
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 4
Clinical manifestations of varicella zoster virus encephalitis in adults: A multifaceted presentation
Xiyang Ji1; Hao Zhu2; Xiaojie Zhang1; Jianbo Zhou1; Ping Chen1*
1Department of Neurology, Xianyang Hospital of Yan’an University, No. 38 Wenlin Road, Xianyang 712000, China.
2Department of Neurology, First Hospital of Xianyang, No. 10, Biyuan Road, Xianyang 712000, China.
*Corresponding Author : Ping Chen
Department of Neurology, Xianyang Hospital of Yan’an University, No. 38 Wenlin Road, Xianyang 712000, China.
Email: cp18291839848@163.com
Received : May 15, 2023
Accepted : Jun 08, 2023
Published : Jun 15, 2023
Archived : www.jcimcr.org
Copyright : © Chen P (2023).
Abstract
Objective: The aim of this study is to investigate the clinical features and outcomes of adult Varicella Zoster Virus (VZV) encephalitis.
Methods: The study analyzed the medical records, imaging results, electrophysiological findings, and prognosis of 9 patients diagnosed with VZV encephalitis.
Results: Nine cases of adult VZV encephalitis were identified. Two of these cases presented with thromboembolic diseases, including one case of venous sinus thrombosis and another case of retinal artery embolism. Three cases displayed brainstem encephalitis, with one of these cases presenting with peripheral nerve damage and another with extensive brain damage in the form of an inflammatory demyelinating pseudotumor with pneumonia. Magnetic Resonance Imaging (MRI) abnormalities were detected in five of the cases. All patients received treatment with ganciclovir and dexamethasone, and after 28 days of treatment, all patients met the clinical cure criteria.
Conclusions: This study highlights that VZV can cause a range of nervous system impairments, including Cerebral Venous Sinus Thrombosis (CVST), brainstem encephalitis, retinal artery thrombosis, inflammatory demyelinating pseudotumors, segmental motor weakness, and Postherpetic Neuralgia (PHN).
Keywords: Varicella zoster virus; Cerebrospinal fluid; Encephalitis; Inflammatory pseudotumor; Cerebral venous sinus thrombosis.
Citation: Ji X, Zhu H, Zhang X, Zhou J, Chen P, et al. Clinical manifestations of varicella zoster virus encephalitis in adults: A multifaceted presentation. J Clin Images Med Case Rep. 2023; 4(6): 2457.
Introduction
Primary infection with VZV is commonly considered a feverish illness accompanied by a vesicular rash in children, but it is rare in adults. Nonetheless, reactivation of VZV in adults is linked to a variety of neurological conditions, including arterial vascular lesions, which can result in ischemic strokes, aneurysms, subarachnoid or cerebral hemorrhages, and carotid dissections. In addition, Adults and immunocompromised patients are more prone to severe infections than healthy children [1,2]. Although it has become widely recognized in recent years that VZV reactivation can cause various acute, subacute, and chronic nervous system conditions, encephalitis caused by VZV is extremely uncommon, affecting only 0.1% to 0.2% of patients with diffuse varicella zoster [3]. In this study, we present relatively rare cases of adult VZV infections resulting in cerebral venous sinus thrombosis, brainstem encephalitis, retinal artery thrombosis, and inflammatory demyelinating pseudotumors.
General materials and methods
This study summarizes the clinical data, imaging, electrophysiological characteristics, and prognosis of patients who were diagnosed with VZV encephalitis and admitted to the Department of Neurology at Xianyang Hospital, Yan’an University between September 2019 and December 2022. A total of 9 adult patients, 7 of whom were male and 2 female, with an average age of 60 (ranging from 42-73) years, were included in the study. The clinical symptoms observed in the patients included vision loss in 6 cases, blurred vision in 3 cases, double vision in 1 case, headache in 4 cases, slow reaction in 1 case, dizziness and walking instability in 5 cases, hoarseness and choking cough in 1 case, limb weakness in 2 cases, and limb numbness in 1 case. Additionally, 5 of the patients were found to have cerebral infarction, 6 had hypertension, and 3 had dermatomal vesicular rash. Lumbar puncture was performed on all patients within 24 hours of admission, and Cerebrospinal Fluid (CSF) was sent for second generation sequencing and PCR before treatment. The general clinical data of these nine patients with nervous system VZV infection and one patient complicated with Human Adenoviruses (HAdVs) was presented in Table 1.
