
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
The dangerous safety pin: Melioidosis
Aashna Gandhi1*; Shivraj Hunge2; Yogya Jha3; Geethu Joe4; Rajeev Soman5
1ID Fellow, Department of Infectious Diseases, Jupiter Hospital, Pune, India.
2Consultant Neurologist, Department of Neurology, Jupiter Hospital, Pune, India.
3Consultant Physician, Department of General Medicine, Jupiter Hospital, Pune, India.
4Consultant Microbiologist, Department of Microbiology, Jupiter Hospital, Pune, India.
5HOD & Consultant ID Physician, Department of Infectious Diseases, Jupiter Hospital, Pune, India.
*Corresponding Author : Aashna Gandhi
ID Fellow, Department of Infectious Diseases, Jupiter Hospital, Pune, India.
Tel: +919870018310;
Email: aashnagandhi2206@gmail.com
Received : May 01, 2023
Accepted : May 30, 2023
Published : Jun 06, 2023
Archived : www.jcimcr.org
Copyright : © Gandhi A (2023).
Abstract
Melioidosis, although endemic, is often misdiagnosed and underreported in India. This is a case report of a 36 year old male patient, who was thought to have a head injury and aspiration pneumonia, and was ultimately diagnosed to have melioidosis, based on peculiar clinical, radiological and microbiological characteristics.
Citation: Gandhi A, Hunge S, Jha Y, Joe G, Soman R. The dangerous safety pin: Melioidosis. J Clin Images Med Case Rep. 2023; 4(6): 2443.
Introduction
Melioidosis is endemic in many parts of India but it is many a time underreported and misidentified. It is a disease that involves multiple organ systems and is often called the ‘great mimicker’ as illustrated by this case [1].
Case presentation
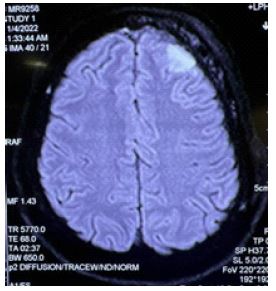
A 36 year old male patient, presented to our centre with a generalized tonic clonic seizure. He had a history of head injury with a seatbelt in his car, 6 days before this presentation. On admission, he was vitally stable but was in a post- ictal drowsy state. Except for a raised total leucocyte count, rest of the routine investigations were normal. An MRI was performed, which was reported as a left frontal lobe subdural hematoma (Figure 1).
A routine chest X ray done showed bilateral infiltrates, therefore an HRCT was performed. The HRCT revealed multiple patchy consolidations, admixed with random nodules, some of which had coalesced, in both the lungs, thought to be aspiration pneumonia (Figure 2). An ID opinion was sought for the same.
A review of history by the ID team revealed the following: The injury with seatbelt in the car 6 days before admission was trivial, and headache and generalized tonic clonic seizure had followed after 6 days of the injury. The HRCT was inconsistent with aspiration pneumonia as there was bilateral lung involvement, with predominantly upper zones involved, and nodules, of which some had coalesced. He also had a history of fever for the last 15-20 days, therefore, blood cultures were ordered.
Blood cultures flagged positive for gram negative bacilli. The patient was from the community and had not been exposed to antibiotics before. Therefore, the first suspicion for community acquired gram negative bacilli was Salmonella spp. However, this did not explain the rest of the clinical and radiological features. To hasten the process of identification, a blood culture identification panel (Multiplex PCR) was ordered which was negative and since Salmonella spp is included in the panel, an off-panel organism was suspected.
Blood culture was identified by Vitek2 susceptibility automated system as Burkholderia pseudomallei. Gram Stain showed typical ‘safety pin’ appearance (Figure 3) and the colony morphology resembled ‘carrom coin’ (Figure 4), as described in literature.



The isolate was subjected to various biochemical tests, three-disk diffusion test (colistin, gentamicin, amoxicillin-clavulanic acid), monoclonal antibody based latex agglutination and PCR assay targeting T3SS1 gene; which confirmed the identity of the organism.
This led us to review the history again. The patient was a diabetic and a chronic alcohol user. He hailed from the Konkan region (which has abundance of paddy fields), and had visited the same a month ago, when there were heavy rains. He was from the community, and had never been hospitalized before nor had he received any antibiotics.

