
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Review Article - Open Access, Volume 4
Characterization of oral-derived neural crest-derived stem cell
populations (oNCSCs) in the teeth: Therapeutic potential for
bone tissue engineering
T Fritsch1,2 ; MA Vukovic3 ; Wolf-D Grimm 1,2,3 *
1Salzburg NAM Research Institute, Austria.
2DGParo Clinical Competence Center Bayerisch Gmain, Germany.
3DGParo Clinical Competence Center Hasslinghausen, Germany.
*Corresponding Author : Univ.-Prof. Dr. Dr. Wolf-D. Grimm
Salzburg NAM Research Institute, Rochusgasse 13, 5020 Salzburg, Austria.
Tel: +43 662-822788, Fax: +43 662-822788;
Email: prof_wolf.grimm@yahoo.de
Received : May 12, 2023
Accepted : Jun 01, 2023
Published : Jun 08, 2023
Archived : www.jcimcr.org
Copyright : © Grimm WD (2023).
Abstract
Oral Neural Crest-Derived Stem Cells (oNCSCs) are a type of adult stem cell that can be isolated from the oral cavity. These stem cells have the ability to differentiate into various cell types, including neurons, glial cells, and adipocytes. oNCSCs have been shown to play a crucial role in the regeneration and repair of damaged tissues in the oral cavity, making them a promising candidate for use in regenerative medicine. This paper provides an overview of oNCSCs, including their origin, isolation methods, and potential applications in tissue engineering and regenerative medicine.
Citation: Fritsch T, Vukovic MA, Grimm WD, et al. Characterization of oral-derived neural crest-derived stem cell populations (oNCSCs) in the teeth: Therapeutic potential for bone tissue engineering. J Clin Images Med Case Rep. 2023; 4(6): 2447.
Introduction
Oral-Derived Neural Crest-Derived Stem Cell Populations (oNCSCs) are multipotent cells that have shown great promise in bone tissue engineering. oNCSCs can differentiate into osteoblasts, chondrocytes, and adipocytes, making them an ideal source for regenerative medicine. In this publication, we will explore the characterization of oNCSC populations in the teeth and their therapeutic potential for bone tissue engineering. Emerging evidence suggests that adult craniofacial tissues in vertebrates contain limited numbers of post-migratory NCSCs (reviewed in [1]. Adult multipotent NCSCs posses high levels of cellular plasticity which is only surpassed by pluripotent stem cells including embryonic stem cells and induced pluripotent stem cells. In particular, NCSCs have been shown to differentiate efficiently into ectodermal and mesodermal progeny including neuronal, glial, osteogenic, adipogenic, and chondrogenic cells, as well as melanocytes and Mesenchymal Stem Cells (MSCs). Previously, we have shown that multipotent Nestin-expressing NCSCs are present within the rat, mouse, and human palate [2,3]. Anatomically, within the subpalatal lamina propria, these cells are localized adjacent to specialized mechanoreceptors referred to as Meissner corpuscles [4]. Being a highly regenerative tissue [5-7], the mammalian palatal tissue contains several other cell types harboring progenitor cell and stem cell properties.
Characterization of oNCSC Populations: Palatal NCSCs can be accessed within minimally-invasive surgical procedures, expanded in vitro self-adherent neurospheres under serum-free conditions and are able to differentiate into major ectodermal and mesenchymal neural crest derivatives. Thus, NCSCs represent promising candidate cells for the use within modern regenerative medicine [8]. However, future use of human NCSCs in the clinical routine requires rigid testing in appropriate animal models to evaluate their safety and efficacy. Notably, according to the revised ISSCR guidelines for stem cell research and clinical translation, large animal models should be used since they better emulate the human anatomy and/or pathology [9]. In particular, the route of administration, the optimal cell numbers and/or dose of biologicals can be better extrapolated to the human system based on large animal studies (Figure 1). In this context, sheep models offer the advantage of a body weight similar to humans and a significantly longer lifespan than rodent models allowing long term studies. This is especially important in evaluating the safety and efficacy of autologous stem cell transplantation in long term preclinical studies.

