
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A case of complicated falciparum malaria from coming back from Myanmar-India border presenting with cerebral malaria, black water fever, acute kidney injury, metabolic acidosis, hypocalcemia, severe anemia, thrombocytopenia and hepatitis having early parasitological failure on Day 14: Awareness on dihydroartemisinine-piperaquine combination therapy
Khin Phyu Pyar1*; Moe Zaw Myint2; Sai Aik Hla2; Soe Win Hlaing2; Soe Min Aung2; Zar Ni Htet Aung2; Nyan Lin Maung2; Aung Phyoe Kyaw2; Thurein Win2; Aung Aung2; Thein Tun Myint2; Kyaw Thet Maung2; Han Lin Aung3; Myo Thant Kyaw3; Zay Phyo Aung3; Kyaw Thuyein Lwin4; Lynn Htet Aung5; Lay Maung Maung4; Ye Min Hein4; Moe Tun Zaw4; Myo Maung Maung4; Thein Aung Moe2; Kaung Myat Oo4; Myat Ko5; Htet Aung5; Zin Min Htet6
1Professor and Head/Senior Consultant Physician, Department of Medicine/ Department of Nephrology, Defence Services Medical Academy/ No.(1) Defence Services General Hospital (1000-Bedded), Myanmar.
2Consultant Physician, No. (1) Defence Services General Hospital (1000-Bedded), Myanmar.
3Assistant Lecturer / Consultant physician, Defence Services Medical Academy, Myanmar.
4Consultant Nephrologist, No. (1) Defence Services General Hospital (1000-Bedded), Myanmar.
5Consultant Pathologist, No. (1) Defence Services General Hospital (1000-Bedded), Myanmar.
6Consultant Microbiologist, No. (1) Defence Services General Hospital (1000-Bedded), Myanmar.
*Corresponding Author : Khin Phyu Pyar
Department of Medicine, Defence Services Medical Academy, Mingalardon 11021, Myanmar.
Email: khinphyupyar@gmail.com
Received : Apr 07, 2023
Accepted : Jun 15, 2023
Published : Jun 22, 2023
Archived : www.jcimcr.org
Copyright : © Pyar KP (2023).
Abstract
A-39-year-old migrant worker coming back from Palatwa (Sagaing Division) and Myanmar-India border area (Rakhine State) developed cerebral malaria, acute kidney injury and metabolic acidosis. He was treated with intravenous artemisinine followed by ACT (artemisinine combination therapy); Dihydroartemisinine- piperaquine, hemodialysis, fresh blood transfusion. He had early parasitological failure on Day 14; therefore, different ACT (Artemether-lumefantrine) was initiated. He had adequate clinical and parasitological response till Day 42.
Keywords: Migrant worker; Border area; Complicated falciparum malaria; Early parasitological failure.
Citation: Pyar KP, Myint MZ, Hla SA, Hlaing SW, Aung SM, et al. A case of complicated falciparum malaria from coming back from Myanmar-India border presenting with cerebral malaria, black water fever, acute kidney injury, metabolic acidosis, hypocalcemia, severe anemia, thrombocytopenia and hepatitis having early parasitological failure on Day 14: Awareness on dihydroartemisinine-piperaquine combination therapy. J Clin Images Med Case Rep. 2023; 4(6): 2468.
Introduction
Malaria is caused by Plasmodium species; severe clinical manifestation is commonly seen with Plasmodium falciparum and extremely rare with Plasmodium vivax. The incidence of malaria has been falling in Myanmar as well as South East Asia for nearly one decade. In fact, Myanmar has been trying for malaria free by 2030 [1,2]. Artemisinin resistance has been threatening not only to SEA but also to Western countries; containment of artemisinine was done in 2014 with many challenges [3].
