
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Cases of severe hypotension caused by prone position
in patients with scoliosis: A case report
Yan Zhang1; Shu Lin1,2,3*; He-fan He1*
1Department of Anesthesiology, The Second Affiliated Hospital of Fujian Medical University, Quanzhou, Fujian Province, China.
2Group of Neuroendocrinology, Garvan Institute of Medical Research, 384 Victoria St, Sydney, Australia.
3Centre of Neurological and Metabolic Research, The Second Affiliated Hospital of Fujian Medical University, Quanzhou, Fujian Province, China.
*Corresponding Author : Shu Lin, He-fan He
Department of Anesthesiology, The Second Affiliated Hospital of Fujian Medical University, Quanzhou, Fujian Province, China.
Tel: 86-15659068071; Tel:86-15860905262
Email: shulin1956@126.com;
15860905262@163.com
Received : May 05, 2023
Accepted : May 31, 2023
Published : Jun 07, 2023
Archived : www.jcimcr.org
Copyright : © Shu Lin, He-fan He (2023).
Abstract
Introduction: We hope to provide useful experience for clinical workers about the solutions to the critical situation of severe hypotension in scoliosis surgery.
Materials and methods: Hypotension was prevented by using Kocher’s forceps to lift the exposed vertebral body and then rotating the staple to relieve body pressure on the stent, thereby relieving right ventricular outflow tract obstruction and ensuring a safe blood pressure level.
Results: We lifted the exposed part of the vertebral body using Kocher forceps and completed the operation. The tube was successfully removed, and the patient was sent back to the ward. Eventually, the patient recovered and was discharged.
Conclusions: We propose a solution to assist in completing the procedure by lifting the patient’s body with Kocher forceps. It is hoped that this case will provide a reference significance for clinicians.
Keywords: Hypotension; Scoliosis; Case report; Prone position.
Abbreviations: TEE: Transesophageal Echocardiography.
Citation: Zhang Y, Lin S, He HF. Cases of severe hypotension caused by prone position in patients with scoliosis: A case report. J Clin Images Med Case Rep. 2023; 4(6): 2445.
Introduction
Scoliosis is a common skeletal disorder. Clinically, this procedure generally uses the prone position, but this integration will cause hemodynamic changes, such as severe hypotension. The causes of hypotension are complex and diverse, and there is no good solution in a clinic for the most part. Stable arterial blood pressure is one of the critical factors for a smooth operation. Therefore, the cases we report can provide experience for a wide range of physicians.
Cases of profound hypotension [1] and hemodynamic collapse [2] have been described in pediatric scoliosis patients undergoing spinal surgery. We report a child with scoliosis who had unexpected severe hypotension due to prone position during thoracolumbar fusion via an elective posterolateral spinal approach. In addition, we propose a simple method to solve the problem of forced suspension of surgery due to severe hypotension during surgery. We hope that this case will arouse the attention and thinking of anesthesiologists and provide experience to surgeons.
Written consent for publication was obtained from the patient’s legal guardian.
