
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
How team work makes the dream work: Successful management of internal carotid artery lesion during routine Functional Endoscopic Sinus Surgery (FESS)
Olga L Quintero1*; María Claudia Niño1; Juan Andrés Mejía2; Martin Pinzón3
1Anesthesiology Department, Universitary Hospital Universitario Fundación Santa Fe de Bogotá; Bogotá, Colombia.
2Department of Radiology, Division of Interventional Neuroradiology, Hospital Universitario Fundación Santa Fe de Bogotá; Bogotá, Colombia.
3Department of Otorhinolaryngology, Hospital Universitario Fundación Santa Fe de Bogotá; Bogotá, Colombia.
*Corresponding Author : Olga L Quintero
Anesthesiology Department, Universitary Hospital Universitario Fundación Santa Fe de Bogotá, Bogotá, Colombia.
Email: olquinterol@gmail.com
Received : May 03, 2023
Accepted : Jun 19, 2023
Published : Jun 26, 2023
Archived : www.jcimcr.org
Copyright : © Quintero OL (2023).
Abstract
We present the case of a 60-year-old male patient with a history of chronic rhinosinusitis with nasal polyps grade III who suffered an injury to the Internal Carotid Artery (ICA) during a scheduled Functional Endoscopic Sinus Surgery (FESS). After careful analysis of the case, all parties involved decided that an arterial reconstruction strategy with placement of a flow diverter stenting was the best approach for the patient. Finally, an optimal outcome was attained for the patient. Despite its rare occurrence in daily practice, ICA injury is a catastrophic complication once it occurs. In our case, we were able to efficiently articulate good and respectful communication amongst a highly trained group of expert care givers in order to serenely but swiftly take action and contain the complication.
Keywords: Internal carotid artery; Carotid injury; Intraoperative complications; Otorhinolaryngologic surgical procedures; Surgical outcomes; Sinus surgery; Vascular injury; Endovascular procedures.
Abbreviations: NPS: Nasal Polyps Score; FESS: Functional Endoscopic Sinus Surgery; PT: Prothrombin Time; PTT: Partial Thromboplastin Time; INR: International Normalized Ratio; OR: Operating Room; MAP Mean Arterial Pressure; ICA: Internal Carotid Artery; Angio: Angiography; CBCT Cone Bean Computerized Tomography; DSA: Digital Subtraction Angiography; ICU Intensive Care Unit.
Citation: Quintero OL, Niño MC, Mejía JA, Pinzón M. How team work makes the dream work: Successful management of internal carotid artery lesion during routine Functional Endoscopic Sinus Surgery (FESS). J Clin Images Med Case Rep. 2023; 4(6): 2472.
Introduction
Over the last three decades, the endoscopic approach to the paranasal sinuses has become a common and popular surgical practice and it is largely a safe procedure, but serious complications can occur [1,2]. Injury to the ICA is a very rare complication, however, once it occurs it has the potential to be catastrophic for the patient and a real challenge for the surgical team. Our patient recovered without neurological sequelae after a multidisciplinary and well-coordinated decision to treat the injury via an endovascular procedure. We believe the factor that was pivotal for our success was our ability to work as a well engrained team. Therefore, we present our case as an opportunity to highlight the importance of team work and expertise in catastrophic scenarios such as this.
Case description
We present the case of a 60-year-old male patient with a history of chronic rhinosinusitis with nasal polyps grade III according to the Nasal Polyps Score (NPS) who presented to our University Hospital for a scheduled Functional Endoscopic Sinus Surgery (FESS). On physical examination, the patient was 68 kg and 1.75 m tall, healthy and in good general conditions for the surgery and preanesthetic assessment did not show any relevant abnormalities for the procedure. Ambulatory laboratory test results showed a preoperative hemoglobin level of 16 mg/dl, hematocrit of 47,8%, platelets count of 355.000, Prothrombin Time (PT) of 11.5 and partial thromboplastin time (PTT) of 28,5 and an International Normalized Ratio (INR) of 0.97 and creatinine levels were within normal range for a male adult (1.09 mg/dl). The anesthetic plan included: general balanced anesthesia with orotracheal intubation, a peripheral venous access and standard non-invasive monitoring of vital signs.
On arriving to the Operating Room (OR), monitoring of blood pressure every 3 minutes, continuous pulse oximetry and 5 electrode electrocardiographic monitoring, and continual end-tidal carbon dioxide analysis using capnography was applied. Anesthetic intravenous induction was achieved using midazolam, propofol and a continuous infusion of remifentanil. Succinylcholine was used for neuromuscular blockade before laryngoscopy after induction of anesthesia. Inhaled sevorane and remifentanil were used for anesthetic maintenance.