Several adult stem cell populations have been identified in the sheep including amniotic fluid MSCs [10], derived from peripheral blood [11], MSCs from the olfactory epithelium [12] and the neural crest-derived periodontal ligament stem cells [13].
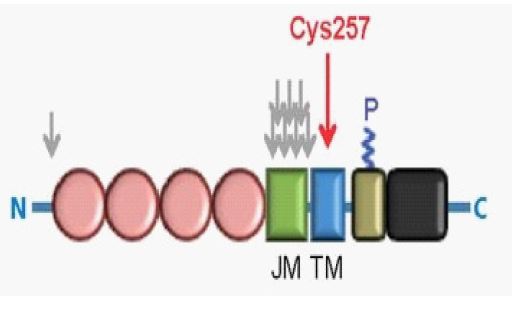
oNCSCs can be isolated from the periodontal tissue of extracted teeth (Figure 2). The cells can be cultured and expanded in vitro to generate a homogeneous population of stem cells. oNCSCs express surface markers such as CD29, CD44, CD73, CD90, and CD105, but do not express markers such as CD34 and CD45, which are associated with hematopoietic cells [14]. oNCSCs also express neural crest cell markers such as nestin, Sox10, and p75NTR [15]. oNCSCs can differentiate into osteoblasts, chondrocytes, and adipocytes under appropriate conditions [16]. The differentiation potential of oNCSCs is regulated by various signaling pathways, including the Wnt, BMP, and Notch pathways [17]. oNCSCs have also been shown to secrete various growth factors and cytokines, which can stimulate tissue regeneration [18].
In addition to this isolation and differentiation of oral NCSC, Molthera GmbH has another collection option from the subepithelial tissue of the palate. For this specific aim Standard Operational Procedures (SOP`s) have been developed by Molthera GmbH, PCT/EP2006/066221“A post-natal periodontal-derived neural stem cell”:

- Perform a new clinical technology to obtain uncultured NCSC isolates from a human tissue source (subepithelial connective tissue of the human palate) based on immuno-magnetic selection for CD271-positive stem cells. Based on our results obtained so far, we assume that uncultured CD45-/lowCD271+ NCSCs uniformly express CD73, CD90 and CD105. In addition, variable expression of MSCA-1 and SUSD2 is expected.
- There by enriching human NCSCs from subepithelial connective tissue of the palate from a native cell count of 105 to a cell count above 107. Enriched oral NCSC fractions express increased levels of BMP-2, COL1A2, VEGFC, SPARC, and CXCL12 transcripts. After culture expansion, CD271-selected NCSCs will be tri-potentially and phenotypically identical to NCSCs selected by plastid adherence (Figure 3).

Clinical-grade oNCSC selection with CD271 microbeads and the CliniMACS® system
We are using a cost-reducing clinical grade cultivation system for oNCSCs by using cGMP grade Afc-FEP bags. Afc-FEP bag-cultured oNCSCs will grow three-dimensionally in the human blood plasma-derived matrix, showing unchanged morphology, proliferative capacity, and the same expression profile compared to classically three-dimensionally cultured oNCSCs in standard adherent cell cultures. The genetic stability, of the oNCSCs cultured in the Afc-FEP bags is, moreover, accompanied by an unaltered telomerase activity. Importantly, the oNCSCs retain their potential to differentiate into mesodermal cell types of oral wound healing and regeneration into a variety of human tissues [19].
