
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Naevo-cellular nevus of pregnancy mimicking melanoma
Sokaina Chhiti1*; Hanane Baybay1; Fatimazahra Hashas1; Zakia Douhi1; Meryem Soughi1; Sara Elloudi1; Fatimazahra Mernissi1; Mouna Rimani2
1Department of Dermatology, University Hospital Hassan II Fez, Morocco.
2Hassan Pathological Anatomy Center, Rabat, Morocco.
*Corresponding Author : Sokaina Chhiti
Department of Dermatology, University Hospital Hassan II Fez, Morocco.
Email: sokaina.chhiti@usmba.ac.ma
Received : May 03, 2023
Accepted : May 30, 2023
Published : Jun 06, 2023
Archived : www.jcimcr.org
Copyright : © Chhiti S (2023).
Abstract
Introduction: It is a common opinion that expansion and darkening in melanocytic nevi may occur during pregnancy. The main problem is that whether is an usual finding, or it is a condition that requires suspicion about melanoma.
Case report: We report the story of a patient with a pigmented lesion of the abdomen that changed in size and color during pregnancy mimicking melanoma.
Discussion: During the pregnancy, widening in diameters and structure changes of nevi may be seen especially on the front of the body. We also think that these findings might be connected with expansion of the skin during pregnancy. Dermoscopic controls are the first choice of method to analysis the nevi since the patient may not recognize these changes.
Conclusion: Dermoscopic data of melanocytic nevi in pregnancy are very limited and related to small groups of women.
Keywords: Neavi; Pregnancy; Melanoma; Dermoscopy.
Citation: Chhiti S, Baybay H, Hashas F, Douhi Z, Soughi M, et al. Naevo-cellular nevus of pregnancy mimicking melanoma. J Clin Images Med Case Rep. 2023; 4(6): 2444.
Introduction
Gestation is accompanied by clinical, dermoscopic and histological changes in benign nevi. The distinction between melanoma and nevus during pregnancy is a diagnostic challenge. Cancers rarely coexist with pregnancy; however, cutaneous melanoma remains a fortunately rare reality. We present a case of a nevus mimicking a melanoma during pregnancy.
Observation
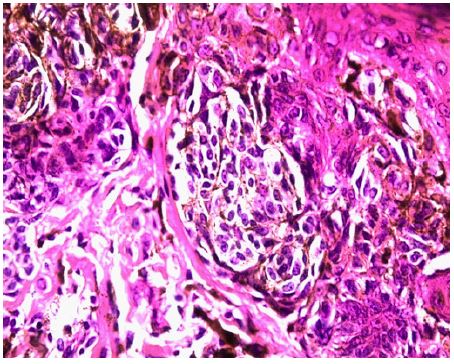
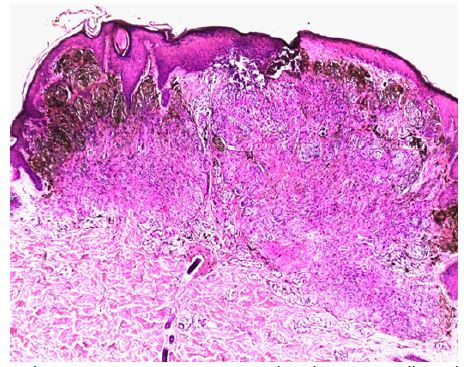
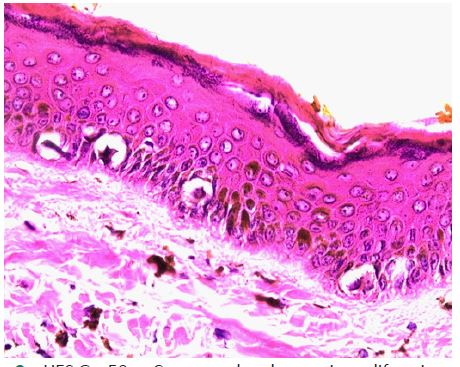
A young 30-year-old patient, with no history, a month and a half postpartum, consulted for a pigmented lesion of the abdomen evolving from childhood, increasing in size during her pregnancy. Clinical examination found a well-defined 0.5 cm pigmented papule resting on a poorly-defined erythematous plaque with irregular contours at the suspubian level below the cesarean section scar (Figure 1a). Dermoscopy showed an irregular peripheral pigmented network, a blue/white veil, an erythematous background and an ink spot (Figure 1b). The diagnosis of a melanoma was evoked and an excisional biopsy revealed the diagnosis of a tuberous compound neavo-cellular neavus (Figure 1a) with non-atypical melanocytic cells and without mitotic activity (Figure 2b) associated with a basal lentiginous junctional activity without pagetoid migration (Figure 2c).