Results
Laboratory and imaging examination results
The results of the examination of 9 patients with nervous system VZV infection indicate that lumbar puncture was performed on all patients. One patient had increased intracranial pressure (250 mm H2O), while 8 patients had CSF leukocytes with an average count of 85 (ranging from 0 to 270) cells/mm3 and a lymphocyte proportion of 85% (ranging from 65-94%). Two patients displayed an elevated level of CSF protein with an average of 1.1 (ranging from 0.29-2.85) g/L, while the CSF chloride and sugar levels were found to be normal.
The MRI of patient No. 1 showed multiple cystic lesions in various parts of the brain, including the left pons, bilateral basal ganglia, bilateral lateral ventricles, and bilateral frontal and parietal lobes. The lesions were mainly located in the white matter, with some appearing to have merged. DWI showed mild diffusion limitation in the cystic wall, but no abnormal enhancement was observed on the contrast-enhanced scan. Interestingly, we also observed the evolution of cranial MRI in the patient of No. 1 from admission to discharge (Figure 1). The head PET/CT of the patient No. 1 revealed multiple low-density intracranial lesions with no obvious edema, a glucose metabolism defect, and an intracranial infection following an inflammatory demyelinating pseudotumor. The patient chest PET/CT scans showed interstitial changes in both lungs, with evidence of emphysema, multiple cord foci in the middle and lower lobe of the right lung and mild bronchiectasis in the lower lobe of the right lung , which may suggest chronic inflammation (Figure 2). The MRI of the patient of No. 2 showed the Diffusion Weighted Imaging Sequence (DWI) showed high signal in the center of pons, which may suggest brainstem encephalitis (Figure 3). The MRV of the patient of No. 4 showed the left transverse sinus and sigmoid sinus to be more slender than the contralateral (Figure 4). Demyelination was seen in 4 patients, while 3 patients had normal MRI results.
Of the 9 patients, visual evoked potential was abnormal in 1 case, brainstem auditory evoked potential was abnormal in 1 case, and somatosensory evoked potential was abnormal in 3 cases. Results for evoked potentials were not collected in 4 cases. The VZV virus was detected in all 9 patients through second-generation sequencing of CSF, and human adenovirus B was detected in the CSF of patient No. 3 (Table 2).
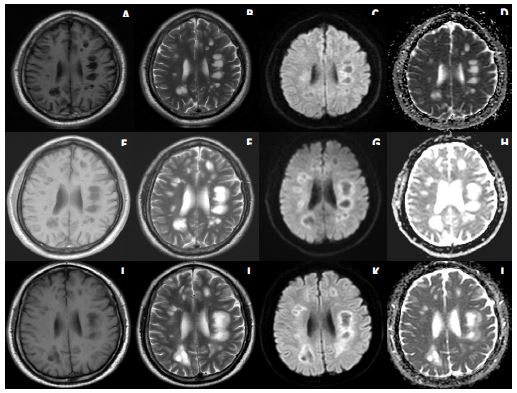
At the time of admission, multiple round cystic lesions were present on the left side of the pons, bilateral basal ganglia, bilateral lateral ventricles, and bilateral frontal parietal lobe (A-D). The diffusion-weighted imaging sequence (DWI) revealed a central low signal shadow with slightly high signal margins, predominantly in the white matter with some lesions appearing to fuse. The apparent diffusion coefficient (ADC) showed high signal.
Two weeks later, the imaging revealed a central low-signal ring with slightly high-signal margins in the DWI, with no diffusion restriction, and some lesions were larger with a necrotic area in the center of the lesion (E-H). The ADC showed a ring shadow with slightly high signal.
At the time of discharge, the MRI showed significant reduction in the size of some lesions, with DWI indicating restricted diffusion in the frontal lobe, the right basal ganglia area, and the pontocerebellum. The ADC showed a slightly higher signal shadow (I-L).

The head PET/CT scans (A-D) revealed multiple low-density lesions in the brain with no visible signs of edema and a glucose metabolism deficit. These findings are indicative of an intracranial infection that presents as an inflammatory demyelinating pseudotumor. The chest PET/CT scans (E-H) showed interstitial changes in both lungs, with evidence of emphysema, multiple cord foci in the middle and lower lobe of the right lung and mild bronchiectasis in the lower lobe of the right lung. There were also multiple enlarged lymph nodes in the mediastinum and bilateral hilum, a higher glucose metabolism and increased density of some lymph nodes, which may suggest chronic inflammation.