Briefly, prior to separation, oNCSCs are washed (400x g for 20 minutes) with GMP grade PBS/EDTA (Miltenyi Biotec) containing GMP grade 5% w/v human serum albumin. The supernatant is discarded. The volume in the transfer bag is then adjusted to 95 ml by adding PBS/EDTA/HSA buffer, to which the contents of a vial containing anti-CD271 microbeads for cell isolation are added. The cell/bead mixture is then incubated at Room Temperature (RT) for 30 minutes. The transfer bag is then transferred to the Clini MACS instrument and connected to a CliniMACS tubing set to achieve separation into a positive (post) and negative cell fraction. As background information, it should be added that the cell marker CD271, also known as LNGFR (low-affinity nerve growth factor receptor) or p75NTR, belongs to the “low-affinity neurotrophin receptor and tumor necrosis factor receptor” superfamily. CD271 is a well-known marker for ecto-mesenchymal stem cells, such as the oral NSCS we used.
Principle of MACS® separation
Briefly, first, the CD271+ cells are magnetically labeled with CD271 Micro Beads. Then, the cell suspension is loaded onto a MACS® column, which is placed in the magnetic field of a MACS separator. The magnetically labeled CD271+ cells are retained within the column. The unlabeled cells pass through, thus the magnetically labeled CD271+ cell fraction is enriched with CD271+ cells. After removing the column from the magnetic field, the magnetically labeled CD271+ cells can be eluted as a positively selected cell fraction. To increase purity, the positively selected cell fraction containing the CD271+ cells must be separated via a second column (Figure 4).
Ovine neural crest-derived stem cell (ovineNCSCs) isolation and culture
Briefly, palatal tissue was extracted from female sheep according to local guidelines and with approval from the Stavropol State Medical University Animal Ethics Committee (approval number 39, 16/04/2014). Prior to surgery, animals were starved overnight and had antibiotics administered (penicillin/streptomycin 3 ml/kg i.m) and general anesthesia was induced with thiopentone 20 mg/kg i.v. The sheep were intubated orally and anesthesia was maintained by halothane (1-2%) and nitrous oxide/oxygen in a ratio of 1:2. Extraction of the tissue was achieved using minimally-invasive access to the palate followed an atraumatic approach. For harvesting the stem cell-containing palatal tissue, a horizontal incision to the bone has been made 5 mm from the palatal gingival margin. Another horizontal incision has been made 2 mm coronal to the first incision and the periosteum has been dissected before removing the wedge of soft tissue. An approximately 10 × 6 mm subepithelial connective tissue graft was harvested from the palate and placed in 100 ml pre-cooled Chill Protec R plus solution. Incisions were closed with resorbable sutures. An antiseptic mouthwash was applied after surgery (chlorhexidine, 0.2%) for 3 days, and animals were returned to normal grazing. Additional control palatal tissue was extracted post-mortem at the Centre for Dairy Research (The University of Reading, Hall Farm) according to local guidelines. After mechanical dissection using a scalpel and surgical scissors, the palatal tissue was dissociated using 4 mg/ml Dispase at 4© for overnight followed by Collagenase I (0.3 units/ml, 90 min, 37©) treatment and mechanical trituration with a fire-polish glass Pasteur pipette. oNCSCs were cultured in serum-free media (Dulbeccos modified Eagles medium [DMEM]/F12) containing basic FGF-2, 20 ng/ml, EGF, 20 ng/ml, B27 supplement in low adhesion T25 cell culture flasks in a humidified incubator at 37© and 10% CO2. After 8–10 days, the cultures reached sub-confluency and primary neurospheres were dissociated using Trypsin/EDTA and a 100μm cell strainer resulting in an average of 2 × 106 single oNCSC per flask. The resulting oNCSC suspension was resuspended in DMEM/F12 containing basic FGF-2, 20 ng/ml, EGF, 20 ng/ml, B27 supplement and 10% newborn calf serum. The sub culturing protocol consisted of neurosphere passaging every 3–4 days with whole culture media change. For adherent culture, neurospheres were dissociated and cultivated in DMEM/F12 supplemented with 10% Fetal Calf Serum (FCS), FGF- 2 (20 ng/ml), and EGF (20 ng/ml). Medium was changed every 2–4 days. Adherent cells were passaged at 80–90% confluency using Trypsin/EDTA [20].

