
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Tropical paradise turns into a nightmare. A rare case of
evisceration caused by the misuse of over-the-counter
proparacaine and dexamethasone eye drops
Chee Shew Fei1,2; Chong Xin Yee1; Ishaq Hakim1; Zunaina Embong2*
1Department of Ophthalmology, Hospital Selayang, Selayang, Selangor, Malaysia.
2Department of Ophthalmology and Visual Science, Universiti Sains Malaysia, Kubang Kerian, Kelantan, Malaysia.
*Corresponding Author : Zunaina Embong
Department of Ophthalmology and Visual Science, Universiti Sains Malaysia, Kubang Kerian, Kelantan, Malaysia.
Tel: +60199396868;
Email: zunaina@usm.my
Received : May 08, 2023
Accepted : Jun 05, 2023
Published : Jun 12, 2023
Archived : www.jcimcr.org
Copyright : © Embong Z (2023).
Abstract
The abuse of topical anesthetics and steroids is not uncommon. However, having an eye eviscerated is rare due to complications from abusing both topical eyedrops. We report a case of Left Eye (LE) severe corneal ulcer with panophthalmitis secondary to over-the-counter topical proparacaine and topical dexamethasone abuse. His vision was No Perception of Light (NPL). His eye was not salvageable and evisceration was performed due to a painful blind eye. Topical anesthetics and steroids abuse can lead to serious complications such as chronic keratitis and endophthalmitis. The availability of topical anesthetics and steroids over-the-counter must be re-evaluated to prevent such complications.
Keywords: Topical anesthetics; Topical steroids; Proparacaine eye drop; Dexamethasone eyedrop, Evisceration; Corneal ulcer.
Citation: Fei CS, Yee CX, Hakim I, Embong Z. Tropical paradise turns into a nightmare. A rare case of evisceration caused by the misuse of over-the-counter proparacaine and dexamethasone eyedrops. J Clin Images Med Case Rep. 2023; 4(6): 2451.
Introduction
Abuse or misuse of topical anesthetics and steroids is not uncommon, especially when the eyedrops are easily accessible in pharmacies without a medical prescription. To save money and time, some patients prefer to purchase eye drops and self-medicate to treat minor ailments and dry eyes, some continue previous prescriptions by the doctor without continuing to follow up. A prospective cross-sectional observational study conducted for 3 months between November 2016 and January 2017 across 16 pharmacies in Amman, Jordan reported about 84.2% of topical eyedrops were requested by the patients without medical prescription [1]. According to the News Straits Times dated 17 Aug 2005 in Malaysia, topical steroid eyedrops were easily obtained from pharmacies in Malaysia without proper prescription by the doctor [2]. This issue was also evident in a cross-sectional study done among welders in Iran, out of 314 welders who have admitted the use of anesthetic eye drops, 97.4% claimed that they have obtained the medication without medical prescriptions [3].
Corticosteroid eyedrops are well known as a “wonder drug” to treat allergic reactions or inflammatory conditions, especially anterior segment inflammation as it alleviates symptoms effectively and rapidly. It is vital to prevent temporary or permanent visual loss which could happen if ocular inflammation is left untreated. However, it could cause a weakening of the immune system and thus increase the susceptibility to infection. It is also known to inhibit the growth factors which are important for wound healing, thus exacerbating the signs and symptoms of infective keratitis or fungal infection. Uncontrolled use of corticosteroid eyedrops could also lead to steroid-induced glaucoma and cataract.
Ayse Yagci et al. reported 100% of oval corneal epithelial defect, 57.7% of ring-shaped keratitis, 46.2% of stromal infiltrate, and 42.3% of hypopyon in 26 eyes of 19 men included in the study who had a history of abusing topical anesthetics [4]. Treatments include topical antibiotics, artificial tears with preservative-free, autologous serum, and bandage contact lenses. However, it’s rare to have an eye eviscerated due to complications from abusing topical anesthetics and steroids. We report a case of Left Eye (LE) severe corneal ulcer with panophthalmitis secondary to abuse of Over-The-Counter (OTC) topical proparacaine and topical dexamethasone that eventually leads to evisceration.