Table 1: General clinical data of 9 patients with VZV infection of nervous system.
| Serial number | Gender | Age | Course of the disease (days) | Main symptoms |
|---|---|---|---|---|
| 1 | Male | 56 | 50 | General weakness, slow response, walking instability |
| 2 | Male | 73 | 3 | Headache, dizziness, numbness and weakness of limbs |
| 3 | Female | 66 | 3 | Headache, dizziness, vomiting, walking instability |
| 4 | Male | 49 | 9 | Headache, nausea vomiting, blurred vision, and double vision. |
| 5 | Male | 42 | 31 | Decreased vision in both eyes |
| 6 | Female | 62 | 4 | Dizziness, nausea and vomiting, walking instability |
| 7 | Male | 63 | 7 | Dizziness, nausea and vomiting, walking instability |
| 8 | Male | 63 | 3 | Headache, dizziness, nausea and vomiting |
| 9 | Male | 63 | 7 | Dizziness |
Table 2: Results of cerebrospinal fluid in the 9 patients with VZV infection of nervous system.
| Serial number | Cranial pressure (mmH2O) | CSF-UTP (g/L) | CSF-WBC (/mm3) | CSF-LYMPH (%) | Sequence number of pathogenic microorganism macrogenes | Electrophysiological examination |
|---|---|---|---|---|---|---|
| 1 | 110 | 0.63 | 0 | 88% | VZV 24 | SEP(+),VEP(+),BAEP(-) |
| 2 | 160 | 1.10 | 270 | 82% | VZV 335 | SEP(+),VEP(-),BAEP(+) |
| 3 | 250 | 0.36 | 20 | 90% | VZV 841 and HAdVsB 12 | SEP(+),VEP(-),BAEP(-) |
| 4 | 130 | 1.54 | 141 | 89% | VZV 2 | |
| 5 | 120 | 0.30 | 10 | 94% | VZV 6.67E+06 | |
| 6 | 140 | 0.33 | 10 | 94% | VZV 140 | SEP(-),VEP(+),BAEP(-) |
| 7 | 130 | 0.79 | 100 | 65% | VZV 585 | SEP(-),VEP(-),BAEP(-) |
| 8 | 175 | 2.72 | 110 | 85% | VZV 595 | |
| 9 | 180 | 2.85 | 100 | 81% | VZV 585 |
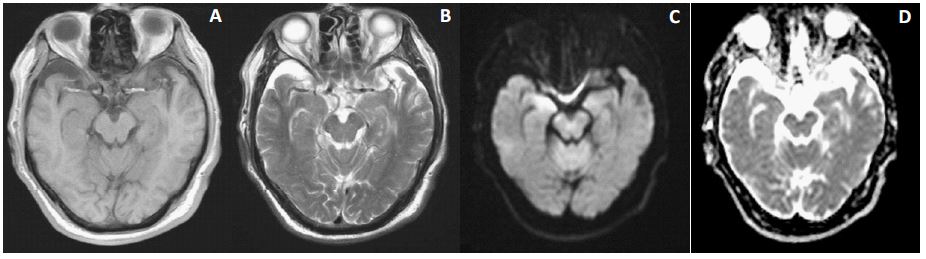
(A,B) Multiple patchy shadows with patchy shadows were observed bilaterally in the basal ganglia, lateral ventricles, and semioval centers. (C) The diffusion-weighted imaging (DWI) sequence showed a high signal in the center of the pons, indicating a new brainstem lesion. (D) The apparent diffusion coefficient (ADC) showed a low signal shadow in the center of the pons.
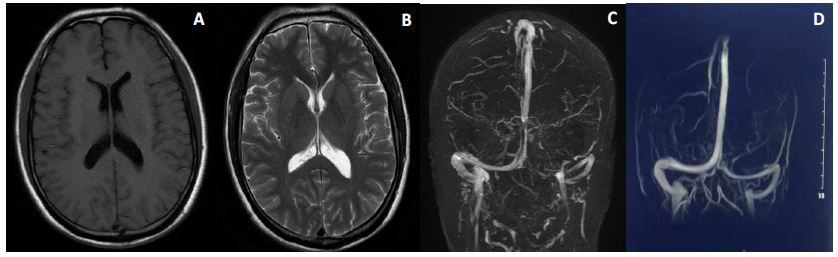
(A-C) Prior to treatment, the MRI indicated a small amount of demyelination in the white matter adjacent to the anterior horn of the lateral ventricle. The MRV also showed thinner left transverse and sigmoid sinuses compared to the contralateral side. (D) Following treatment, the MRV indicated no abnormalities in the bilateral transverse or sigmoid sinuses.