Therapeutic potential of oNCSCs for bone tissue engineering
Bone tissue engineering is an emerging field that aims to regenerate damaged or lost bone tissue using stem cells, scaffolds, and growth factors. oNCSCs have shown great promise in bone tissue engineering due to their ability to differentiate into osteoblasts and secrete various growth factors. oNCSCs have been used in various preclinical and clinical studies for bone tissue engineering. In a preclinical study, oNCSCs were seeded onto a collagen scaffold and implanted into a rat calvarial defect. The oNCSC-seeded scaffold resulted in a significant increase in new bone formation compared to the scaffold alone. In a clinical study, oNCSCs were isolated from the periodontal tissue of extracted teeth and implanted into a human alveolar cleft defect. The oNCSC implant resulted in significant bone formation and improved bone density.
Sources of oral tissues for stem cells
Discrete populations of stem cells (Figure 6) were extracted from a series of oral tissues. Dental Pulp, Both Adult Dental Pulp Stem Cells (DPSC) and Stem Cells from Human Exfoliated Deciduous Teeth (SHED), comprise the best-studied populations, complemented by studies of Periodontal Ligament Stem Cells (PDLSC), Alveolar Bone Stem Cells (ABSC), and Stem Cells from the Apical Papilla (SCAP). Tooth Germinal Progenitor Cells (TGPC) and Dental Follicle Stem Cells (DFSC) present in the tooth bud are stem cells directly involved in tooth development and therefore accessible for therapeutic use.
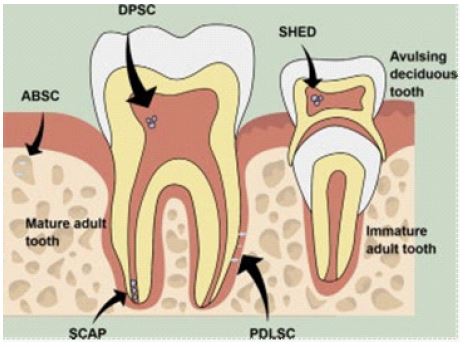
SHED, Stem Cells from HumanDeciduous Teeth; DPSC, Dental Pulp Stem Cells; SCAP, Stem Cells from the Apical Papilla Zellen aus der apikalen Papille; PDLSC, Parodontale Ligament Stammzellen; ABSC, Alveolarknochen-Stammzellen; TGPC, Tooth Germ Progenitor Cells; DFSC, Dental Follicle Stem Cells.
Associated oral tissues such as epithelium, gingiva (gums) and salivary gland also harbor unique populations of stem cells. Molthera GmbH, together with its international cooperation partners, has contributed significantly to the further development of this field of regenerative dentistry since 2005 [21-25], (Figure 6). Stem cells, also known as “progenitor cells”, are defined as clonogenic cells capable of both self-renewal and differentiation into multiple lineages. The term “stem cell” first appeared in the work of the German biologist Haeckel in 1868.” In 1908, the Russian histologist Alexander Maksimov postulated the existence of hematopoietic stem cells at the Congress of the Hematological Society in Berlin. There the term “stem cell” was proposed for scientific use.
Stem cells have contributed to the establishment of regenerative medicine. Regenerative medicine is the process of replacing or regenerating human cells, tissues, or organs for therapeutic purposes. Although the concept of regeneration in the medical field is not new, it has evolved significantly following the discovery of stem cells and, more recently, has found its application in dentistry following the identification of dental stem cells. Nevertheless, subsequent researchers have further improved this work. The major breakthrough in the history of regenerative dentistry was achieved in 2000, when [27] identified and isolated an odontogenic progenitor population in adult dental pulp. These cells were termed Dental Pulp Stem Cells (DPSCs). Since this discovery, several investigators have reported different types of dental stem cells, which are briefly described below.
