
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Role of superior mesenteric artery doppler and maternal pancreatic size for prediction of gestational diabetes mellitus
Gupta A; Khanduri S; Surbhi; Pathak V*; Dwari K; Siddiqui SA; Fatima A; Bansal T
Radiodiagnosis, Era’s Lucknow Medical College, Lucknow, India.
*Corresponding Author : Vaibhav Pathak, MD
Radiodiagnosis, Era’s Lucknow Medical College, Lucknow, India.
Tel: +91-980-891-7393
Email: vaibhawfbd@gmail.com
Received : May 02, 2023
Accepted : Jun 21, 2023
Published : Jun 28, 2023
Archived : www.jcimcr.org
Copyright : © Pathak V (2023).
Abstract
Background: Gestational Diabetes (GDM) is a glucose tolerance disorder that occurs or is diagnosed during pregnancy with no prior history of the disorder [1,2]. Contemporary studies have reported that GDM affects 1%-14% of all pregnancies, and the incidence has been steadily rising [3]. The mechanism of GDM is defined as insufficient/dysfunction of β-cell, which regulate the diabetogenic conditions by overcoming the antagonism created by the anti-insulin hormone of pregnancy [4].
Aim: To study the role of superior mesenteric artery doppler and maternal pancreatic size for prediction of gestational diabetes mellitus.
Objectives: 1. to measure maternal superior mesenteric artery Doppler indices and maternal pancreatic size. 2. To determine gestational diabetes mellitus by maternal superior mesenteric artery Doppler indices and maternal pancreatic size.
Methods: The research was performed on (82) antenatal subjects coming for routine anomaly scan between 18 weeks to 22 weeks of gestation.
Maternal pancreatic body size and doppler indices of maternal superior mesenteric artery was taken using transabdominal probe with mean 3.5 MHz broadband (GE LOGIQ P9 AND SAMSUNG HS70). Then the Oral Glucose Tolerance Test (OGTT) was performed on follow – up visits between 24 and 28 weeks. Subjects were divided into gestational Diabetes Mellitus (GDM) categories on the basis of OGTT performed then the pancreatic body size and doppler indices taken during 18–22 weeks were compared between GDM and non-GDM subjects to predict the development of gestational diabetes mellitus.
Results: This is a prospective study; all 82 subjects were selected from the patients visiting the opd for routine ANC visit between 18 weeks to 22 weeks for singleton pregnancy. In our study, we observed that there is coherence between Doppler indices of the superior mesenteric artery and maternal pancreatic size predicting the development of gestational diabetes mellitus. Out of 82 subjects, 53 came out to be positive for gestational diabetes mellitus.
Conclusion: In this study, we concluded that mesenteric artery Doppler and pancreatic size can be used as a tool for predicting the development of gestational diabetes mellitus.
Keywords: Gestational diabetes mellitus; Superior mesenteric artery; Transvaginal ultrasound; Doppler.
Abbreviations: GDM: Gestational Diabetes Mellitus; SMA: Superior Mesenteric Artery; DM: Diabetes Mellitus: GDM: Gestational Diabetes Mellitus.
Citation: Gupta A, Khanduri S, Surbhi, Pathak V, Dwari K, et al. Role of superior mesenteric artery doppler and maternal pancreatic size for prediction of gestational diabetes mellitus. J Clin Images Med Case Rep. 2023; 4(6): 2476.
Introduction
Some of the maternal complications associated with GDM include: (i) excessive weight gain (ii) miscarriage (iii) poly-hydramnios (iv) preeclampsia (v) preterm labour (vi) Premature Rupture of Membrane (PROM) and increased incidence of caesarean section i.e. operative interference while foetal complications include: (a) congenital malformation (b) macrosomia (c) birth trauma (d) shoulder dystocia and new born will have increased incidence of hypoglycaemia, hypocalcaemia, hyper bilirubinaemia, Respiratory Distress Syndrome (RDS) and polycythemia [5-8].