Discussion
The rapid growth or change in size and color of a melanocytic tumor must be interpreted with the greatest caution, especially in certain situations, notably adolescence and pregnancy, which constitute favorable ground for maximum clinical and dermoscopic modification thanks to effects of sex and growth hormones as well as stretching of the skin at this period of life [1-3].
The distinction between the benign or malignant nature of a melanocyte lesion, during pregnancy, represents a real diagnostic challenge based essentially on clinical data, dermoscopy, confocal microscopy and histology.
It has been reported that during pregnancy approximately 90% of women will experience skin changes including changes in moles [4]. The association between pregnancy and melanoma has been a hot topic for many years with reports supporting the idea that pregnancy increases the risk of melanoma [5]. While single case reports of development of melanoma during pregnancy [6] can be found in the literature, several studies also support the idea that pregnancy is not a risk factor for the development of melanoma [7,8]. It seems that localized nevi in the abdomen and breast as well as melanomas are those that can grow most rapidly during pregnancy [9].
A meta-analysis noted dermoscopic changes in globular, reticular, and vascular patterns with architectural disorganization during this period, but this should not be interpreted as an ever-worrying fact. However, in case of diagnostic doubt, the use of histology becomes essential to have a definitive diagnosis. In the study by Strumia, it was noted that nevi with a globose pattern developed more peripheral brown blood cells and the studies by Rubegni et al. [10] and Gunduz et al. [11] also mention changes and increase in the number of dots and globules [9]. The presence of peripheral dots and globules observed at dermatoscopy is usually a sign of nevus growth [12]. At a young age, however, these observations related to the pregnancy could also result from mechanical distention of the skin resulting in upward movement of the base. Layer with junctional or dermal nests becoming more easily visible by dermatoscopy [9].
In our case, the clinic and the dermatoscopy were highly suggestive of melanoma, but the history of the disease and the histology had confirmed the benign nature of the lesion.
Conclusion
According to our experience, in front of a melanocytic lesion which changes during pregnancy, although we have malignancy criteria in dermoscopy, we must also think of the possibility of a benign melanocytic nevus, even if it becomes phenotypically atypical, with carrying out a pathological examination if strong suspicion.
Declarations
Consent: The examination of the patient was conducted according to the Declaration of Helsinki principles.
Conflicts of interest: The authors do not declare any conflict of interest.
References
- Cosgarea I, Trevisan-Herraz M, Ungureanu L, Zalaudek I. Dermatoscopic Features of Naevi During Pregnancy-A Mini Review. Front Med (Lausanne). 2021; 8: 727319.
- Slominski A, Tobin DJ, Shibahara S, Wortsman J. Melanin pigmentation in mammalian skin and its hormonal regulation. Physiol Rev. 2004; 84: 1155-1228.
- Ellis DL, Wheeland RG. Increased nevus estrogen and progesterone ligand binding related to oral contraceptives or pregnancy. J Am Acad Dermatol. 1986; 14: 25-31.
- Kumari R, Jaisankar TJ, Thappa DM. A clinical study of skin changes in pregnancy. Indian J Dermatol Venereol Leprol. 2007; 73: 141.
- Sanchez JL, Figueroa LD, Rodriguez E. Behavior of melanocytic nevi during pregnancy. Am J Dermatopathol. 1984; 6: 89-91.
- Sato T, Ishiko A, Saito M, Tanaka M, Ishimoto H, Amagai M. Rapid growth of malignant melanoma in pregnancy. J Dtsch Dermatol Ges. 2008; 6: 126-129.
- 13. Martins-Costa GM, Bakos R. Total body photography and sequential digital dermoscopy in pregnant women. Dermatol Pract Concept. 2019; 9: 126-131.
- Pennoyer JW, Grin CM, Driscoll MS, Dry SM, Walsh SJ, et al. Changes in size of melanocytic nevi during pregnancy. J Am Acad Dermatol. 1997; 36: 378-382.
- Strumia R. Digital epiluminescence microscopy in nevi during pregnancy. Dermatology. 2002; 205: 186-187.
- Rubegni P, Sbano P, Burroni M, Cevenini G, Bocchi C, et al. Melanocytic skin lesions and pregnancy: digital dermoscopy analysis. Skin Res Technol. 2007; 13: 143-147.
- Gunduz K, Koltan S, Sahin MT, Filiz EE. Analysis of melanocytic naevi by dermoscopy during pregnancy. J Eur Acad Dermatol Venereol. 2003; 17: 349-351.
- Fikrle T, Pizinger K, Szakos H, Panznerova P, Divisova B, et al. Digital dermatoscopic follow-up of 1027 melanocytic lesions in 121 patients at risk of malignant melanoma. J Eur Acad Dermatol Venereol. 2013; 27: 180-186.