Case presentation
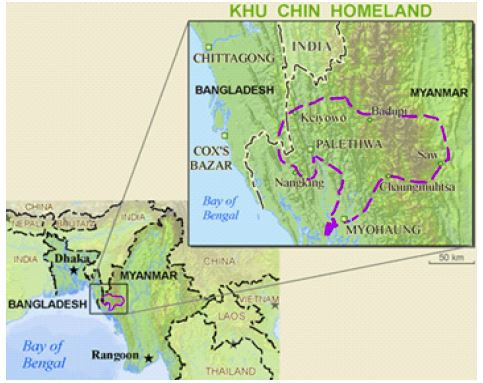
A-39-year-old migrant worker was transferred from Sittwe (Rakhine State) in state of unconsciousness, anuria and severe anemia following 3 days history of fever. He was from Htarwei (Tanintharyi State); and, he visited to Palatwa (Sagaing Division) and Myanmar- India border area (Rakhine State) for 3 months.
On arrival, his Glasgow Coma Scale was 6/15 with equivocal plantar response with loss of eye lid reflexes; he was very pale; temperature was 370C; SaO2 92% on air; respiratory rate was 32/minutes; blood pressure was 110/70 mmHg; pulse rate was 110/minutes; lungs were clear; abdomen was soft; liver was enlarged 3 cm; spleen was not enlarged; and, indwelling urinary catheter had only 20 cc of brownish urine.
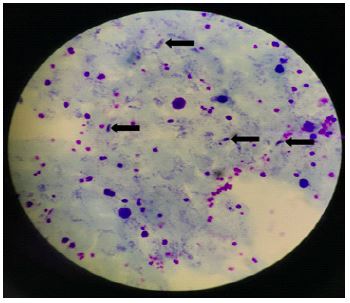
Blood for malaria parasite was 4224/UL; random blood sugar was 154 mg%; blood urea was raised 5 times (247 mg/dl); serum creatinine was raised 5 times (6.7 mg/dl); electrolytes were normal; hemoglobin was low (9.8 gm%); Hct was 27.1%; Total WBC was normal (8.85 x 109/L) with relative monocytosis (10.7%); platelet count was very low (30 x 109/L) normal differential count; AST was raised three times (82.7 U/L ); serum calcium was low (8.7 mg%); and, CRP was normal. His blood was inspected for evidence of severe intravascular hemolysis; the serum was brownish with low red cell part. Serial estimation till day 3 revealed improvement in hemolysis and serum was yellowish reflecting jaundice.
He was treated as cerebral malaria, acute kidney injury, metabolic acidosis, hypocalcemia, severe anemia, thrombocytopenia and hepatitis with intravenous artemisinine. Renal replacement therapy (hemodialysis) was done on arrival to combat metabolic acidosis. Fresh blood was transfused to correct thrombocytopenia and anemia. Initial intravenous artemisinine was followed by ACT (artemisinine combination therapy); Dihydroartemisinine-piperaquine.
He was apyrexial throughout hospital stay. The color of black urine gradually faded and it was normal on Day 7. He became fully conscious and orientated on Day 10 and renal recovery on Day 14. Blood for malaria parasite was done daily to monitor parasitological response; it was negative on Day 5. Then, it was done weekly after 3 consecutive negative for 3 days. He had early parasitological failure on Day 14 with the parasite count of 5,000/UL; therefore, different ACT (Artemether-lumefantrine) was initiated. After 48 hours, blood for malaria parasite was negative; he had adequate clinical and parasitological response till Day 42.
Discussion
The incidence of malaria has been falling in Myanmar; therefore, diagnosis can be missed if travel history is not clerked. Moreover, severe manifestation of Plasmodium falciparum was rarely seen. History of travelling is important as well as awareness of diagnosis of cerebral malaria. Otherwise, the patient cannot be saved and diagnosis can be made only in autopsy [4]. Mortality rate of severe falciparum malaria is high even with treatment. This is the main reason for presenting case.
This patient did not have high parasite count; however, he did have severe manifestation and multi-organ involvement. Several studies pointed out that the higher the parasite count, the more severe the disease manifestation; hyper parasitemia itself is one of the criteria of complicated alaria. The severity of disease may be exacerbated by both higher parasite burdens and the tissue-specific patterns of infected RBC [5].