Case presentation
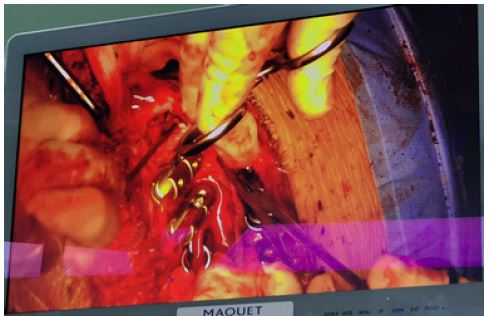
A 12-year-old female (weight 46 kg and height 156 cm) underwent surgical treatment for idiopathic thoracolumbar scoliosis. Her medical and past history was unremarkable except for decreased activity resistance. Radiographs taken showed a Cobb angle of 95 (Figure 1), and a thoracolumbar fusion via a posterolateral spinal approach with robot assistance was proposed. Upon arrival in the operating room, we performed routine monitoring and pre-operative procedures. Before the start of surgery, the patient received intravenous midazolam. They were induced with triamcinolone, sufentanil, and etomidate and intubated three minutes later. The central venous pressure was measured after the right internal jugular vein puncture using an infusion of propofol and remifentanil as maintenance. Autologous blood was recovered, and a blower insulation blanket was used to maintain the patient’s temperature during the operation. After the patient turned to the prone position, her cardiovascular and respiratory states were normal and stable during the induction period. However, during the operation, two severe drops in blood pressure (as low as about 40 mmHg) and increased heart rate occurred suddenly, and the amount of bleeding during the operation reached 300 ml. For the first time, we adopted blood transfusion and fluid replacement measures, inputting four units of red blood cells, 1500 ml of crystal solution, and continuous pumping of norepinephrine. After that, blood pressure recovered to the point when anesthesia began. The second time, the blood pressure suddenly dropped again. We took the same measures, but the situation did not improve, forcing the surgery to suspend. During the pause, we found that, without any action, the descending blood pressure gradually increased. Therefore, we thought about how to solve the problem of severe hypotension during the operation. Finally, we lifted the exposed part of the vertebral body using Kocher forceps (Figure 2) and completed the operation. The tube was successfully removed, and the patient was sent back to the ward.

Discussion
Various methods have been proposed to prevent severe hypotension during surgery, such as an operating table or stent dedicated to the prone position [3], to reduce bleeding from the surgical site, transesophageal echocardiography (TEE) [1] was used during the operation to monitor the ventricular size and function in real-time. This case illustrates the severe hemodynamic instability that can occur in patients undergoing surgery to rectify scoliosis. Causes of hemodynamic instability include massive blood loss, anaphylactic shock, pulmonary embolism, prone position, and surgical procedures. Through our professional judgment, intraoperative hypotension caused by excessive bleeding, hypovolemia, allergic reactions, and pulmonary embolism can be excluded. After the vertebral body was lifted with the Kocher forceps, the staple was rotated to reduce the pressure of the body on the support frame, thereby relieving the obstruction of the right ventricular outflow tract and ensuring the smooth return of venous blood. The operation was completed. Case reports are indicating that special stents are beneficial in spinal surgery and reducing bleeding at the surgical site [4], but they may also have a significant impact on the patient’s hemodynamics and respiratory function, resulting in reduced preload and cardiac output. It has also been reported that TEE can well monitor the ventricular condition [5], but it is necessary to find a probe that matches the patient. In conclusion, there is no gold standard to address intraoperative hypotension clinically.
Our case puts forward the solution when severe hypotension occurs during the operation and the blood pressure cannot be recovered by conventional fluid replacement, providing a new idea for surgeons, and also causing anesthesiologists to think about intraoperative management: We should carry out TEE to guide surgery during the operation, pay more attention to observing the patient’s abnormalities, and timely communicate with surgeons for early detection of problems.
Conflicts of interest: Yan Zhang, Shu Lin and He-fan He declare no confict of interest.
References
- Soliman DE, Maslow AD, Bokesch PM, Strafford M, Karlin L, et al. Transoesophageal echocardiography during scoliosis repair: Comparison with CVP monitoring. Can J Anaesth. 1998; 45: 925-932.
- Bagshaw ON, A Jardine. Cardiopulmonary complications during anaesthesia and surgery for severe thoracic lordoscoliosis. Anaesthesia. 1995; 50: 890-892.
- Anderton JM. The prone position for the surgical patient: a historical review of the principles and hazards. Br J Anaesth. 1991; 452-463.
- Yuen VMY, BFM Chow, MG. Irwin. Severe hypotension and hepatic dysfunction in a patient undergoing scoliosis surgery in the prone position. Anaesth Intensive Care. 2005; 393-399.
- Abcejo AS, Soto JD, Castoro C, Armour S, Long TR. Profound Obstructive Hypotension From Prone Positioning Documented by Transesophageal Echocardiography in a Patient With Scoliosis. A & A Case Reports. 2017; 9: 87-89.