Dental pulp stem cells
DPSCs are mesenchymal stem cells in the dental pulp. DPSCs have osteogenic and chondrogenic potential in vitro and can differentiate into dentin in vivo and also differentiate into a dentin-pulp-like complex. Recently, immature dental pulp stem cells were identified to be a pluripotent subpopulation of DPSCs generated by dental pulp organ culture. DPSCs have since been putative candidates for dental tissue engineering due to:
- Easy surgical access to the harvest site and very low morbidity after dental pulp extraction.
- DPSCs can generate much more typical dentin tissue within a short period of time than non-dental stem cells.
- Can be safely cryopreserved and recombined with many biological carrier materials.
- Possess immunoprivileging and anti-inflammatory capabilities that show advantages for allografts.
Stem cells from human exfoliated deciduous teeth (SHED).
Dr. Songtao Shi discovered SHED in 2003, and [28] confirmed that SHED were capable of differentiating into a variety of cell types, to a greater extent than DPSCs, including osteoblast-like, odontoblast-like cells, adipocytes, and neural cells. [29] investigated the possible neural crest origin of SHED. The main function of these cells appears to be the formation of mineralized tissue that can be used to enhance orofacial bone regeneration. Stem cells present in human exfoliated deciduous teeth are:
- Adipocytes: Can be used to treat various spinal and orthopedic conditions, Crohn’s disease, cardiovascular disease, and may also be useful in plastic surgery.
- Chondrocytes and osteoblasts: Have been used to grow intact teeth in animals.
- Mesenchymal stem cells (MSCs): Have been successfully used to repair spinal cord injuries and restore feeling and movement in paralyzed human patients. They can also be used to treat neuronal degenerative diseases such as Parkinson’s, cerebral palsy, Alzheimer’s and other such diseases. MSCs have better healing potential than other types of adult stem cells.
Stem cells from the apical papilla (SCAP)
Mesenchymal Stem Cells (MSCs) located in the apical papilla of permanent teeth with incompletely formed roots are referred to as SCAP. These were discovered by Sonoyama et al. SCAP are capable of forming odontoblast-like cells, producing dentin in vivo, and are likely the cell source of primary odontoblasts for root dentin formation. SCAP supports apexogenesis, which may occur in infected non-fully formed permanent teeth with periradicular periodontitis or abscess. SCAP located in the apical papilla survive such pulp necrosis due to their proximity to the periapical tissue vasculature. Therefore, even after endodontic therapy, SCAP can generate primary odontoblasts that complete root formation under the influence of the vital epithelial Hertwig root sheath.
Periodontal ligament stem cells (PDLSCs).
[30] described the presence of multipotent Postnatal Stem Cells In the Human Periodontal Ligament (PDLSCs). When transplanted into rodents, PDLSCs had the ability to generate a cementum/periodontal ligament-like structure and contributed to periodontal tissue repair. These cells can also be isolated from cryopreserved periodontal ligaments, retaining their stem cell characteristics, including formation of single colonies, regeneration of cementum/periodontal ligament-like tissue, expression of MSC surface markers. Thus, based on multipotent differentiation, they represent a source of MSC-assisted regeneration.
In a mini-pig model, autologous SCAP and PDLSCs were loaded onto hydroxyapatite/tricalcium phosphate and gelfoam scaffolds and implanted into mandibular alveoli, where they formed a bio-root surrounded by periodontal ligament tissue and in a direct relationship with the surrounding bone. [31] recognized that PDLSCs have regenerative potential when seeded onto a three-dimensional biocompatible scaffold, enabling their use as graft biomaterials for bone tissue engineering in regenerative dentistry, while other authors [32] reported the formation of cementum and periodontal ligament-like tissue when PDLSCs were seeded onto bioengineered dentin.