The mortality rate of cerebral malaria was high [6]; and the patient recovered. Falling conscious level in cerebral malaria was due to various pathological changes: mechanical microvascular obstruction by sequestered infected erythrocytes, activation of immune cells and release of pro-inflammatory cytokines, endothelial dysfunction, dysregulation of coagulation pathways, derangement in Blood–Brain Barrier (BBB) permeability, and brain swelling [7,5,3]. In this patient, CT scan of head was normal; MRI brain was not performed though it could detect changes in cerebral malaria [8,9]. The patient gained fully conscious and oriented only on Day 12. Regarding the duration and severity of unconsciousness in cerebral malaria, it is difficult to say exactly because it was influenced by several factors: the severity of parasitemia in peripheral blood as well as that of microcirculation; the degree of cytokine storm; electrolytes particularly intracellular sodium; hypocalcemia; hypoglycemia; metabolic acidosis in cellular level; CSF lactate; secondary effects from other organ involvement like acute kidney injury; degree of hepatitis; anemia; hypoxia; acute lung injury; concomitant septicemia; hyperpyrexia; hypoxic effect if the patient has convulsion; and effects of drugs like anti-convulsant and sedatives.
Black water fever in malaria became recurring according to some reports. Having black water fever in children from Uganda was reported to have high risk of death [10]. The patient had anuria for 48 hours and the urine color was black/prune juice. Black water fever was due to massive intravascular hemolysis of parasitized RBC both young and old; it was more pronounced in those with G6PD deficiency [11]. Some reports mentioned possible immune mechanism and it was related with anti-malaria drugs; artemisinin derivatives (Dihydroartemisinine-piperaquine) [12]; lumefantrine [13]; and quinine [14]. G6PD enzyme level was normal in this patient; his parasite count was not high. One report pointed out thatblack water fever was not frequently seen in patient with low parasite count; the mechanism was not clearly understood [15]. It also aggravated acute kidney in several ways: acute tubular necrosis; dehydration; hypotension; and possibly direct damage effect on kidney. Thus, the patient required renal replacement therapy till Day 11.
The overall mortality of adult cerebral malaria was reported as 15-20% and it was also influenced by associated vital organ dysfunction. The risk of death increased 3-fold in the presence of acidosis and renal failure [16]. Therefore, it is another reason for case presentation.
The patient had moderate anemia which was refractory and required correction with blood. Moreover, presence of thrombocytopenia also reflected bone marrow depressant effect of falciparum malaria. Having normal BT, CT, PT and D dimer excluded DIC in this patient.
Table 1: Clinical progress.
| Parameter | Day 0 | Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | Day 6 | Day 7 | Day 8 | Day 9 | Day 10 | Day 11 | Day 12 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| GCS | 6 | 6 | 6 | 8 | 8 | 8 | 8 | 12 | 12 | 12 | 14 | 14 | 15 |
| Urine output (cc/24 hr) | 5 | 5 | 5 | 100 | 500 | 950 | 900 | 1650 | 2100 | 2700 | 2050 | 2500 | 3200 |
| Urine color | Black | Black | Black | Black | Black | Black | Brown | Brown | Brown | brown | Yellow | Yellow | Yellow |
| Hemodialysis | + | + | + | + | + | ||||||||
| Blood/blood product transfusion | + | + | + | ||||||||||
| Fits | + | + | + | ||||||||||
| Anemia | + | + | + | + | + | + | + | + | + | + | + | + | + |
| Jaundice |
Table 2: Changes in hematological parameter
| Parameter/Day | D0 | D1 | D2 | D3 | D6 | D8 | D9 | D11 | D13 | D14 | D16 | D17 | D19 | D30 | D38 | D50 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Blood transfusion | + | + | + | |||||||||||||
| Hb (gm%) | 9.8 | 10.4 | 9.3 | 8.3 | 7.8 | 8.3 | 7.9 | 7.8 | 7.1 | 7.4 | 6.6 | 8.0 | 8.1 | 8.0 | 10.0 | 12.3 |
| Hct (%) | 27.1 | 29.5 | 26.2 | 23.2 | 22 | 24.2 | 22.6 | 22.3 | 20.8 | 21.0 | 18.7 | 23.6 | 23.6 | 23.0 | 29.6 | 35.5 |
| TWBC (x109/L) | 8.6/td> | 11.6 | 10.1 | 11.6 | 8.9 | 9.8 | 13.9 | 9.2 | 6.8 | 7.6 | 6.3 | 5.7 | 7.9 | 9.0 | 6.0 | 5.9 |
| N% | 72.4 | 71.6 | 63.3 | 67.1 | 75.1 | 69.3 | 83.9 | 72.9 | 63 | 66.5 | 65.9 | 63.4 | 66.3 | 71.9 | 55.6 | 61.6 |
| L% | 16.9 | 21.3 | 28.6 | 27.7 | 20.5 | 24.7 | 12.2 | 21.9 | 30.5 | 26.2 | 28.1 | 30.4 | 28.3 | 23.2 | 37.7 | 31.8 |
| M% | 10.7 | 7.1 | 8.1 | 5.2 | 4.4 | 6 | 3.9 | 5.2 | 6.5 | 7.3 | 6 | 6.2 | 5.4 | 4.9 | 6.7 | 6.6 |
| E% | ||||||||||||||||
| Platelet (x109/L) | 31 | 75 | 111 | 172 | 259 | 398 | 394 | 390 | 338 | 348 | 273 | 248 | 214 | 271 | 265 | 204 |
Table 3: Renal profile.
