
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A rare case of an inclusion cyst mimicking carcinoma
unknown primary with secondary in the neck
Mayank Rampal; Jaimanti Bakshi*; Aakriti Basandrai
Department of Otorhinolaryngology, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
*Corresponding Author : Jaimanti Bakshi
Department of Otorhinolaryngology, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
Email: bakshi.jaimanti@pgimer.edu.in
Received : May 09, 2023
Accepted : Jun 01, 2023
Published : Jun 08, 2023
Archived : www.jcimcr.org
Copyright : © Bakshi J (2023).
Keywords: Squamous cell carcinoma; Carcinoma of unknown primary; Epithelial inclusion cyst.
Citation: Rampal M, Bakshi J, Basandrai A. A rare case of an inclusion cyst mimicking carcinoma unknown primary with secondary in the neck. J Clin Images Med Case Rep. 2023; 4(6): 2448.
Introduction
Squamous cell carcinomas of Head and Neck are at a rising trend since recent years. Southeast Asia (especially the Indian subcontinent) is a high-risk region for these cancers. More than 200,000 new such cases are reported each year in India [1].
Patients usually present with a neck mass without any other known primary tumour. The differential diagnosis includes both benign and malignant growth, of which malignant can be either primary tumours or metastases. Also they can present with metastatic carcinoma to a neck lymph node without any known primary lesion known as Carcinoma Unknown Primary (CUP) with secondary in neck.
Carcinoma unknown primary with secondaries in neck refers to cases in which even after thorough clinical, radiographic and surgical evaluation (which includes biopsies and/or resection of the suspected primary site), the primary remains unidentified and these includes lesions in oral cavity, oropharynx and upper aerodigestive tract. CUP cases account for 5-10% of head and neck cancers and almost 75% or more of these are squamous cell carcinomas (SCCs) [2,3]. “True” CUP accounts for 1-2% of head and neck cancers and are in a decreasing trend because of improvement in detection methods [3].
In CUP, the lymph nodes involved can help to determine the likely site of tumour origin.
The most common site of head and neck SCCs with an unknown primary is the oropharynx (90%) (specifically the crypt epithelium of the palatine tonsils and base of the tongue or lingual tonsil) [4]. Oropharyngeal SCCs, including HPV-related, metastasize to levels II and III, and occasionally to level IV. 18F-fluorodeoxyglucose positron emission tomography combined with CT (18F-FDG-PET/CT) is very helpful in localizing the primary tumours. The detection rate of primary in patients with tumour metastasis in the head and neck region and other body regions is from 24% to 53% [5]. Generally, a node with a SUV max value of 4.5 and above is counted as metastatic, while the nodes with SUV value below this value remains uncertain [6].
Table 1: Common patterns of lymph node metastasis in the head and neck.
| Nodal group | Primary tumour sites |
|---|---|
| Level IA (submental) | Anterior oral cavity, lower lip |
| Level IB (submandibular) | Oral cavity, anterior nasal cavity, submandibular gland, midfacial face skin |
| Level II (upper jugular) | Oropharynx, oral cavity, nasopharynx, nasal cavity, larynx, hypopharynx |
| Level III (mid jugular) | Oropharynx, oral cavity, nasopharynx, larynx, hypopharynx |
| Level IV (lower jugular) | Oropharynx, larynx, hypopharynx, upper oesophagus, thyroid |
| Level V (posterior triangle) | Nasopharynx, posterior scalp skin, thyroid |
| Level VI (anterior compartment) | Thyroid, larynx, hypopharynx, upper oesophagus |
| Supraclavicular | Non-head and neck, thyroid |
| Retropharyngeal | Nasopharynx, posterior pharynx |
| Parotid | Lateral/upper facial and scalp skin, parotid gland |
Epidermoid cysts are slow-growing benign cysts which are rare and is derived from abnormally situated ectodermal tissue. It is defined as “A simple cyst lined with stratified squamous epithelium with lumen filled with cystic fluid or keratin and no other specialized structure” [7]. During the development period, these are derived from abnormal squamous epithelial components of ectodermal tissue. These can also be developed as acquired cyst from trauma or surgery-related implanted epithelium.
Epidermoid cysts are benign pathologies which can occur anywhere in the body, predominantly in areas of fusion of embryonic elements. Most common sites are the ovaries and the testicles (80%) and the cysts have an incidence of 1.6-7% in the head and neck region [8].
This article aims to discuss a case of epithelial inclusion cyst on the left side of the neck region (level II) of a 69 years old male patient mimicking carcinoma unknown primary with secondary in the neck.