Conclusion
oNCSCs are a promising source of stem cells for bone tissue engineering. oNCSCs can be isolated from the periodontal tissue of extracted teeth and expanded in vitro to generate a homogeneous population of stem cells. oNCSCs express various surface markers and can differentiate into osteoblasts, chondrocytes, and adipocytes under appropriate conditions. oNCSCs also secrete various growth factors and cytokines, which can stimulate tissue regeneration. oNCSCs have shown great promise in preclinical and clinical studies for bone tissue engineering, making them a promising source of stem cells for regenerative medicine.
References
- Hauser S, Widera D, Qunneis F, Müller J, Zander C, et al. Isolation of Novel Multipotent Neural Crest-Derived Stem Cells from Adult Human Inferior Turbinate. Stem Cells and Development 2012; 21: 742–756. https://doi.org/10.1089/scd.2011.0419
- Widera DC, Zander M, Heidbreder, Kasperek Y, Noll T, O Seitz, et al. Adult palatum as a novel source of neural crest- related stem cells, Stem Cells. 2009; 27: 1899–1910.
- Martin et al. Multiple versus single virus respiratory infections: Viral load and clinical disease severity in hospitalized children. Influenza and Other Respiratory Viruses. 2012; 6: 71–77.
- Kaltschmidt B, Kaltschmidt C, Widera D. Adult craniofacial stem cells: Sources and relation to the neural crest. Stem Cell Rev Rep. 2012; 8: 658-671.
- Kahnberg KE, Thilander H. Healing of experimental excisional wounds in the rat palate. (I) Histological study of the interphase in wound healing after sharp dissection. Int J Oral Surg. 1982; 11: 44-51.
- Kahnberg KE, Thilander H. Healing of experimental excisional wounds in the rat palate. II. Histological study of electrosurgical wounds. Swed Dent J. 1984; 8: 49-56.
- Kahnberg KE, Thilander H. Healing of experimental excisional wounds in the rat palate. III. Effects of radiation on wound healing. Swed Dent J. 1987; 11: 61-70.
- Grimm WD, M Plöger, I Schau, MAA Vukovic, EVV Shchetinin, et al. Prefabricated 3D allogenic bone block in conjunction with stem cell-containing subepithelial connective tissue graft for horizontal alveolar bone augmentation: A case report as proof of clinical study principles, Med. News North Caucasus. 2014; 9: 175–178.
- Daley GQ, et al. Setting Global Standards for Stem Cell Research and Clinical Translation: The 2016 ISSCR Guidelines. Stem cell reports. 2016; 6: 787–797.
- Tian M, Wang H, Chen Y, Yang F, Zhang X, et al. Characteristics of aerosol pollution during heavy haze events in Suzhou, China. Atmospheric Chemistry and Physics. 2016; 16: 7357–7371. https://doi.org/10.5194/acp-16-7357-2016.
- Jaber Lyahyai, Aziza Sbiti, Amina Barkat, Ilham Ratbi, Abdelaziz Sefiani. Spinal Muscular Atrophy Carrier Frequency and Estimated Prevalence of the Disease in Moroccan Newborns. Genetic Testing and Molecular Biomarkers. 2012.215-218. http://doi.org/10.1089/gtmb.2011.0149
- Veron AD, Bienboire-Frosini C, Feron F, et al. Isolation and characterization of olfactory ecto-mesenchymal stem cells from eight mammalian genera. BMC Vet Res. 2018; 14: 17. https://doi.org/10.1186/s12917-018-1342-2
- Gronthos S, K Mrozik, S Shi, PM Bartold, et al. Ovine periodontal ligament stem cells: Isolation, characterization, and differentiation potential. Calcif. Tissue Int. 2006; 310-317.
- Grimm WD, A Dannan, S Becher, G Gassmann, W Arnold, G Varga, T Dittmar, et al. The ability of human periodontium-derived stem cells to regenerate periodontal tissues: A preliminary in vivo investigation. Int. J. Periodontics Restorative Dent. 2011; 31: e94–e101.