| Parameter/ Day | D 0 | D 1 | D 2 | D 3 | D 6 | D 8 | D 9 | D 11 | D 13 | D 14 | D 16 | D 17 | D 19 | D 30 | D 38 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sugar (mg%) | 154 | 160 | |||||||||||||
| Hemodialysis | + | + | + | + | + | ||||||||||
| Urea (mg/dl)(10-50) | 247 | 166.2 | 222 | 207 | 209 | 140 | 93 | 114 | 96.5 | 110 | 57 | 38.4 | 34 | 52 | 19.9 |
| Creatinine (mg/dl) (0-1.3) | 6.7 | 5.4 | 6.2 | 6.2 | 7.4 | 7.0 | 6.1 | 7.2 | 4.5 | 3.8 | 1.9 | 1.5 | 1.5 | 1.3 | 0.88 |
| Na (mmol/L) (135-145) | 143 | 142 | 142 | 142 | 138 | 141 | 142 | 141 | 137 | 138 | 133 | 140 | 136 | 136 | 137 |
| K (mmol/L) (3.5-5.5) | 5.2 | 4.1 | 5.5 | 5.2 | 4.9 | 4.7 | 3.9 | 3.9 | 3.5 | 3.2 | 3.3 | 3.9 | 3.9 | 4.2 | 4.2 |
| Cl (mmol/L) (95-105) | 111.8 | 105.9 | 104.3 | 103.2 | 101.7 | 104.2 | 103.1 | 106.3 | 97.6 | 103 | 98 | 104 | 102 | 98.5 | 101 |
| Ca (mg/dL) (8.6-10.2) | 7.36 | 7.85 | |||||||||||||
| Corrected Ca (8.6-10.2) | 8.4 | 9.2 | |||||||||||||
| PO4 (mmol/L) (0.81-1.45) | 2.03 | 2.3 | |||||||||||||
| CK (U/L) (39-308) | 3041 | 640 | 378 | ||||||||||||
| Total protein (gm/L) (62-80) | 51.8 | 55 | |||||||||||||
| Albumin (gm/L) (38-54) | 23.5 | 21.3 |
Table 4: Liver profile.
| Parameter | D 0 | D 1 | D 2 | D 3 | D 6 | D 8 | D 9 | D 11 | D 13 | D 14 | D 16 | D 17 | D 19 | D 30 | D38 | D 50 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total Bilirubin (mg/dL) (0-1) | 0.9 | |||||||||||||||
| AST (U/L) (0-37) | 82.7 | 115 | 32 | |||||||||||||
| ALT (U/L) (0-40) | 21.2 | 24.7 | 15 | 7.7 | 18 | |||||||||||
| rGT (U/L) (11-43) | 30 | |||||||||||||||
| Alkphos (U/L) (40-106) | 96 | 94 | 121 | 122 | 111 | |||||||||||
| LDH (U/L) (135-225) | 677 | 301 | 303 | |||||||||||||
| Total protein (gm/L) (62-80) | 51.8 | 55 | ||||||||||||||
| Albumin (gm/L) (38-54) | 23.5 | 21.3 |
USG -mild hepatosplenomegaly, kidneys. Echo – normal, CT head - normal.