During right sphenoidectomy of the FESS, bleeding of arterial appearance occurred (approximately 1500 ml of blood in the suction canister in less than 3 minutes) with an abrupt drop of arterial blood pressure (Mean Arterial Pressure MAP dropped from 75 mmHg to 39 mmHg). Hemostasis was performed by otorhinolaryngologist surgeon with Floseal Hemostatic Matrix + thrombin, Surgicel™ Fibrillar™ Absorbable Hemostat and cottonoids damped in an adrenaline mix until transient control of the bleeding was attained. While the surgical team aimed to control the bleeding, the anesthesiologist started resuscitation with a bolus of 1500 ml of crystalloids (lactate ringer solution) plus 500 ml of 5% albumin, 1 gram of tranexamic acid and peripheral vasopressors (bolus of 4 micrograms of noradrenaline and 1 mg of etilefrine per necessity) in order to maintain a mean pressure above 70 mmHg. Aninjury of right ICA was considered asthe most likely diagnosis given the hemodynamic changes and anatomic location of the bleeding point.
Simultaneously, another peripheral access was obtained and, the blood bank was called to crossmatch 2 units of packed red blood cells, and a venous blood gases test was taken in order to evaluate hemoglobin level, which showed a decrease in hemoglobin from 16 mg/dl to 13 mg/dl. Meanwhile, both the on-call neurosurgeon and neurointerventional radiology team were called to the operating room in order to plan a multidisciplinary approach of the situation. At this point patient was hemodynamically stable without the need of a continuous infusion of vasopressors and without further measures. The anesthesiologist decided to initiate monitoring of depth of anesthesia with a bispectral index monitor (target score between 40 and 60) and change anesthetic maintenance from balanced anesthesia to total intravenous anesthesia with target-controlled infusions of propofol (Eleveld+opioid model) and remifentanil (Minto model), and to provide deep neuromuscular blockade with rocuronium in order to ensure patient immobility. After fifteen minutes of the detection and intraoperative initial management of the complication, a multidisciplinary decision was made to transfer patient to the angiography (Angio) suite in order to perform a diagnostic cerebral angiography and minimally invasive definitive management of the possible vascular lesion.
Once the patient was securely transferred, invasive monitoring of arterial blood pressure was obtained by the anesthesiologist. Arterial blood gas test showed after crystalloid resuscitation a further decrease in hemoglobin to 9.7 mg/dl, but without further signs of continued bleeding or hemodynamical instability, therefore no blood transfusion was initiated in the moment.
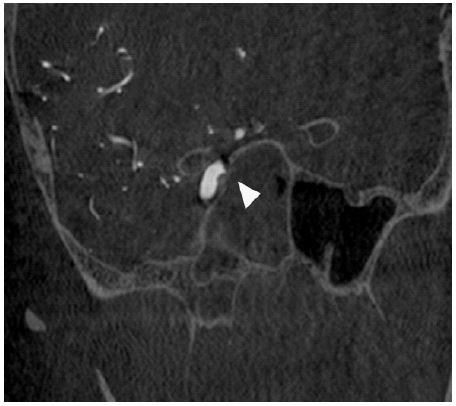
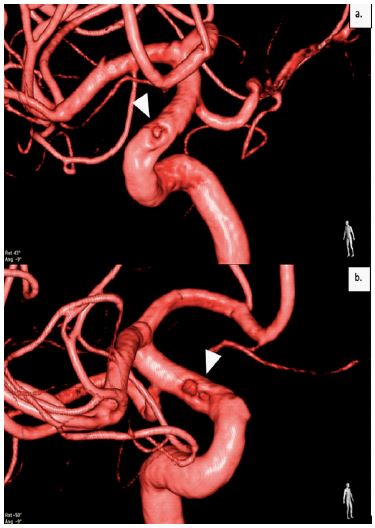
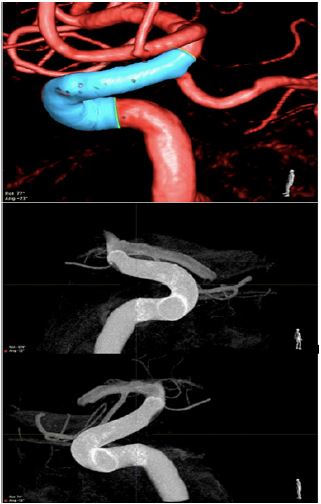
Approximately 45 minutes since the bleeding complication occurred, the patient was in the Angio suite ready and prepared for aCone Bean Computerized Tomography (CBCT), where no intraparenchymal or subarachnoid hemorrhage were detected; neither acute nor subacute ischemic lesions were seen in the right cerebral hemisphere (Figure 1). After CBCT, a right groin puncture was performed for 8-Fr sheath placement. Complete intra and extracranial Digital Subtraction Angiography (DSA) was performed to study the patency and efficiency of the Circle of Willis, which was found to be complete and functional in case arterial carotid sacrifice was needed. However, DSA and tridimensional rotational studies, showed several filling defects on the internal and lateral wall of the carotid lumen on the supraclinoid portion of the right ICA (Figures 2 and 3), attributable to hemostatic material used during the bleeding control held in the operating room. No contrast extravasation, pseudoaneurysm formations, or vasospasm were detected.