One must understand that timely action taken in screening all pregnant women for glucose intolerance, achieving euglycemia in them and ensuring adequate nutrition may prevent in all probability, the vicious cycle of transmitting glucose intolerance from one generation to another [9].
As diabetes finds its origin at either dysfunctioning of pancreas resulting in insufficient insulin secretion and/or improper absorption of sugar from blood. Contemporary studies have provided with sufficient evidence regarding the role of Superior Mesenteric Artery (SMA) blood flow and increased nutrient absorption in the small intestine [10-12]. Since the findings and physiological relationships between SMA, pancreas and diabetes have been reported there has been an additional attempt at better understanding the relationship between SMA and pancreas with gestational diabetes. In a similar attempt, the present study was conducted with the aim to study the role of pancreatic size and superior mesenteric artery in Gestational diabetes.
Materials and methods
The study was carried out at the Department of Radiodiagnosis in collaboration with the Department of Medicine in Era’s Lucknow Medical College & Hospital, Lucknow. Clearance for carrying out the study was obtained from the Institutional Ethical Committee Era’s Medical College (Approval number: ELMC & H /RCELL, EC/2021/132), and informed consent was obtained from all the patients. Inclusion criteria includes antenatal women with period of gestation 18-22 weeks and singleton pregnancy. Whereas exclusion criteria include pre-pregnancy Diabetic patients, Multifetal pregnancies, Hypertensive patients and BMI more than 30 kg/m2. All subjects underwent maternal superior mesenteric artery Doppler and pancreatic body size measurement after foetal anomaly screening. Between 24 and 28 weeks of gestation routine oral glucose tolerance test was ordered for each participant. Subjects were divided into two groups as patients with gestational diabetes and normal pregnancies. Relationship between Doppler and pancreatic measurements with GDM was analysed.
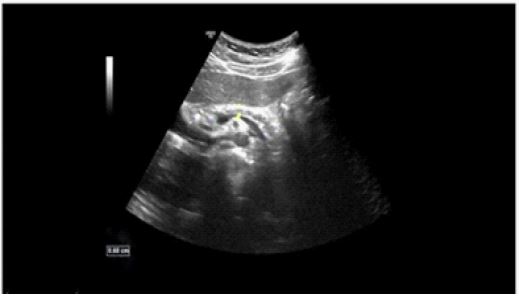
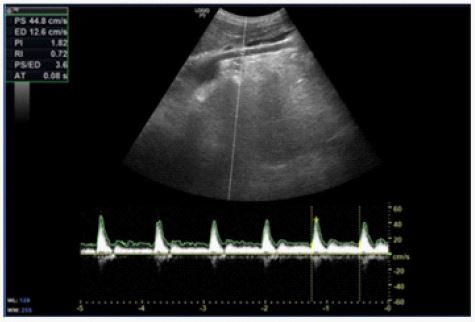
All subjects scanned in supine position after 8 h fast. Grayscale and Doppler US studies were performed in convex-array transabdominal probe with mean 3.5 MHz broad band (GE LOGIQ P9 AND ‘Samsung HS 70A, Samsung Medison, Korea) by two clinical radiologist who was unaware which subjects had GDM. We measured the anteroposterior diameter of pancreatic body on transverse images respectively. SMA was evaluated along the sagittal plane long axis. After the demonstration of SMA on gray scale examination, we applied colour flow mapping window and spectral analysis. The sampling pointer was placed at 2-3 cm distal component from the origin of the branch in real time imaging. The sampling was applied inside of the lumen. The Doppler signal was optimized with adjustment of probe position and gain measurements. The Doppler angle was kept below 60 to the long axis of SMA and the width of sampling gate was 3 mm. The pulse repetition frequency was 1.3 kHz and aliasing artefacts were excluded. Continuous wave trace was used to evaluate the waveform of the vessel [13]. We obtained the proper signal after five similar consecutive waveforms during one breath-hold. After the peak-systolic and end-diastolic (S/D) flow velocities measurement, we also obtained Resistance Index (RI) ratios in all subjects. Resistance index (RI), is a ratio of blood flow pulsatility measurement and reflects the resistance to the blood flow caused by distal component of the measurement site. RI ratio is determined by peak systolic velocity––end diastolic velocity/peak systolic velocity [14].