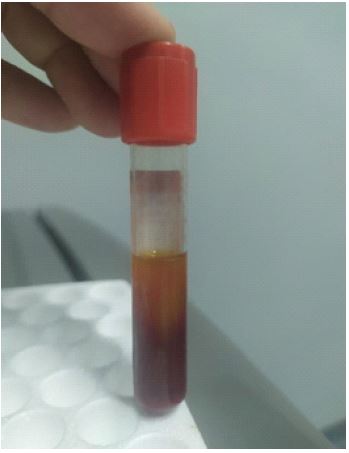

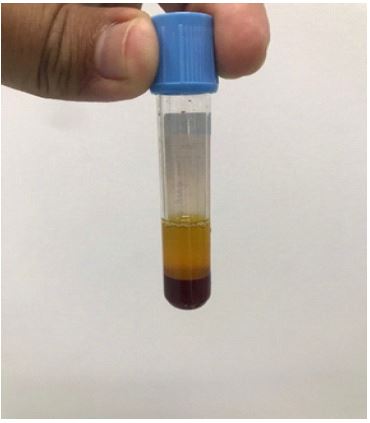





Inspection of clotted blood in clear test tube was very informative in this patient particularly in correlation with urine color; it was very useful in low resource setting. Having low red cell column indicated degree of anemia; brownish plasma revealed presence of hemolyzed RBC; daily inspection signified clinical improvement; improvement in RBC column showed improvement in anemia; less brownish color of plasma revealed less intravascular hemolysis. In addition, yellowish color at the top demonstrated increased bilirubin in serum. Combination of clinical changes, urine color and amount and serial inspection of clotted blood specimen in bed side gave excellent remarks. It is extremely useful in remote areas where malaria is endemic. This is the important reason for sharing bed side examination.
Having parasitological relapse in Day 14 after ACT (Dihydroartemisinine-piperaquine) was alarming although parasite count was not high. Containment of artemisinine resistance was done in 2014 with many challenges [3]. The recommendation from this case is “to contain ACT resistance”. He made good response to different ACT (Artemether-lumefantrine) till Day 42. It is very good news because Artemether-lumefantrine combination therapy has been introduced in Myanmar over 10 years.
Conclusion
Importance of asking travel history in medicine is highlighted. Awareness of diagnosis of malaria is important particularly to those coming back from malaria endemic areas. Recognition of severe features of falciparum malaria and timely treatment can save lives. ACT resistance in Myanmar-India border area is alarming; it may be iceberg phenomenon.
Declarations
Acknowledgements: The authors would like to thank the patient for giving consent to this article. Also, to all doctors and nursing team for making great efforts in caring him. The authors acknowledged Professor Tin Moe Mya for laboratory support, Professor Thet Naing, Professor Myint Zaw, Professor Kyaw Zay Ya and Professor Ko Ko Lwin for administrative support.
Declaration of conflict of interest: The authors declared no potential conflicts of interests with respect to authorship and publication of this article.
Ethical approval: Our institution does not require ethical approval for reporting cases.
Funding: The authors received no financial support for publication of this article.
Informed consent: The informed consent for publication in this article was obtained from patient.