Treatment
All patients received treatment with ganciclovir antiviral and dexamethasone anti-inflammatory drugs. The patient of No. 1 received additional Methylprednisolone 1 g pulse therapy. After 28 days of treatment, all patients were cured and met the clinical cure standard. A 3-month telephone follow-up showed that all patients’ symptoms had improved and there were no recurrences or worsening.
Discussion
VZV is a highly neurotropic, double-stranded DNA human α-herpesvirus that typically causes varicella [4,5], a primary infection that most commonly affects unvaccinated children. The virus usually infects individuals in infancy or adolescence, and serological evidence suggests that 98% of adults have been exposed to the virus. Following primary infection, the virus establishes latency in neurons of the cranial nerve, dorsal root, and autonomic ganglia throughout the nervous system, including the adrenal glands. As cellmediated immunity to VZV declines with advancing age and immunosuppression [6], the virus can reactivate and replicate, spreading along sensory nerve axons to the corresponding skin, leading to skin rash and neuralgia, and upwards to the central nervous system, causing encephalitis or meningitis [7,8].
However, there have been few reports of inflammatory demyelinating pseudotumor caused by adult VZV infection. In our group, the central nervous system lesion of patient No.1 caused by VZV involved brain parenchyma, eventually forming an inflammatory demyelinating pseudotumor. Treatment with corticosteroids was found to be effective in reducing symptoms, with clinical improvement occurring prior to changes observed on head MRI. The size of the lesion appeared to decrease significantly after one month of treatment. However, new punctate lesions may appear during the treatment process, and continued observation of the MRI evolution is necessary.
HadVs are capable of causing a wide range of diseases in both children and adults, including acute respiratory tract infection, gastroenteritis, and epidemic keratoconjunctivitis. Those who are immunocompromised, children, and military recruits are particularly susceptible to adenovirus infections. There are currently 7 species (A-G) that encompass more than 79 genotypes. Among them, HAdV-B3 and B7 are the most commonly associated with respiratory tract infections [9-11]. In our group, second-generation sequencing of CSF from patient No. 3 detected the presence of both VZV and HAdVs B, whose response to treatment was initially slow but eventually improved within 28 days.
VZV has been associated with cerebral artery disease, purpura outbreaks, and extensive thromboembolism, which are thought to be related to acquired antibody-mediated coagulation disorders [12,13]. However, reports of primary VZV infection causing CVST are rare. In our group, patient No. 4 had thinner left transverse and sigmoid sinuses on MRV before treatment, suggesting the possibility of CVST. After one week of anticoagulant treatment, MRV showed normal bilateral transverse and sigmoid sinuses. Additionally, patient No. 5 had primary VZV infection and central retinal artery thrombosis. Therefore, we conclude that primary VZV infection may be related to both cerebral artery and venous sinus thrombosis.
It has been reported that herpes zoster most commonly affects the distribution of the trigeminal nerve and facial nerve, with the vestibulocochlear nerve also commonly affected [14,15]. Along with facial palsy and external auditory canal vesicles and rashes, vestibulocochlear neuropathy such as tinnitus, hearing loss, and vertigo can occur. In our group, patient No. 3 had facial paralysis, which was considered to be caused by VZV involving the facial nerve. When zoster affects the ophthalmic division of the trigeminal nerve, local ocular complications such as keratitis, scleritis, iritis, retinitis, optic neuritis and glaucoma can follow [7,16]. In our group, patients No. 5, No. 7, and No. 9 involved the ophthalmic branch of the trigeminal nerve and were complicated with iritis and keratitis, which is consistent with literature reports.
As is well known, PHN typically occurs in patients who have had herpes zoster and is usually localized to the area where the herpes zoster rash has healed, with varying degrees of pain severity. The incidence and prevalence of PHN tend to increase with age [17]. Autopsy studies have shown that VZV is present in the trigeminal ganglion in 97.1% of cases [18]. Among the three branches of the trigeminal nerve, the incidence of herpes zoster in the ophthalmic branch (V1) is 19% [19], which is 20 times higher than in the maxillary ramus (V2) and mandibular ramus (V3) [20]. In our group, patients No. 5, 7, and 9 experienced front oparietal pain one week after herpes healing, likely due to involvement of the ophthalmic branch of the trigeminal nerve. After treatment with gabapentin, their symptoms significantly improved.