Diagnosis of GDM between 24 and 28 weeks of gestation routine, 50 g glucose challenge test was ordered for each participant. Plasma glucose concentration is measured after 1 h. Cut off value of glucose challenge test was accepted to be 140 mg/dl. The participants with test result higher than 140 mg/dl were referred to 3 h of 100 g glucose administration for assessment of glucose tolerance status in pregnancy. The diagnostic criteria accepted by American Diabetes Association were 2 or more abnormal values during a standard 100 g OGTT. Normal glucose values were <95, <180, <155, <140 at 0, 1, 2 and 3 h respectively [15]. Subjects with a screening result higher than 180 mg/dl coupled with wasting glucose level higher than 95 mg/dl were not referred to OGTT and accepted to be GDM.
Statistical analysis: Sample size at 90% Power of Study.
Sample size is calculated on the basis of proportion of cases with S/D less than 4.04 using the formula.
Where p1 = 0.266 (26.6%) proportion of cases with S/D less than 4.04 in normal. p2 = 0.786 (94.4%) proportion of cases with S/D less than 4.04 in cases (Ref. Tosun et. al.). Risk difference e = (p2- p1) considered to be clinically significant Type I error, α=5% (level of significance) Type II error β=10% for setting power of study 90% Data loss factor = 10% the sample size was calculated to be n=82.
Results
For this study, 82 pregnant women attending ANC at Dept. of Obstetrics and Gynaecology, ELMC&H and referred to Dept. of Radiodiagnosis, ELMC&H were screened for the inclusion and exclusion criteria and enrolled in the study. Table 1 below shows the Age wise distribution of the study population:
Table 1: Age wise distribution of the study population (N=82)
| SN | Age Group | Frequency | Percentage |
|---|---|---|---|
| 1 | ≤20 years | 6 | 7.3 |
| 2 | 21-30 years | 52 | 63.4 |
| 3 | 31-40 years | 22 | 26.8 |
| 4 | ≥41 years | 2 | 2.4 |
| Mean Age in years ± SD (Range) | 28.11 ± 5.81 (18.0-49.0) years | ||
Majority of the women were aged between 21 & 30 years (63.4%), followed by 31-40 years (26.8%), ≤20 years (7.3%) and ≥41 years (2.4%). The mean age of the women was 28.11 ± 5.81 years.
Table 2: Distribution of the study population according to Maternal Anthropometric Parameters
| SN | Maternal Parameters | |
|---|---|---|
| 1 | Mean Weight in kgs ± SD (Range) | 61.73 ± 6.12 (49-84) |
| 2 | Mean Height in cms ± SD (Range) | 158.35 ± 4.00 (148.30-166.73 |
| 3 | Mean BMI in kg/m2 ± SD (Range) | 24.58 ± 1.49 (22.0-30.8) |
Maternal Weight ranged between 49 & 84 kgs. The Maternal Weight was 61.73 ± 6.12 kgs. Maternal Height ranged between 148.30 & 166.73 cms. The mean Maternal Height was 158.35 ± 4.00 cms. Maternal BMI ranged between 22 & 30.85 kg/m2. The mean BMI was 24.58 ± 1.49 kg/m2
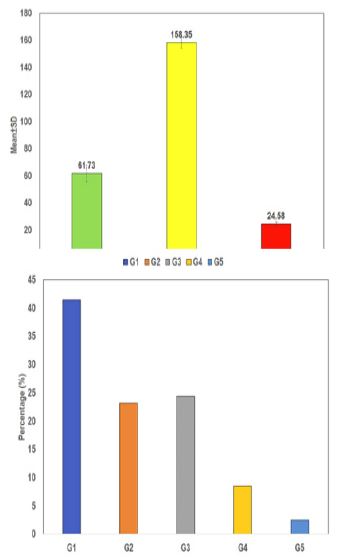
With respect to Gravida status, most of the women were G1 (41.5%), followed by G3 (24.4%), G2 (23.2%), G4 (8.5%) and G5(2.5%).