Case presentation
Our patient, a 69 years old gentleman sought ENT consultation for swelling in the left side of the neck for around 3-4 months duration. The swelling had an indolent course and was gradually progressive. Our patient denied any history of pain, dysphagia, odynophagia, dyspnea, weight fluctuations and trauma. The patient was a chronic smoker (biddi) with an approximately 60 pack years smoking history. Local examination of the neck revealed nodular swelling of size 2 x 2 cm which was firm, mobile in all directions, and non-tender in left level II of the neck. The overlying skin was free from underlying mass and mobile. The patient had good oral hygiene and the oral cavity was grossly normal. On 70-degree endoscopy bilateral vocal cords were within normal limits and nasal endoscopy showed no growth or mass in the nasopharynx and nasal cavity.
FNAC from the lesion yielded necrotic material, smears from which show scattered as well as few clusters of mature-looking squamous cells. The cells show mild atypia. The background shows many degenerated polymorphs (Figure 1). The possibility of well-differentiated squamous cell carcinoma cannot be ruled out.

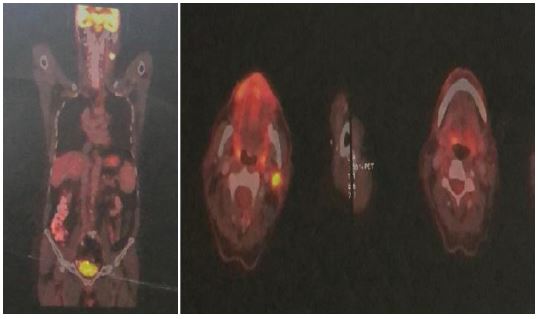
A positron emission tomography-computed tomography of whole body(base of skull to mid-thigh) was done in which intense focal FDG uptke SUV max 6 was seen in an enhancing soft tissue lesion of size approx 18 x 19 mm in level II left cervical lymph node? lymph node. (Figure 2) Non-FDG avid bilateral IIA & left level III cervical lymph nodes were also noted.
Under general anaesthesia, biopsy was taken from the left base of the tongue and left fossa of Rossenmuller which showed no evidence of malignancy and the neck lesion was excised with left selective neck dissection. The left level II lymph node was removed along with the left level III and IV lymph node. The left internal jugular vein, left spinal accessory nerve and left sternocleidomastoid muscle were identified and preserved. The left submandibular gland was preserved. A negative suction drain was placed and the wound was closed in two layers. The drain was removed on post-op day 5. His follow-up at 4 weeks revealed a well-healed wound over the neck.
Histopathology of one of the larger level II lymph nodes showed few cysts lined by bilateral epithelium, with the discontinuous basal cells and tall oncocytic epithelium. The surrounding lymphoid stroma showed many follicles. In addition, foci of collection of foamy histiocytes, and neutrophils with fibrosis were noted. Overall features were epithelial inclusions (rests) with acute lymphadenitis. The rest of the lymph nodes i. e. level II (0/9), level II (0/2), and level IV (0/16) showed follicular hyperplasia. All of these findings pointed towards left level II epithelial inclusion cyst.
There was no evidence of any local recurrence of the lesion at his 6 monthly follow up visits. Our patient was, to a great degree satisfied with the surgical outcome and was symptom-free with no recurrences.
Discussion
The definition of an occult or unknown primary carcinoma is the presentation of metastatic neck lymph nodes without the development of a primary lesion within a period of subsequent five-year. Carcinoma unknown primary with secondaries in neck are the cases in which even after a thorough clinical, radiological and surgical evaluation (which can include biopsies or resection of the suspected primary site), primary remains unidentified which could be in the oral cavity, oropharynx and upper aerodigestive tract. “True” CUP accounts for 1-2% of head and neck cancers and are now further in decreasing trend due to improvement in detection methods [3]. In CUP, the likely site of tumour origin can be determined by the lymph nodes involved. The most common site of head and neck SCCs that present as an unknown primary includes the oropharynx (specifically the crypt epithelium of the palatine tonsils and base of the tongue or lingual tonsil), where almost 90% of detectable primary tumours are present [4]. Oropharyngeal SCCs, including HPV-related, metastasize to levels II and III, and often to level IV.
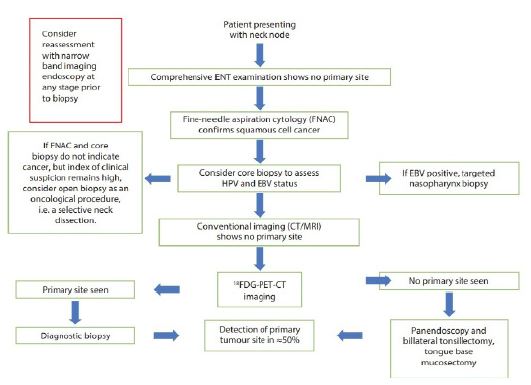
National Institute for Health and Care Excellence (NICE) made the following recommendations for people with a neck lump that is thought to arise from head and neck cancer [9]:
1. Consider adding ultrasound guidance to fine-needle aspiration cytology or core biopsy.
2. Consider having a cytopathologist or a biomedical scientist to assess the adequacy of the cytology sample.
3. Consider an FDG PET-CT scan as the first investigation to detect the primary site.
4. Consider using NBI (in the clinic or during general anaesthetic assessment) in cases where PET-CT has led to identifying a primary site.