- Achilleos A, PA Trainor. Neural crest stem cells: Discovery, properties and potential for therapy. Cell Res. 2012; 22: 288–304.
- Dupin E. L. Sommer. Neural crest progenitors and stem cells: from early development to adulthoodDev. Biol. 2012; 366: 83-95.
- Weber M, G Apostolova, D Widera, M Mittelbronn, G Dechant, et al. Alternative generation of CNS neural stem cells and PNS derivatives from neural crest-derived peripheral stem cells, Stem Cells. 2015; 33: 574–588.
- Zeuner MT, K Patel, B Denecke, B Giebel, D Widera, et al. Paracrine effects of TLR4- polarised mesenchymal stromal cells are mediated by extracellular vesicles. J. Transl. Med. 2016; 14: 34.
- Widera D, Zander C, Heidbreder M, et al. Adult palatum as a novel source of neural crest related stem cells. Stem Cells. 2009; 27:1899-1910
- Grimm WD, N Didenko, A Dolgalev, D Bobryshev, et al. Isolation and characterisation of adult ovine Neural Crest Derived Stem Cells (ovine NCSCS) from Palatal tissue for comparative implant research and alveolar regeneration, J Clin Periodontol. 2018; 45: 328–329
- Grimm WDWD, T Fritsch, B Giesenhagen, SSV Sirak, AAA Sletov, MMM Aybazov,
- G Petrosyan, AA Adamchik, A Vukovic, IIV Koshel, et al. Neural crest-related stem cells of oral origins in vitro and used in osteoporotic sheep model - investigated due to therapeutic effects in alveolar bone regeneration. Med. News North Caucasus. 2016; 11: 192–196.
- Grimm WN Didenko, T Fritsch, B Giesenhagen, M Vukovic, et al. Effect of Human Neural Crest-Related Stem Cell Homing (hNCSCs homing) on the Mineralization of Newly Formed Alveolar Bone using an Allogen Bone Substitute. Biomed. J. Sci. Tech. Res. 2019; 17: 1-12.
- Grimm W, W Arnold, S Becher, A Dannan, G Gassmann, S Philippou, et al. Does the chronically inflamed periodontium harbour cancer stem cells? Stem Cell Biol. Heal. 2009; 251–279.
- Arnold WH, S Becher, A Dannan, D Widera, T Dittmar, M Jacob, et al. Morphological characterization of periodontium-derived human stem cells. Ann. Anat. 2010; 192: 215–219.
- Grimm W. 3-D-Augmentation mit simultaner Implantation unter Einsatz einer natürlichen Stammzellresource. Implantol. J. 2016; 11: 2-11.
- Gronthos S, Brahim J, Li W, Fisher LW, Cherman N, et al. Stem cell properties of human dental pulp stem cells. J Dent Res. 2002; 81: 531-535.
- Miura M, Gronthos, S, et al. SHED: Stem cells from human exfoliated deciduous teeth. Proceedings of the National Academy of Sciences of the United States of America www.pnas.orgcgidoi10.1073pnas.0937635100.
- Sonoyama W, Liu Y, Fang D, Yamaza T, Seo BM, et al. Mesenchymal Stem Cell- Mediated Functional Tooth Regeneration in Swine. PLoS ONE. 2006; 1: e79.
- Seo BM, Miura M, Sonoyama W, Coppe C, Stanyon R, Shi S, et al. Recovery of Stem Cells from Cryopreserved Periodontal Ligament. Journal of Dental Research. 2005; 84: 907-912.
- Trubiani, et al. Stem Cell Research & Therapy. 2016; 7: 1.
- Kabir MA, M Murata, T Akazawa, K Kusano, K Yamada, M Ito, et al. Evaluation of perforated demineralized dentin scaffold on bone regeneration in critical-size sheep iliac defects. Clin. Oral Implants Res. 2017.