Case presentation
A 70-year-old man with underlying diabetes mellitus and hypertension was first seen at our ophthalmology clinic two years ago. At the initial presentation, he complained of LE blurring of vision associated with LE redness, pain, and double vision for 1 month. His LE vision was Counting Fingers (CF). A diagnosis of LE carotid-cavernous fistula was made after Computed Tomography Angiography (CTA) was done. His condition was successfully treated with embolization although his LE vision remained poor at CF post-operation. He was under the multi-disciplinary care of ophthalmologists and neurosurgeons. However, he failed to attend his follow-ups subsequently.
Despite discontinuing his appointments, the patient used OTC topical proparacaine 0.5% and dexamethasone 0.1% from time to time in both eyes. He used OTC topical proparacaine and dexamethasone whenever he had eye discomfort, eye pain, foreign body sensation, or eye redness in either eye. After using proparacaine and dexamethasone eye drops intermittently for one year, he started to notice a small central whitish spot over his LE. He denied any eye redness, eye discharge, or eye pain. The patient increased the frequency of both OTC eyedrops instillation to three times daily in the LE to treat his eye condition and thought that it would resolve. However, the whitish spot did not disappear but was growing bigger progressively. There was no history of injury or trauma to the eye.
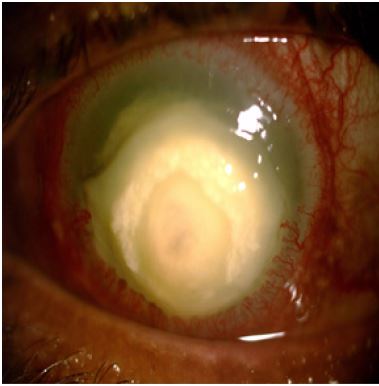
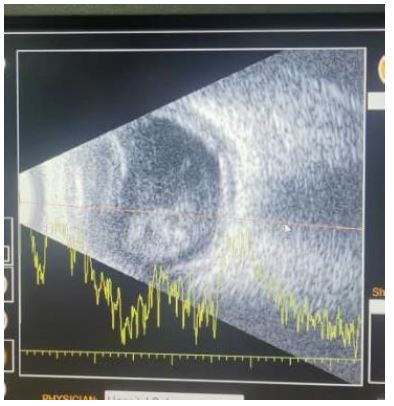
After self-medicating for four months, he finally decided to seek treatment. He came to our clinic, complaining of LE severe pain with eye redness and total loss of vision for 2 weeks. LE examination revealed his vision was No-Perception-Of-Light (NPL) with positive reverse Relative Afferent Pupillary Defect (RAPD) and total ophthalmoplegia. His conjunctiva over LE was markedly injected with huge opacity almost covering the whole of the cornea, obscuring the visual axis. Anterior segment examination showed a severe cornea ulcer with an endothelial plaque (Figure 1). We were unable to view his fundus due to obscuration by the cornea ulcer. The LE Intraocular Pressure (IOP) was 6 mmHg. An ultrasound scan of the LE showed dense vitritis with loculation and posterior scleral thickening (Figure 2). Right Eye (RE) examination revealed 6/12 visual acuity with a normal anterior segment. On fundus examination, the RE optic disc was pink, the cup-disc ratio was 0.4 and there were no diabetic retinopathy changes. The RE IOP was high at 30 mmHg. Gonioscopy done over RE revealed an open angle in all quadrants. The diagnosis of his condition was LE severe corneal ulcer with panophthalmitis and RE high IOP secondary to steroid responder. He was admitted to the ward. Corneal scraping was performed and sent for culture. His LE was started on hourly Gutt ceftazidime at 5% and hourly Gutt gentamicin at 0.9%. Intravenous ceftriaxone 1 g OD was administered too. His RE was treated with Gutt Timolast OM and Gutt Xalatan ON.