any neurological or cognitive deficit associated with the internal carotid lesion. Four hours in the ICU the patient reported an episode of right amaurosis fugax which was successfully treated with MAP augmentation with norepinephrine (target MAP 90 to 95 mmHg) after a Computed tomography angiography discarded a stroke or any complication related to the flow diverting stent as the cause of the episode. No new events were reported after. Dual antiplatelet therapy with a 300 mg loading dose of Clopidogrel and 300 mg of Aspirin was initiated prior to suspension of tirofiban.
Four days after admission to the ICU the patient nasal packing was removed and the patient was discharged home with dual antiplatelet oral therapy, without any neurological symptoms nor deficits.
Discussion
Over the last three decades, the endoscopic approach to the paranasal sinuses has become a common and popular surgical practice and it is largely a safe procedure, but serious complications can occur [1,2]. According to a systematic review by Dalziel, K. et al, overall complications for FESS from case series studies ranged from 0.3 to 22.4% (median, 7.0%), and injury to the ICA, being among the potentially most serious complications reported, could occurr in 0.3% of patients [3,4]. However, most studies have reported an incidence of ICA during FESS below 0.1% [1,2]. Despite its rare occurrence in daily practice, it is safe to say that ICA injury is one of the most feared and terrifying situations faced by otolaryngologists, skull base surgeons and anesthesiologists for its potential to render severe neurological sequelae or even a mortal outcome for the patient [1]. Multidisciplinary teams working together, comprehensive preoperative imaging, patient risk assessment, and formal training in vascular emergencies may reduce the risk of adverse outcomes in case this devastating complication occurs [2,5].
Effective communication in the OR refers to the process by which all parties involved understand what is being conveyed and it includes all forms of interaction that are required for complete understanding of everyone involved: verbal, para-verbal (e.g., tone, speed), and non-verbal elements (e.g., body language, eye contact) [5]. Nevertheless, at times where it is most relevant and needed, the process of communicationin the OR can be seriously hindered by barriers such as perceived hierarchies and environmental factors (e.g., stressful situations, multiple senders/receptors of information interacting at the same time, unexpected complications). Precise and unambiguous communication is difficult to accomplish, yet it is the cornerstone of effective teamwork and it is a skill that must be intentionally developed by groups working together [5]. As Etherington et al. explains in their narrative review, high-reliability OR teamwork requires mutual performance monitoring, team leadership, backup behavior, adaptability, team orientation, mutual trust, and shared mental models (or common understanding of the situation among team members) [5].
In our case, we were able to efficiently articulate good and respectful communication amongst a highly trained group of care givers in order to serenely but swiftly take action and contain the complication. All team members shared information and established a common understanding of the situation, treatment plan, and individual roles without letting barriers interfere. This, in our opinion, made the difference and yielded a great outcome for our patient. Once the bleeding presented, the anesthesiologist communicated clearly to the surgeon that hemodynamically instability had ensued and that given the rapidity and volume of blood loss, an injury to the ICA was possibly the culprit. This prompted a hastyresponse from the surgeon to call for help (neurosurgery and neurointerventional radiology) meanwhile doing effective hemostasis of the bleeding vessel. The OR chief nurse and the rest of the staff was also made aware of the severity of the complication, and proceeded to rapidly provide all the support and care needed. The interventional radiology team also provided a rapid support response and were ready to receive the patient as soon as it was prudent to transfer him to the Angio suite (located across the hall from the OR in our hospital).
