
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A rare presentation of idiopathic distal radial artery aneurysm in anatomical snuff box in a 40 year old male
Dr. Sai Sampath Kumar Vasantham1*; Dr. Jameel Akhter*2; Dr. Priyadarshini kumarswamy3
1Department of General Surgery Resident, Apollo Hospitals Chennai, India.
2Department of Consultant Surgeon, Apollo Hospitals Chennai, India.
3Department of Cardiothoracic and Vascular Surgery Resident, Apollo Hospitals Chennai, India.
*Corresponding Author : Dr. SSK Vasantham
Department of General Surgery Resident, Apollo Hospitals, Chennai, India.
Tel: +91-21879382
Email: saimbbsdavao2013@gmail.com
Dr. Jameel Akhter
Department of General Surgery, Consultant Surgeon, Apollo Hospitals Chennai, India.
Received : May 19, 2023
Accepted : Jun 12, 2023
Published : Jun 19, 2023
Archived : www.jcimcr.org
Copyright : © Vasantham SSK & Akhter J (2023).
Abstract
True non- traumatic radial artery aneurysms (RAAs) are uncommon; just a small number of cases have been reported. The majority are iatrogenic pseudo-aneurysms caused by arterial cannulation and have traumatic origins. There have also been reports of other uncommon causes include vascular tumors, connective tissue disorders, and industrial injuries. Only eight cases of true idiopathic Radial artery aneurysms were reported as of 2018. Snuffbox radial artery aneurysms are even more uncommon. Here we present a case of an 59-year-old male, with no previous history of trauma, presenting with right wrist swelling, upon investigating with MRI was suspected to have ganglion cyst, patient underwent excision, on table the swelling was pulsatile and was suspected to have Radial Artery Aneurysm, a vascular surgeon opinion was taken and was managed by surgical repair with out reconstruction. Post operative patient didn’t develop any ischemia or neurological deficits and was discharged.
Keywords: Radial artery aneurysms; Iatrogenic; Anatomical snuffbox; Surgery.
Citation: Vasantham SSK, Akhter J, kumarswamy P. A rare presentation of idiopathic distal radial artery aneurysm in anatomical snuff box in a 40 year old male. J Clin Images Med Case Rep. 2023; 4(6): 2462.
Introduction
Rare radial artery aneurysms frequently result from penetrating or intentional injury to the wrist [1]. There have only been 20 occurrences of snuffbox radial artery aneurysms described till date, making them even more rare [1]. The radial artery is relatively superficial and unprotected in the anatomical snuffbox, a triangular depression between the extensor pollicis longus and extensor pollicis brevis tendons [2]. Because of it rarity, diagnosis is difficult to make, and treatment differs with each diagnosis.
Case presentation
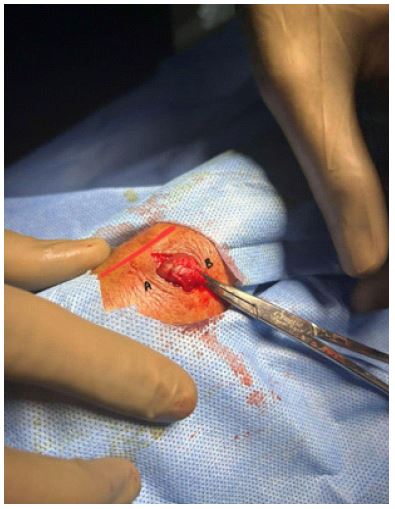
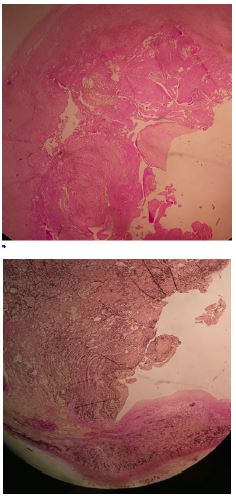
A 59-year-old male came to the outpatient services at Apollo Main Hospitals, Chennai, with wrist pain since one month. The patient had a history of right wrist swelling since 5 years, with gradual increase in size of the swelling. No other significant history was noted. He gave history of pain and difficulty in performing routine activities. There was no history of numbness or tingling sensation in lateral aspect of the hand. There was no history of trauma, previous cannulation or surgery. On physical examination, swelling was solitary, smooth, soft, cystic, well defined margins, located in the right anatomical snuff box, measuring 2 x 2 cm, skin over the swelling was normal. The swelling on examination was non pulsatile and no bruit was detected, but with regard to the differential diagnosis radial artery aneurysm needed to be ruled out. He was evaluated with MRI which was suggestive of non-conclusive soft tissue swelling. As imaging was inconclusive, patient was offered surgical excision of the swelling, Under local anesthesia, an vertical incision was made over the swelling, tissues opened in layers and swelling was exteriorised. It was then noticed that the swelling was pulsatile with findings consistent with an aneurysm (Figure 1). Intraoperatively vascular surgeon opinion was obtained. Patient was explained about the findings. After performing Allen’s test and confirming the patency of ulnar artery, the swelling was meticulously dissected and doubly lighted both proximally and distally, excised in toto and sent for Histopathology. Since the aneurysm was smaller in size and patency of the ulnar artery was good, the excision was not followed by reconstruction of the artery. Post operative period was uneventful, patient did not develop any tingling sensation or digital gangrene. Patient was advised CT Angiogram to rule out any other missed aneurysms. Histopathology findings were conclusive of true Radial artery true aneurysm bound by all three layers of the vessel wall (intima, media and adventitia) (Figure 2).