Corneal scraping successfully isolated Staphylococcus epidermis and Staphylococcus lugdunensis. Both organisms were sensitive to his antibiotic regimen. However, in view of persistent eye pain and no improvement of his LE condition after 5 days of treatment, an evisceration was performed. Intraoperatively, the vitreous was noted to be straw-colored and foul-smelling with macerated retinal tissue. The corneal button was sent for culture and sensitivity. The result came back as occasional pus cells with few gram-positive cocci; however, no growth was obtained.
Discussion
To the best of our knowledge, a case of abuse of both proparacaine and dexamethasone eye drops so severe that the patient ended up with evisceration has never been reported. Topical anesthetics such as proparacaine is commonly used by ophthalmologists in daily settings for an eye examination. It is also used in the emergency department or general practice to reduce discomfort before procedures such as eye irrigation. Topical anesthetics generally do not cause any harm when used correctly. Topical dexamethasone is also a common ocular drug prescribed by ophthalmologists for conditions such as allergic conjunctivitis, herpetic keratitis, uveitis, post-ocular surgery such as cataract surgery, and trabeculectomy. Topical anesthetics and dexamethasone eye drops are usually not available as OTC unless prescribed. However, the increasing ease to purchase these eyedrops OTC had posed some serious problems that lead to misuse, abuse, and addiction. There are grave complications from the abuse of both eye drops.
The side effects of topical anesthetics are well-documented. Long-term usage of topical anesthetics can cause mild to severe cornea conditions such as punctate epithelial keratopathy, loss of corneal epithelial cells, delay of epithelial wound healing, ring-shaped stromal keratitis, corneal edema, pain disproportionate to endothelial cell loss and decreased visual acuity. More serious sequelae from abuse of topical anesthetics are infectious keratitis, neurotrophic ulcer, stromal melting, corneal perforation, and permanent visual loss [5,6]. Evidence showed that topical anesthetics cause cornea toxicity by preventing corneal epithelial cell proliferation and migration [7]. In the presence of an epithelial defect, the topical anesthetics can penetrate deeper into the stromal layer and cause further damage. This eventually led to delayed epithelial wound healing and persistent epithelial defect. Besides the direct toxic effect on the cornea, topical anesthetics can also disrupt the tear film stability [8]. Topical anesthetics induce corneal sensory loss and as a result, this causes diminished reflex tear secretion and decreased eye blinking. Reduced tear secretion indirectly allows topical anesthetics to cause more direct toxicity to the ocular surface. Lastly, it is believed that preservatives in topical anesthetics were toxic to the cornea and can cause damage to the ocular surface.
Corticosteroids are one of the commonest medications prescribed by ophthalmologists. Corticosteroids such as dexamethasone eye drops and prednisolone eye drops are very potent and effective in the treatment of pseudomembrane conjunctivitis, vernal keratoconjunctivitis, uveitis, post-operative ocular inflammation, etc. However, they can produce a plethora of adverse ocular and systemic events. Systemic side effects are hypothalamic-pituitary-adrenal axis suppression, hyperglycemia, delayed wound healing, susceptibility to infection, osteoporosis, gastritis, anxiety, insomnia, depression, skin thinning, bruising, and proximal muscle atrophy [9]. The ocular side effects of topical corticosteroids are well-reported. These include lid ptosis, orbital fat atrophy, delayed epithelial healing, exacerbation of infection, reactivation of herpes simplex keratitis, crystalline keratopathy, corneal deposits, corticosteroid-induced glaucoma, and corticosteroid-induced cataract [10].
Certain risk factors for patients to develop topical eyedrop abuse include addictive behavior, psychiatric illness, etc. These should also be taken into consideration by ophthalmologists and primary care practitioners when prescribing topical anesthetics and steroids to prevent permanent damage to the cornea.