5. Offer surgical diagnostic assessment if the FDG PET-CT does not identify a primary site, including guided biopsies, tonsillectomy and TBM.
F-fluorodeoxyglucose positron emission tomography along with CT (F-FDG-PET/CT) helps in localizing the primary tumours. A node with SUV max value more than 4.5 is considered as metastatic and the nodes with SUV value less than this value remains uncertain [6]. The conditions like infection, inflammation and granulomatous diseases can also show increased FDG uptake in head and neck cancer patients, which mimics malignancy. The increased uptake in such cases is due to increased glycolysis in activated inflammatory cells (the macrophages). The clinical history points to the cause of FDG uptake; however, various inflammatory conditions and neoplastic diseases can coexist. The value of SUVs helps to differentiate between benign and malignant diseases and SUVs more than 3 is considered as a guide to indicate towards neoplasm. But SUVs more than 3 can also occur in acute infections, suppurative lymphadenopathy and abscess [10]. In our case, the swelling had an indolent course and was gradually progressive. Also, the patient was a chronic smoker (biddi) with an approximately 60 pack years smoking history and a local examination of the neck revealed nodular swelling of size 2 x 2 cm which was firm, mobile in all directions, and non-tender in the left level II of the neck, features were not suggestive of suppurative lymphadenopathy and abscess.
Conclusion
True Carcinoma of unknown primary is a rare entity and a surgeon faced with such a tumour is at a challenge with the clinical diagnosis. Presentation of a chronic slow-growing nodular swelling in the head and neck region of an old patient with chronic tobacco consumption without detection of the primary tumour after a thorough clinical, radiographic and surgical evaluation should alert the surgeon to the possibility of a Carcinoma unknown primary with secondaries in the neck. 18F-fluorodeoxyglucose positron emission tomography combined with CT (18F-FDG-PET/CT) is very helpful in the localization of primary tumours but has its own demerits of false positivity. This, to the best of our knowledge, is the first-ever reported case of an inclusion cyst mimicking carcinoma unknown primary with secondary in the neck.
Patient consent: Informed consent has been obtained from the patient and patient attendants as a standard departmental protocol for all publications.
References
- Kulkarni MR. Head and neck cancer burden in India. Int J Head Neck Surg. 2013; 4: 29-35.
- Pavlidis N, Briasoulis E, Hainsworth J, Greco FA. Diagnostic and therapeutic management of cancer of an unknown primary. European journal of cancer. 2003; 39: 1990-2005.
- Guntinas-Lichius O, Peter Klussmann J, Dinh S, Dinh M, Schmidt M, et al. Diagnostic work-up and outcome of cervical metastases from an unknown primary. Acta oto-laryngologica. 2006; 126: 536-544.
- Cianchetti M, Mancuso AA, Amdur RJ, Werning JW, Kirwan J, et al. Diagnostic evaluation of squamous cell carcinoma metastatic to cervical lymph nodes from an unknown head and neck primary site. The Laryngoscope. 2009; 119: 2348-2354.
- Delgado-Bolton RC, Fernández-Pérez C, González-Maté A, Carreras JL. Meta-analysis of the performance of 18F-FDG PET in primary tumor detection in unknown primary tumors. J Nucl Med. 2003; 44:1301-1314.
- Lim RSM, Ramdave S, Beech P, Billah B, Karim MN, et al. Utility of SUVmax on 18 F-FDG PET in detecting cervical nodal metastases. Cancer Imaging. 2016; 16: 1-8.
- Janarthanam J, Mahadevan S. Epidermoid cyst of submandibular region. Journal of oral and maxillofacial pathology: JOMFP. 2012; 16: 435.
- Gulia SP, Lavanya M, Kamidi V, Arun Kumar SP. Epidermoid cyst of the tonsil: An incidental finding. Case Reports. 2015; 2: 777-779.
- Nice Guideline [NG36]. Cancer of the upper aerodigestive tract: assessment and management in people aged 16 and over. 2016; 2016.
- Purohit BS, Ailianou A, Dulguerov N, Becker CD, Ratib O, et al. FDG-PET/CT pitfalls in oncological head and neck imaging. Insights Imaging. 2014; 5: 585-602.