An MRI with contrast was done after the clinical condition stabilized. It revealed a subdural empyema (Figure 5).
Therefore, the patient was diagnosed as bacteremic melioidosis with pulmonary + neurological involvement. He was started on Inj. Ceftazidime 2g IV TDS + Tab Co-trimoxazole 800/160 2-1-2. The patient improved significantly and was discharged on Tab Co-trimoxazole.
Discussion
Melioidosis is a disease endemic to tropical regions like Southeast Asia, Northern Australia and South Asia. South Asia makes up 44% of the global burden [1]. The predisposing factors include Diabetes mellitus, alcoholism, chronic lung disease, HIV, chronic kidney disease, chemotherapy for malignancy and exposure to soil [2]. Numerous organ systems are involved in melioidosis and therefore is rightly called ‘the great mimicker’ [1]. Some of the clinical manifestations mentioned in literature include pneumonia, skin infections, genitourinary infections, bacteremia without an evident clinical focus, soft tissue abscess, septic arthritis, neurological disease and osteomyelitis [3]. An unusual presentation is subdural empyema, without parenchymal involvement, as seen in our patient. A similar case has also been reported by Saravu et al [4]. The varied clinical presentations and low sensitivity of cultures mean that some patients have to be treated empirically if a strong clinical suspicion exists and other diagnoses are ruled out [5]. This organism also gets vastly misidentified in microbiology laboratories by automated systems like Vitek2. Common organisms that can mimic it are Burkholderia cepacia and Pseudomonas spp. Therefore, it is important to confirm the identity of a suspicious isolate with various biochemical tests, three disc diffusion test using colistin, gentamicin and amoxicillin-clavulanic acid (Burkholderia pseudomallei is intrinsically resistant to colistin, gentamicin and susceptible to amoxicillin- clavulanic acid) and antigen detection tests like latex agglutination and PCR (targeting T3SS1 gene) [6]. The treatment of melioidosis depends on the severity of illness. In the intensive phase, non-critically ill patients can be treated with Inj Ceftazidime 50 mg/kg upto 2 g IV 6-8 hourly while in critically ill patients, meropenem 25 mg/kg upto 1 g IV 8 hourly or imipenem 25 mg/kg upto 1 g 6 hourly can be used [7]. The drug of choice in the eradication phase is co-trimoxazole, at a dose of 320 mg of the trimethoprim component twice a day for adults >60 kg. Co-trimoxazole can be used in combination during intensive phase in non-pulmonary, difficult to penetrate foci. The minimum duration of intensive phase is 2 weeks and eradication phase is 3 months, but needs to be much longer in neurological, osteoarticular and vascular sites. Clinical suspicion, performance of correct tests and using appropriate treatment are often incredibly rewarding in the management of this disease.
References
- Mohapatra PR, Mishra B. Burden of melioidosis in India and South Asia: Challenges and ways forward. The Lancet Regional Health-Southeast Asia. 2022.
- K Saravu, C Mukhopadhyay, S Vishwanath, R Valsalan, M Docherla, et al. Melioidosis in southern India: epidemiological and clinical profileSoutheast Asian J Trop Med Public Heal. 2010; 41: 401-409
- Currie BJ, Mayo M, Ward LM, Kaestli M, Meumann EM, et al. The Darwin Prospective Melioidosis Study: a 30-year prospective, observational investigation. The Lancet Infectious Diseases. 2021; 21: 1737-1746.
- Saravu K, Kadavigere R, Shastry AB, Pai R, Mukhopadhyay C, et al. Neurologic melioidosis presented as encephalomyelitis and subdural collection in two male labourers in India. The Journal of Infection in Developing Countries. 2015; 9: 1289-1293.
- Soman R, Davda K, Sunavala A, Chhatwani C, Doshi A. experiences with empiricism in melioidosis. Sri Lankan Journal of Infectious Diseases. 2017; 7.
- Gupta A, Siddiqui F, Purwar S, Joshi R, Mukhopadhyay C, et al. Is it always COVID-19 in acute febrile illness in the tropics during the pandemic?
- Simpson AJ, Suputtamongkol Y, Smith MD, Angus BJ, Rajanuwong A, et al. Comparison of imipenem and ceftazidime as therapy for severe melioidosis. Clinical Infectious Diseases. 1999; 29: 381-387.