
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Otologic presentation of nasal rhinosporidiosis: A clinical picture
Marlapudi Sudheer kumar1*; Roohie Singh1; Jeenu Varghese2; Sanjay Kumar1; Angshuman Dutta1
1Department of ENT-HNS, Command Hospital Airforce, Bangalore, India.
2Department of Pathology, Command Hospital Airforce, Bangalore, India.
*Corresponding Author : Marlapudi Sudheer Kumar
Department of ENT, Command Hospital Airforce, Bangalore, India.
Tel: +91-8121525345;
Email: sudheerjoel.medico@gmail.com
Received : May 15, 2023
Accepted : Jun 13, 2023
Published : Jun 20, 2023
Archived : www.jcimcr.org
Copyright : © Kumar MS (2023).
Citation: kumar MS, Singh R, Varghese J, Kumar S, Dutta A. Otologic Presentation of Nasal Rhinosporidiosis: A Clinical Picture. J Clin Images Med Case Rep. 2023; 4(6): 2464.
Clinical image description
25 year, male, pilot by profession presented with complaints of blockage and pain in (R) ear for 2 weeks. Otoendoscopic examination revealed fluid menisci behind (R) Tympanic membrane (Figure 1a). On Diagnostic nasal endoscopy, a bluish-grey mass arising near (R) inferior meatus was seen extending posteriorly over the nasal floor with a pinkish hue with multiple white spots (classical strawberry appearance) over the surface (Figure 1b). (R) eustachian tube orifice opening was occluded due to extension of mass into the nasopharynx. Endoscope-assisted posterior rhinoscopy revealed a pedunculated mass with multiple white spots over the surface hanging from (R) choana (Figure 1c)
Concomitant CECT and MRI of paranasal sinuses and nasopharynx revealed a soft tissue lesion epicentered around (R) Inferior meatus extending along the nasal floor into the nasopharynx. The patient underwent Endonasal endoscopic excision of nasal mass in toto. Histopathological examination was (Figures 2a,2b,2c) consistent with Rhinosporidiosis. Postoperatively the patient was started on Tablet Dapsone 100 mg once daily for 06 months
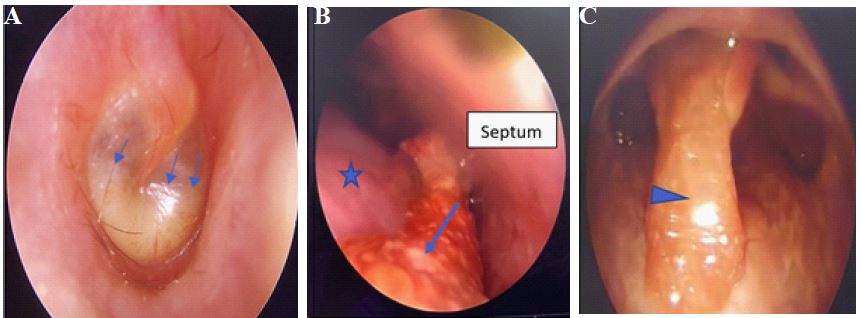
(B) Mass with white spots (arrow) over the surface along (R) inferior turbinate (star) and floor of nose.
(C) Endoscope assisted posterior rhinoscopy showing nasopharyngeal mass (arrow head) with white spots over the surface.

(B) AS stain 10 x - Variably sized thick-walled PAS positive sporangia, with numerous microspores within (black arrows). Each measuring 6-7 microns.
(C) GMS Stain 10x - Sporangia are highlighted in GMS stain (yellow arrows).
Discussion
Rhinosporidiosis is a chronic granulomatous infection of the mucus membranes. It grows in stagnant waters and infects humans by gaining access through the traumatized epithelium and lining mucosa. The characteristic lesion is a painless friable polypoid vascular mass, which may be pedunculated or sessile with surface studded with tiny white dots from spores beneath the epithelium, giving it a “strawberry-like” appearance [1,2].
Differential diagnosis include antrochoanal polyp with squamous metaplasia, inverted papilloma, extra nasopharyngeal angiofibroma, etc., [2]. Rhinosporidiosis is most easily and definitively diagnosed via microscopy. No culture media for the isolation of Rhinosporidium seeberi are available.
Wide local surgical excision of the lesions and electrocautery of the base of the lesions is the most acceptable and successful treatment modality [3]. Recurrence is known to occur in 10% of cases after excision, the only drug that appears to have a promising result when used in the postoperative period is, Dapsone [3].
Declarations
Conflicts of interest: Nil
Research involving human participants and/or animals: Nil
Informed consent: Informed consent was taken from the patient for this publication.
Funding: No funding was received to assist with the preparation of this manuscript. The authors have no relevant financial or non-financial interests to disclose.
References
- Das, Shukla; Kashyap, Bineeta; Barua, Madhumita; Gupta, Neelima; Saha, Rumpa; Vaid, Lakshmi; Banka, Alok (2011). Nasal rhinosporidiosis in humans: new interpretations and a review of the literature of this enigmatic disease. Medical Mycology. 2011; 49: 311-315.
- Venkatachalam VP, Anand N, Bhooshan O. Rhinosporidiosis: Its varied presentations. Indian J Otolaryngol Head Neck S. 2007; 59: 142-144.
- International Journal of Advances in Medicine Majumdar AB et al. Int J Adv Med. 2014; 1(3): 213-216.