Table 3: Distribution of the study population according to Imaging Characteristics
| SN | Imaging characteristis | |
|---|---|---|
| 1 | Mean SMSAD ratio ± SD | 3.88 ± 0.44 (2.8-4.7) |
| 2 | Mean SMARI ± SD | 0.70 ± 0.04 (0.58-0.76) |
| 3 | Mean Pancreatic Size ± SD | 16.35 ± 1.71 (9.2-19.0) |
Maternal Mesenteric Artery Ratio (SMASD) ranged between 2.8 & 4.7 kgs. The mean SMASD was 3.88 ± 0.44. Maternal SMARI ranged between 0.58 & 0.76 units. The mean Maternal Height was 0.70 ± 0.04 units. Maternal Pancreatic Size ranged between 9.2 & 19.0 units. The mean Pancreatic size was 16.35 ± 1.71 kg/m2.
Table 4: Distribution of the study population according to GDM status
| SN | GDM Status | Frequency | Percentage |
|---|---|---|---|
| 1 | Negative | 53 | 64.6 |
| 2 | Positive | 29 | 35.4 |
Table 5: Association of GDM status with imaging parameters
| SN | GDM Negative | GDM Positive | Student’s t-test | ||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | T | p | ||
| 1 | SMASD Ratio | 4.09 | 0.33 | 3.50 | 0.34 | 7.542 | <0.001 |
| 2 | SMARI | 0.72 | 0.02 | 0.66 | 0.03 | 8.690 | <0.001 |
| 3 | Pancreatic Size | 17.26 | 0.87 | 14.70 | 1.63 | 9.310 | <0.001 |
On comparing statistically, GDM negative women as compared to GDM positive had significantly higher SAMASD ratio (4.09±0.33 vs. 3.54±0.32), SMARI (0.72±0.02 vs. 0.66±0.04) and Pancreatic size (17.31±0.78 vs. 14.70±1.63).
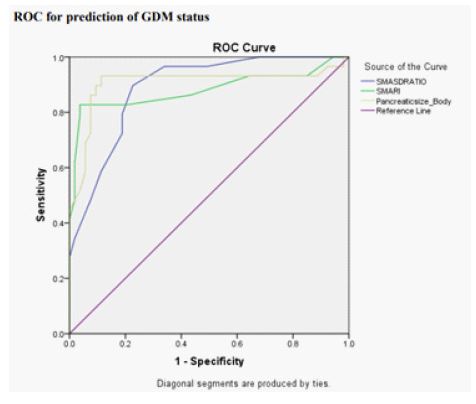
Table 6:
| SN | Variable | Cut off | Sensitivity | Specificity |
|---|---|---|---|---|
| 1 | SMASD Ratio | <3.70 | 72.4% | 81.1% |
| 2 | SMA RI | <0.685 | 79.3% | 96.20% |
| 3 | Pancreatic Size | <16.25 | 86.2% | 90.60% |
Table 7:
| SN | Variable | AUC | 95% CI Lower Bound | 95% CI Upper Bound | ‘p’ |
|---|---|---|---|---|---|
| 1 | SMASD Ratio | 0.888 | 0.819 | 0.958 | <0.001 |
| 2 | SMA RI | 0.881 | 0.784 | 0.977 | <0.001 |
| 3 | Pancreatic Size | 0.905 | 0.815 | 0.995 | <0.001 |


Discussion
Gestational Diabetes Mellitus (GDM) is a common metabolic disorder that develops during pregnancy and affects the health of both mother and foetus. It is characterized by high blood sugar levels that usually resolve after childbirth but increases the risk of developing Type 2 Diabetes Mellitus (T2DM) later in life. GDM can lead to a range of adverse pregnancy outcomes such as macrosomia, preeclampsia, and foetal malformations. Early detection and management of GDM are important to reduce these risks. In recent years, there has been growing interest in the use of non-invasive diagnostic tools such as ultrasound to predict GDM. This review focuses on the role of pancreatic size and mesenteric artery Doppler in predicting GDM. The pancreas is a glandular organ that plays a vital role in glucose metabolism by producing insulin and glucagon. Alterations in pancreatic size and function have been implicated in the pathogenesis of GDM. Several studies have investigated the relationship between pancreatic size and GDM. Various contemporary studies have reported a strong association of pancreatic size and GDM [16,17]. The findings of these studies suggest that increased pancreatic size may be a potential marker for GDM. However, further studies are needed to confirm these results and determine the clinical usefulness of pancreatic size as a predictor of GDM. On the other hand, doppler ultrasound is a non-invasive imaging technique that measures blood flow velocity and direction in blood vessels. It has been used to evaluate the mesenteric artery, which supplies blood to the gastrointestinal tract, liver, and pancreas. Alterations in mesenteric artery blood flow have been associated with GDM [18,19]. The findings of such studies suggest that alterations in mesenteric artery blood flow may be a potential marker for GDM. However, like the studies on pancreatic size, further studies are needed to confirm these results and determine the clinical usefulness of mesenteric artery Doppler as a predictor of GDM.