References
- Liwang Cui, Yaming Cao, Jaranit Kaewkungwal, Amnat Khamsiriwatchara, Saranath Lawpoolsri, et al Malaria Elimination in the Greater Mekong Subregion: Challenges and Prospects. In Sylvie Manguin & Vas Dev (Eds.), Towards Malaria Elimination (p. Ch. 8). Intech Open. 2018; https://doi.org/10.5772/intechopen.76337
- World Health Organization. Countries of the Greater Mekong are stepping up to end malaria. World Health Organization; JSTOR. http://www.jstor.org/stable/resrep28212. 2018;
- Kyaw T, Hlaing T, Thimasarn K, Mon K, Galappaththy G, et al. Containing artemisinin resistance of Plasmodium falciparum in Myanmar: Achievements, challenges and the way forward. WHO South-East Asia Journal of Public Health. 2014; 3: 90–94. https://doi.org/10.4103/2224-3151.206893
- Ben Abderrahim S, Gharsallaoui S, Ben Daly A, Mosbahi A, Chaieb S, et al. Imported malaria in adults: About a case of cerebral malaria. Egyptian Journal of Forensic Sciences. 2022; 12: 19. https://doi.org/10.1186/s41935-022-00279-1
- Wassmer SC, Taylor TE, Rathod PK, Mishra SK, Mohanty S, et al. Investigating the Pathogenesis of Severe Malaria: A Multidisciplinary and Cross-Geographical Approach. The American Journal of Tropical Medicine and Hygiene. 2015; 93: 42–56. https://doi.org/10.4269/ajtmh.14-0841
- Schiess N, Villabona-Rueda A, Cottier KE, Huether K, Chipeta J, et al. Pathophysiology and neurologic sequelae of cerebral malaria. Malaria Journal. 2020; 19: 266. https://doi.org/10.1186/s12936-020-03336-z
- Trivedi S, Chakravarty A. Neurological Complications of Malaria. Current Neurology and Neuroscience Reports, 2022; 22: 499–513. https://doi.org/10.1007/s11910-022-01214-6
- Looareesuwan S, Laothamatas J, Brown TR, Brittenham GM. Cerebral Malaria: A New Way Forward with Magnetic Resonance Imaging (MRI). The American Journal of Tropical Medicine and Hygiene Am J Trop Med Hyg. 2009; 81: 545–547. https://doi.org/10.4269/ajtmh.2009.07-0411
- Sahu PK, Duffy FJ, Dankwa S, Vishnyakova M, Majhi M, et al. Determinants of brain swelling in pediatric and adult cerebral malaria. JCI Insight. 2022; 6. https://doi.org/10.1172/jci.insight.145823
- Opoka RO, Waiswa A, Harriet N, John CC, Tumwine JK, et al. Blackwater Fever in Ugandan Children With Severe Anemia is Associated With Poor Postdischarge Outcomes: A Prospective Cohort Study. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2020; 70: 2247–2254. https://doi.org/10.1093/cid/ciz648
- Brunee F, Gachot B, Wolff M, Régnier B, Danis M, et al. Resurgence of Blackwater Fever in Long-Term European Expatriates in Africa: Report of 21 Cases and Review. Clinical Infectious Diseases. 2001; 32: 1133–1140. https://doi.org/10.1086/319743
- Raymond S, Sitompul ARH. Successful Oral Antimalarial Therapy in A 14-Year-Old Child with Blackwater Fever: A Case in a Rural Area of Asmat Regency of Papua, Indonesia: Successful Oral Antimalarial in Blackwater Fever. IJID Regions. 2022; 3: 157–159. https://doi.org/10.1016/j.ijregi.2022.03.021
- Ujiie M, Kato Y, Takeshita N, Kanagawa S, Ohmagar N, et al. A Case of Blackwater Fever after Treatment for Plasmodium falciparum Malaria]. Kansenshogaku Zasshi. 2016; 90: 657–660.
- Yang SI, Choe YJ, Lee HJ, Choi EH. Blackwater Fever Followed by Severe Falciparum Malaria in a Child. Piv. 2017; 24: 117–122. https://doi.org/10.14776/piv.2017.24.2.117
- Huggan PJ, Ng CH, Ho J, Lin R, TP V. A case of blackwater fever with persistent Plasmodium falciparum parasitaemia detected by PCR after artemether–lumefantrine treatment. Malaria Journal. 2018; 17: 35. https://doi.org/10.1186/s12936-018-2180-1
- Newton PN, Stepniewska K, Dondorp A, Silamut K, Chierakul W, et al. Prognostic indicators in adults hospitalized with falciparum malaria in Western Thailand. Malaria Journal. https://doi.org/10.1186/1475-2013; 2875-12-229.
- Von Seidlein L, Peto TJ, Tripura R, Pell C, Yeung S, et al. Novel Approaches to Control Malaria in Forested Areas of Southeast Asia. Trends in Parasitology. 2019; 35: 388–398. https://doi.org/10.1016/j.pt.2019.03.011