary Fistula in a Neonate Technical Report and Review of the Literature. Surg Laparo Endo Per. 2021; 32: 266-271.
- Liu AH, Zhao SY, Wang W. Congenital biliary bronchial fistula A case report and literature review. Chinese Remedies & Clinics. 2018; 18: 2015-2017.
- Yuan L, Yang H, Yang J, Ma D. Congenital tracheobiliary fistula shown on 99mTc-EHIDA hepatobiliary scintigraphy. Clin Nucl Med. 2016; 41: 164-166.
- Kim JS, Suh JH, Park CB, Yooh JS. Congenital tracheobiliary fistula in an adolescent patient [J]. Ann Thorac Surg. 2015; 99: 328-331.
- Pérez CG, Reusmann A. Congenital broncho-biliary fistula: A case report [J]. Arch Argent Pediatr. 2016; 114: e350-e353.
- Kondo N, Hashimoto M, Takuwa T, Matsumoto S, Okumura Y, et al.Treatment of bronchial fistula after extraplural pneumonectomy using flexible bronchoscopy with the administration of OK432, fibroblast growth factor basic and fibrin glue sealant. Gen Thorac Cardiovasc Surg. 2020; 68: 1562-1564.
- Mukkada RJ, Antony R, Francis JV, Chettupuzha AP, Augustine P, Venugopal B, et al.
- Bronchobiliary fistula treated successfullu with endoscopic microcoils and glue [J]. Ann Thorac Surg. 2014; 98: e33-e34.
- Yu Lee-Mateus A, Garcia-Saucedo JC, Abia-Trujillo D, Kroner PT, Gomez V, et al.
- Bronchobiliary Fistula Management With Bronchoscopic Occlusive Stenting and Fibrin Glue Instillation. J Bronchology Interv Pulmonol. 2022; 29: e49-e51.
- Lee S, Lee JH, Kim HB, Lee IJ. Percutaneous Bronchial Embolization to Treat Intractable Bronchobiliary Fistula. Cardiovasc Inter Rad. 2019; 42: 784-786.