There are several considerations in the endovascular management of ICA injuries under endoscopic endonasal surgery. Some of the most important concerns before transferring the patient to the Angio suite are obtaining hemostasis, hemodynamic stability and assessing if intracranial bleeding has occurred (most frequently subarachnoid hemorrhage) [6]. Regarding hemostasis and hemodynamic stability, deliberate hypotension has been previously used in order to improve visibility of the surgical field and reduce de blood loss [2], none the less maintaining normotension to provide contralateral cerebral perfusion and prevent ischemic neurologic sequelae might be more important for favorable outcomes which in the case of our patient was successfully done. According to best practice literature, after temporary hemostatic control is attained, all patients with no exception should be immediately transferred to the Angio suiteto effectively characterize the extent of the carotid injury [6].
Concerning the endovascular treatment of ICA injuries, it basically involves three strategies which include deconstructive therapy through arterial sacrifice, arterial dissection or pseudoaneurysm embolization, and endoluminal reconstruction [7]. Often, the treatment planning must be held immediately according to the correlating imaging features and hemodynamic status of the patient [7]. In our case, given the characteristics of the injury, a vessel preservation technique was considered and turned to be the best option. The decision of how to approach the ICA damage should always be judiciously pondered for each patient. Multiple factors including vascular anatomy, injury characteristics, and risk of dual antiplatelet therapy should guide best treatment, but as many other areas of the practice of medicine, more research is needed to refine the decision making [7]. Nonetheless, it is clear from our perspective and from the available literature that ideally all endovascular treatment options and an experienced group of providers should be available at institutions performing endonasal surgery [6-8].
Even though great advances have been made in technology, resources and training, the rate of complications experienced by surgical patients remains high with nearly one in ten suffering from one at some point of their medical care [5]. How the team of caregivers handle these complications is critical since any error might potentially result in severe consequences such as increased length of hospital stay, morbidity, mortality, and financial costs to the healthcare system [5,9]. Therefore, good communication skills, teamwork in the operating room, flat hierarchies, and an institutional culture that encourages individuals to speak up and express concerns without retaliation, are all invaluable for patient outcomes, especially when complications arise as it directly impacts incident recovery [5].
Declarations
Acknowledgements: We would like to thank everyone who contributed to the study: The specialist reviewers and the researcher assistant of the Department of anesthesia for the co-ordination of the data collection.
Competing interests: The authors declare that they have no competing interests.
References
- R Valentine, PJ Wormald, Carotid Artery Injury After Endonasal Surgery, Otolaryngol. Clin. North Am. 2011; 44: 1059–1079.
- RK Sharma, AL Irace, JB. Overdevest, DA Gudis, Carotid artery injury in endoscopic endonasal surgery: Risk factors, prevention, and management, World J. Otorhinolaryngol. - Head Neck Surg. 2022; 8: 54–60.
- K Dalziel, K Stein, A Round, R Garside, P Royle, et al. Endoscopic sinus surgery for the excision of nasal polyps: A systematic review of safety and effectiveness, Am J Rhinol. 2006; 20: 506–519.
- R Weber, W Draf, R Keerl, B Schick, A Saha, et al. Endonasal microendoscopic pansinusoperation in chronic sinusitis II. Results and complications, Am. J. Otolaryngol. - Head Neck Med. Surg. 1997; 18: 247–253.
- N Etherington, M Wu, O Cheng-Boivin, S Larrigan, S Boet, et al. Interprofessional communication in the operating room: A narrative review to advance research and practice, Can. J. Anesth. 2019; 66: 1251–1260.
- ZM Kassir, PA Gardner, EW Wang, GA Zenonos, CH Snyderman, et al. Identifying Best Practices for Managing Internal Carotid Artery Injury During Endoscopic Endonasal Surgery by Consensus of Expert Opinion, Am. J. Rhinol. Allergy. 2021; 35: 885–894.
- PT Sylvester, CJ Moran, CP Derdeyn, DT Cross, RG Dacey, et al., Endovascular management of internal carotid artery injuries secondary to endonasal surgery: Case series and review of the literature, J. Neurosurg. 2016; 125: 1256–1276.
- G Kahilogullari, B Bahadır, M Bozkurt, S Akcalar, S Balci, et al. Carotid Artery-Cavernous Segment Injury during an Endoscopic Endonasal Surgery: A Case Report and Literature Review of the Overlooked Option for Surgical Trapping in the Hyperacute Phase, J. Neurol. Surg. Reports. 2021; 82: e53–e62.
- M Zegers, MC de Bruijne, B de Keizer, H Merten, PP Groenewegen, et al., The incidence, root-causes, and outcomes of adverse events in surgical units: Implication for potential prevention strategies, Patient Saf. Surg. 2011; 5: 13.