In the present study, the prevalence of GDM was reported to be 35.4%. In the present study, no significant association was observed between Gravida status and GDM status. In the present study no significant association was observed between GDM status and Maternal Age. The prevalence of GDM in the present study is higher than most of the contemporary studies that estimated the prevalence of GDM in India to be around 7% to 17% depending on the region and demography [20-22], but it can be contributed to the study setting, which is a tertiary center and hence witnesses a large number of referral cases from nearby rural and smaller districts as well, and hence the higher prevalence of GDM in the study.
In the present study, mean SMA S/D ratio was 3.88±0.44. SMA S/D ratio ranged between 2.8 & 4.7. While the SMARI ranged between 0.58 & 0.76. Mean SMARI was 0.70±0.04 units. In the present study, the Pancreatic size ranged from 9.2 to 19.0 mm. Mean Pancreatic size was 16.35±1.71 mm. In the present study, a statistically significant association of lower SMA SD ration, SMARI & Pancreatic size with GDM status was reported.
The findings of the preset study with respect to findings of SMA and Pancreatic artery are similar to most of the contemporary literature that has been published using diabetic population. The findings of some of these contemporary studies suggest that there is a significant effect of diabetes, especially Type 1 diabetes on the pancreatic size and thereby providing one of the most crucial evidential support to the present study. The findings of the present study can be explained by the etiology of the two types of diabetes.
However, because the causes of GDM and Type-I diabetes are both very complex and not very well understood, the seems to be a need to clearly establish similarities between the two disorders, it is also difficult to rely on the findings of the study due to acute shortage of studies comparing SMA and Pancreatic size in women with and without-GDM and the only one by Tosun et al. (2015) 23 have presented with contradictory results.
In the present study, the Area Under the Curve, for SMA SD ratio, SMA RI and Pancreatic size were 0.888, 0.881, and 0.905 respectively. The cut-off for the SMA SD ratio was <3.750 and the sensitivity and specificity were 72.4% & 81.1% respectively. While the cut-off for SMA RI and Pancreatic size was <0.685 and <16.25 mm with sensitivity & specificity of 79.3% & 96.2% and 86.2% & 90.60% respectively.
In totality, the findings of the present study suggest that there exists a relationship suggestive of the role of pancreatic size and SMA in predicting GDM, but this relationship needs to be further evaluated in depth and studies with larger sample sizes and multi-centric models need to be taken to better understand this relationship. It is also recommended that SMA parameters and maternal pancreatic size be evaluated at ANC visits to add to evidence and predict GDM. Also, most of the studies discussed above suggest that pancreatic size and mesenteric artery Doppler may be potential markers for GDM. However, it is important to note that these findings are based on relatively small sample sizes and may not be generalizable to larger populations. Furthermore, the clinical usefulness of these markers as predictors of GDM remains uncertain.