Therefore, for patients suspected of VZV infection, particularly those without typical rashes and complicated with conditions such as CVST, brainstem encephalitis, retinal artery thrombosis, inflammatory demyelinating pseudotumor, and peripheral nerve injury, it is recommended to perform lumbar puncture and enhance the second-generation sequencing of CSF to identify pathogens. This will aid in guiding clinical medication and evaluating prognosis.
References
- Nagel MA, Gilden D. Update on varicella zoster virus vasculopathy [J]. Current infectious disease reports. 2014; 16: 407.
- Gershon AA, Chen J, Gershon MD. Use of Saliva to Identify Varicella Zoster Virus Infection of the Gut [J]. Clinical infectious diseases: An official publication of the Infectious Diseases Society of America. 2015; 61: 536-544.
- Ellis DL, Barsell A, Riahi RR, et al. Varicella zoster virus encephalitis in a patient with disseminated herpes zoster: report and review of the literature [J]. Dermatology online journal. 2014; 21.
- Nagel MA, Gilden D. Neurological complications of varicella zoster virus reactivation [J]. Current opinion in neurology. 2014; 27: 356-60.
- Nagel MA, Gilden D. Developments in Varicella Zoster Virus Vasculopathy [J]. Current neurology and neuroscience reports. 2016; 16: 12.
- Amlie-Lefond C, Gilden D. Varicella Zoster Virus: A Common Cause of Stroke in Children and Adults [J]. Journal of stroke and cerebrovascular diseases: The official journal of National Stroke Association. 2016; 25: 1561-1569.
- Kennedy PGE, Gershon AA. Clinical Features of Varicella-Zoster Virus Infection [J]. Viruses, 2018; 10.
- Badani H, White T, Schulick N, et al. Frequency of varicella zoster virus DNA in human adrenal glands [J]. Journal of neurovirology. 2016; 22: 400-402.
- Chen S, Tian X. Vaccine development for human mastadenovirus [J]. Journal of thoracic disease. 2018; 10: S2280-S2294.
- Chen M, Zhu Z, Huang F, et al. Adenoviruses associated with acute respiratory diseases reported in Beijing from 2011 to 2013 [J]. PloS one. 2015; 10: e0121375.
- Guo L, Gonzalez R, Zhou H, et al. Detection of three human adenovirus species in adults with acute respiratory infection in China [J]. European journal of clinical microbiology & infectious diseases : official publication of the European Society of Clinical Microbiology. 2012; 31: 1051-1058.
- Zerboni L, Sen N, Oliver S L, et al. Molecular mechanisms of varicella zoster virus pathogenesis [J]. Nature reviews Microbiology. 2014; 12: 197-210.
- Gunturu M, Gosi SK, Kanduri S, et al. Varicella Zoster Meningitis, Optic Neuritis Preceding the Development of Posterior Outer Retinal Necrosis, and Central Retinal Artery Occlusion in a HIV Patient [J]. Case reports in medicine. 2019; 2019: 4213162.
- Tsau PW, Liao M F, Hsu J L, et al. Clinical Presentations and Outcome Studies of Cranial Nerve Involvement in Herpes Zoster Infection: A Retrospective Single-Center Analysis [J]. Journal of clinical medicine. 2020; 9.
- Gilden D, Nagel MA, Cohrs RJ. Varicella-zoster [J]. Handbook of clinical neurology, 2014, 123: 265-83.
- Gershon AA, Breuer J, Cohen JI, et al. Varicella zoster virus infection [J]. Nature reviews Disease primers. 2015; 1: 15016.
- Kawai K, Gebremeskel BG, Acosta CJ. Systematic review of incidence and complications of herpes zoster: Towards a global perspective [J]. BMJ open. 2014; 4: e004833.
- Inoue H, Motani-Saitoh H, Sakurada K, et al. Detection of varicella-zoster virus DNA in 414 human trigeminal ganglia from cadavers by the polymerase chain reaction: A comparison of the detection rate of varicella-zoster virus and herpes simplex virus type 1 [J]. Journal of medical virology, 2010; 82: 345-349.
- Wulf H, Maier C, Schele HA. [The treatment of zoster neuralgia] [J]. Der Anaesthesist. 1991; 40: 523-529.
- Kaufman SC. Anterior segment complications of herpes zoster ophthalmicus [J]. Ophthalmology, 2008; 115: S24-32.