Discussion
Upper extremity arterial aneurysms are rare [1,2]. Radial artery aneurysms account for only 2.9% of all upper- extremity aneurysms [3]. The majority of radial artery aneurysms that had perviously been documented were pseudoaneurysms in the wrist brought on by trauma from arterial cannulation or cardiac interventional operations. However, idiopathic radial artery aneurysms are quite uncommon [4]. Snuff box radial artery aneurysms have been recorded in a total of 20 occurrences to date. In the anatomical snuff box, 16 cases of radial artery aneurysms were discovered as of 2016. Four other instances were reported between January 2016 to January 2022 [5-7].
In the current case, the cause of distal radial artery aneurysm was unknown. Based on normal inflammatory marker levels and an analysis of the aneurysm’s histology, the likelihood of an connective tissue problem or inflammatory condition was ruled out. Extensor pollicis longus tendon compression on the radial artery, according to Halbach et al., may have a role in the development of an idiopathic aneurysm [6]. A true radial artery aneurysm in a tailor was documented by Behar et al., as a result of recurrent industrial damage [7]. Other reported cases of aneurysms describe trauma, infection, connective tissue disease, or atherosclerosis as the etiological factors [8].
Clinical examination might provide the initial diagnosis [4]. In majority of cases, a pulsatile swelling is the first sign. Apart from that, nerve irritation, paresthesia, restricted wrist movement, distal thrombosis, digital ischemia, rupture, hemarthrosis, skin ulceration, and secondary infection are other problems that may appear [4]. This condition can be often confused with ganglion cyst. Other differential diagnosis includes synovial cyst, lipomas, and neuromas [2].
This condition can be preoperatively diagnosed using angiography, it also helps in identifying other vascular pathologies, such as arteritides, arteriovenous fistulas and malformations, fibromuscular dysplasia and venous anomalies [9]. Duplex ultrasonography can play an important role in distinguishing true arterial aneurysms from pseudoaneurysms and the quality of in-line flow [9].
Resection of the aneurysm and arterial reconstruction with primary end-to-end anastomosis or proximal and distal ligature of the vessel appears to be the preferred approach in cases where the ulnar artery is the dominant arterial supply for the hand [10]. The most common approach for Radial artery an eurysms is ligation and excision, which appears to be the preferred approach [11]. Transcatheter therapeutic options such as covered stent exclusion, coil, polymerizing agent embolization are extremely limited and ill advised given the local anatomical restrictions [12]. In the case described here, the location of the aneurysm is within the anatomical snuffbox and affecting the distal radial artery, vascular surgeon opinion was obtained and decision was made to do ligation and excision of the aneurysm, following which distal flow was well maintained and patient developed no complications.
Conclusion
Idiopathic distal radial artery aneurysms of the anatomical snuffbox and extremely rare in presentation, and can be misdiagnosed with a synovial or ganglion cyst. Through preoperative evaluation shall be performed and patient education is necessary. Patient shall be advised to have regular follow up because idiopathic aneurysms can occur anywhere in the body.
References
- Ho PK, Weiland AJ, McClinton MA, Wilgis EF. Aneurysms of the upper extremity. J hand Surg Am. 1987; 12: 39-46.
- Ogeng’o JA, Otieno B. Aneurysms in the arteries of the upper extremity in a Kenyan population. Cardiovascular Pathology. 2011; 20: e53-56.
- Walton NP, Chaudhary F. Idiopathic radial artery aneurysm in the anatomical snuffbox. Acta Orthop Belg. 2002; 68: 292-294.
- Yamamoto Y, Kudo T, Igari K, Toyofuku T, Inoue Y. Radial artery aneurysm in the anatomical snuffbox: A case report and literature review. International journal of surgery case reports. 2016; 27: 44-47.
- Halbach J, Lowry D, Nelles M, Ayers J. Extensor pollicis longus tendon compression as the etiology of a true aneurysm of the radial artery in the anatomical snuffbox. Journal of Vascular Surgery Cases, Innovations and Techniques. 2016; 2: 152-154.
- Ghaffarian AA, Brooke BS, Rawles J, Sarfati M. Repair of a symptomatic true radial artery aneurysm at the anatomic snuff box with interposition great saphenous vein graft. J Vasc Surg Cases Innov Tech. 2018; 4: 292-295.
- Behar JM, Winston JS, Knowles J, Myint F. Radial artery aneurysm resulting from repetitive occupational injury: Tailor’s thumb. European Journal of Vascular and Endovascular Surgery. 2007; 34: 299-301.
- Umeda Y, Matsuno Y, Imaizumi M, Mori Y, Iwata H. et al. Bilateral radial artery aneurysms in the anatomical snuffbox seen in Marfan syndrome patient: case report and literature review. Annals of Vascular Diseases. 2009; 2: 185-189.
- Shaabi HI. True idiopathic saccular aneurysm of the radial artery. J Surg Case Rep. 2014; 2014: rju058.
- Gabriel SA, Abreu MF, Abreu GC, Simoes CR, Chrispim AC, et al. True posttraumatic radial artery aneurysm. Jornal Vascular Brasileiro. 2013; 12: 320-323.
- Thai H, Vasyluk A, Rits Y. Bilateral radial artery aneurysm: case report and review of literature. Vasc Med Surg. 2016; 4: 247.
- Nassiri N, Kogan S, Truong H, Nagarsheth KJ, Shafritz R, et al. Surgical repair of a snuffbox radial artery pseudoaneurysm. Clin Surg. 2016; 1: 1154.