This patient had previous experience using both types of eyedrops. He felt he had benefited from the medications. However, he did not know about the solemn side effects of long-term usage of both eye drops. The fact that his LE vision was poor after embolization of the carotid-cavernous fistula had hindered him from seeking early treatment from an ophthalmologist and instead patient chose to self-medicate. The patient did not realize the severity of his eye condition as his vision was poor, to begin with. He was able to purchase both eyedrops easily from the pharmacy, sometimes with his general practitioner’s prescription and sometimes without a doctor’s prescription. The patient used topical dexamethasone 0.1% which is one of the most potent corticosteroid eye drops. We believed both eyedrops had caused him to develop LE epithelial thinning with a persistent epithelial defect which subsequently led to a corneal ulcer. Topical dexamethasone predisposed him to be sussusceptible to infection and thus worsen his LE corneal ulcer and became panophthalmitis. He also used both eyedrops for his RE and fortunately, on examination, his RE had raised IOP, with no other ocular abnormalities detected. Corticosteroid-induced ocular hypertension generally happens within a few weeks of treatment with potent corticosteroids, or within months with less potent corticosteroids [11]. Corticosteroid-induced glaucoma happens when high IOP persists, resulting in glaucomatous visual field loss and characteristic optic nerve changes.
This patient is not adequately counseled about the adverse effects of long-term topical corticosteroids and the potency of different corticosteroids. Potent topical corticosteroids are relatively inexpensive and easily available. In India, the sale of topical steroids is estimated to be 20 times that in the United States [12]. However, in Malaysia, there is no data on the sales of OTC topical steroids. We believed there is a need for community-based studies to determine the prevalence of topical anesthetics and corticosteroids use. Stricter laws should be implemented for dispensing topical steroids. General practitioners need to be alerted about the adverse complications and advised to avoid prescribing topical anesthetics and corticosteroids.
Conclusion
Topical anesthetics and corticosteroids abuse can lead to serious complications such as chronic keratitis and endophthalmitis. The availability of topical anesthetics and steroids over the counter must be re-evaluated to prevent such complications. Pharmacy regulations on safe dispensing should be strictly enforced to control and reduce the possibility of topical eye drops abuse or misuse. Ophthalmologists and primary care physicians should be more vigilant in prescribing steroid eyedrops, especially in patients who require long-term steroids. Education on proper usage of topical anesthetics and steroids should also be delivered to the patients to raise public awareness of the destructive sequelae of uncontrolled overuse of these topical drugs.
References
- Al-Khalaileh W, Abu-Farha R, Wazaify M, Van Hout MC. Ophthalmic drug abuse: An observational study from community pharmacies. Res Social Adm Pharm. 2019; 15: 943-948.
- Special Focus: Steroid eye drops abuse; “Self-medication” can lead to blindness, glaucoma. The News Straits Times. 2005.
- Sharifi A, Sharifi H, Karamouzian M, Mokhtari M, Esmaeili HH, et al. Topical ocular anesthetic abuse among Iranian welders: Time for action. Middle East Afr J Ophthalmol. 2013; 20: 336.
- Yagci A, Bozkurt B, Egrilmez S, Palamar M, Ozturk BT, et al. Topical anesthetic abuse keratopathy: A commonly overlooked health care problem. Cornea. 2011; 30: 571-575.
- Varga CJ, Rubinfeld RS, Wolf TC, Stutzman CR, Peele MK, Clifford WS, et al. Topical anesthetic abuse ring keratitis: Report of four cases. Cornea. 1997; 16: 424-429.
- Pharmakakis NM, Katsimpris JM, Melachrinou MP, Koliopoulos JX. Corneal complications following abuse of topical anesthetics. Eur J Ophthalmol. 2002; 12: 373-378.
- Dass BA, Soong HK, Lee B. Effects of proparacaine on actin cytoskeleton of corneal epithelium. J Ocul Pharmacol Ther. 1988; 4: 187-194.
- Rosenwasser GO. Complications of topical ocular anesthetics. Int Ophthalmol Clin. 1989; 29: 153-158.
- Yasir M, Goyal A, Sonthalia S. Corticosteroid Adverse Effects. StatPearls. 2022.
- Charles NJ, Simon D, Helen DM. Locally Administered Ocular Corticosteroids. Drug Saf. 2002; 25: 33-55.
- Cohen A. Steroid Induced Glaucoma. Glaucoma - Basic and Clinical Concepts. 2011.
- Gupta S, Shah P, Grewal S, Chaurasia AK, Gupta V. Steroid-induced glaucoma and childhood blindness. Br J Ophthalmol. 2015; 99: 1454-1456.