One potential application of these markers can be for the screening of GDM. Current screening methods for GDM include a glucose challenge test followed by a glucose tolerance test. These tests are invasive and time-consuming and may not be feasible in resource-limited settings. Non-invasive markers such as pancreatic size and mesenteric artery Doppler may provide a simpler and more cost-effective screening tool for GDM.
Another potential application of these markers is in identifying women at high risk for adverse pregnancy outcomes associated with GDM. Women with GDM are at increased risk of developing macrosomia, preeclampsia, and fetal malformations. Non-invasive markers such as pancreatic size and mesenteric artery Doppler may help identify women at high risk for these complications and guide appropriate management strategies.
Limitations
Despite the potential advantages of these markers, there are several limitations that need to be considered. First, the cost and availability of imaging equipment may limit the widespread use of these markers in clinical practice. Second, the interpretation of imaging results may be subjective and depend on the experience of the operator. Finally, the clinical usefulness of these markers needs to be validated in larger, multi-centre studies before they can be recommended for routine clinical use.
In summary, pancreatic size and mesenteric artery Doppler may be potential markers for GDM. The available evidence suggests that increased pancreatic size and alterations in mesenteric artery blood flow may be associated with the development of GDM. However, further studies are needed to confirm these findings and determine the clinical usefulness of these markers as predictors of GDM. These markers may have potential applications in screening for GDM and identifying women at high risk for adverse pregnancy outcomes associated with GDM. However, their cost, availability, and interpretive subjectivity need to be considered before recommending routine clinical use.
Conclusion
The findings of the present study were:
On maternal abdominal ultrasound, mean SMA SD ratio was 3.88 ± 0.44 and ranged between 2.8 & 4.7. While, mean SMA RI was 0.70 ± 0.04 and ranged between 0.58 & 0.76. The mean pancreatic size was 16.35 ± 1.71 mm and ranged from 9.2 to 19.0 mm. Majority of the patients were GDM negative (64.6%), while the remaining were GDM positive (35.4%).No statistically significant association was for GDM status with Age or Gravida. Women who developed GDM had statistically significantly lower SMA SD ratio, SMA RI and Pancreatic size (3.50±0.34, 0.66±0.03 & 14.70 ± 1.63 mm, respectively) as compared to GDM negative patients (4.09 ± 0.33, 0.72 ± 0.02 and 17.26 ± 0.87 mm, respectively). AUC for SMA SD ratio, SMA RI and Pancreatic size was 0.888, 0.881 and 0.905 respectively. At cut-off of <3.750 for SMA SD was 72.4% for SMA SD was 72.4% <0.685 SMA RI was 79.3% sensitive and 96.2% specific, at cut-off <16.25 Pancreatic size was 86.2% sensitive and 90.6% specific for prediction of GDM.
Declarations
Conflict of interest: The author declares no conflict of interest.
Competing interests: The authors declare there are no financial conflicts of interest to disclose.
Ethical consent: Waiver for the written informed consent has been received from the ethics committee.
Informed consent: Informed consent was obtained from all individual participants included in the study.
Consent for publication: I hereby give our consent for publication.
Author contributions: Dr. Ashkrit Gupta was responsible for the conception and design, analysis and interpretation of the data, the drafting of the paper or revising it critically for intel- lectual content. The author has approved the final version of the manuscript to be published.
Data availability statement: The data that support the findings of this study are available on request from the corresponding author, Dr. Vaibhav Pathak, upon reasonable request.
References
- Kaaja RJ, Greer IA. Manifestations of chronic disease during pregnancy. JAMA. 2005; 294: 2751–2757.
- Beckmann CRB, Ling FW, Smith RP, et al, editors. Obstetrics and Gynecology. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2005.
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2007; 30: S45–S46.
- Seshiah V, Das AK, Balaji V, Joshi SR, Parikh MN, et al. Gupta S for DIPSI. Gestational Diabetes Mellitus – Guidelines. JAPI. 2006; 54: 622-628.
- Reece EA. The fetal and maternal consequences of gestational diabetes mellitus. J MaternFetal Neonatal Med. 2010; 23: 199-203.
- Odar E, Wandabwa J, Kiondo P. Maternal and fetal outcome of gestational diabetes mellitus in Mulago Hospital, Uganda. African Health Sciences. 2004; 4: 9-14.
- Farooq MU, AyazAb, Ali Bahoo Lb, Ahmad I. Maternal and Neonatal Outcomes in Gestational Diabetes Mellitus. Int J Endocrinol Metab. 2007; 3: 109-115.
- Pettitt DJ, Knowler WC, Baird HR, Bennett PH, et al. Gestational Diabetes: Infant and Maternal Complications of Pregnancy in Relation to Third Trimester Glucose Tolerance in the Pima Indians. Diabetes Care. 1980; 3: 458-464.
- Seshiah V, Balaji V, Madhuri S Balaji. Scope for Prevention of Diabetes – Focus Intrauterine milieu Interieur. JAPI. 2008; 56: 109-113.
- Sim JA, Horowitz M, Summers MJ, Trahair LG, Goud RS, et al. Mesenteric blood flow, glucose absorption and blood pressure responses to small intestinal glucose in critically ill patients older than 65 years. Intensive Care Med. 2013; 39: 258-266.
- Gentilcore D, Nair NS, Vanis L, Rayner CK, Meyer JH, et al. Comparative effects of oral and intraduodenal glucose on blood pressure, heart rate, and splanchnic blood flow in healthy older subjects. Am J Physiol RegulIntegr Comp Physiol. 2009; 297: R716-22.
- Vanis L, Gentilcore D, Hausken T, Pilichiewicz AN, Lange K, et al. Effects of gastric distension on blood pressure and superior mesenteric artery blood flow responses to intraduodenal glucose in healthy older subjects. Am J Physiol RegulIntegr Comp Physiol. 2010; 299: R960-967.
- Sigirci A, Senol M, Aydin E, et al. Doppler waveforms and blood flow parameters of the superior and inferior mesenteric arteries inpatients having Behcet disease with and without gastrointestinal symptoms: preliminary data. J Ultrasound Med. 2003; 22: 449–457.
- Tublin ME, Bude RO, Platt JF. The resistive index in renal Doppler sonography: where do we stand? AJR Am J Roentgenol. 2003; 180: 885– 892.
- American diabetes association. Gestational diabetes mellitus. Diabetes Care. 2000; 23: S77–S79.
- Kayemba-Kay’s S, Fabry C, Harnois F, et al. Pancreatic size is a marker of glucose intolerance in pregnancy. Ultrasound Obstet Gynecol. 2017; 50: 731-737.
- Cho NH, Kim KW, Roh SG, et al. Pancreatic volume and fat fraction in women with gestational diabetes mellitus. Diabetologia. 2018; 61: 1141-1148.
- Sahin HG, Aslan E, Aslan H, et al. Mesenteric artery Doppler in predicting gestational diabetes mellitus. J Obstet Gynaecol Res. 2016; 42: 269-275.
- Ciavattini A, Delli Carpini G, Di Giuseppe J, et al. Doppler velocimetry of the superior mesenteric artery in prediction of gestational diabetes mellitus. Arch Gynecol Obstet. 2019; 300: 195-202.
- Swaminathan G, Swaminathan A, Corsi DJ. Prevalence of Gestational Diabetes in India by Individual Socioeconomic, Demographic, and Clinical Factors. JAMA Netw Open. 2020; 3: e2025074.
- Seshiah V, Balaji V, Balaji MS, et al. Prevalence of gestational diabetes mellitus in South India (Tamil Nadu)--a community based study. J Assoc Physicians India. 2008; 56: 329-333.
- Wahi P, Dogra V, Jandial K, et al. Prevalence of Gestational Diabetes Mellitus (GDM) and its outcomes in Jammu region. J Assoc Physicians India. 2011; 59: 227-230.
- Tosun A, Duzguner S, Ozkaya E, Korkmaz V, A car S, et al. Utility of superior mesenteric artery Doppler and maternal pancreatic size for predicting gestational diabetes mellitus. Ir J Med Sci. 2015; 184: 499-503.