
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Rheumatoid arthritis presenting as vasculitis and neuropathy: A case report and review
Arti Muley*; Bhargav Bhaliya; Sona Mitra; Dinesh Nakum; Kuldeep
1Professor, Department of Medicine, PIMSR, Parul University, Waghodia, Vadodara, Gujarat, India.
2Assistant Professor, Department of Medicine, PIMSR, Parul University, Waghodia, Vadodara, Gujarat, India.
3Clinical Research Associate, PIMSR, Parul University, Waghodia, Vadodara, Gujarat, India.
4Senior Resident, Department of Medicine, PIMSR, Parul University, Waghodia, Vadodara, Gujarat, India.
5Resident, Department of Medicine, PIMSR, Parul University, Waghodia, Vadodara, Gujarat, India.
*Corresponding Author : Arti Muley
Professor, Department of Medicine, PIMSR, Parul University, Waghodia, Vadodara, Gujarat, India.
Email: muleyarti40@gmail.com
Received : Jun 05, 2023
Accepted : Jun 22, 2023
Published : Jun 29, 2023
Archived : www.jcimcr.org
Copyright : © Muley A (2023).
Abstract
Rheumatoid vasculitis is a rare condition that causes inflammation of small or medium sized blood vessels. It most often affects vessels of skin, fingers, toes, nerves, eyes and heart. Neuropathy is also a rare extra articular complication of rheumatoid arthritis which is associated with vasculitis in most cases. We present a long standing untreated case of rheumatoid arthritis who presented with vasculitis and neuropathy (nonvasculitic) to emphasize significance of timely diagnosis, awareness of extra articular complications, good lower extremity examination and proper in time treatment of rheumatoid arthritis.
Keywords: Rheumatoid arthritis; Vasculitis; Neuropathy.
Citation: Muley A, Bhaliya B, Mitra S, Nakum D, Kuldeep V, et al. Rheumatoid arthritis presenting as vasculitis and neuropathy: A case report and review. J Clin Images Med Case Rep. 2023; 4(6): 2478.
Case report
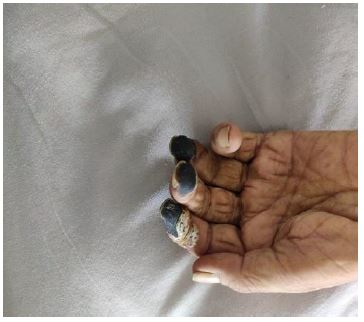
A 49-year-old male presented to our OPD with bilateral lower limb weakness, inability to bear weight and tingling sensation over both upper limbs since three to four months. He had ulcers over lower back and dorsum of both feet since two months. He also had blackening of fingers of both hands since 10-15 days.
The weakness was insidious in onset, developed simultaneously in both limbs and progressed slowly over 15 days to inability in walking. The ulcers were painless with no bleeding or discharge. The lower back ulcer was reported by his wife as the patient was unaware of it.
There was no history of rash, fever, headache, epistaxis, nasal crusting, sinusitis, deafness, cough, haemoptysis, wheeze, chest pain, dyspnoea, mouth ulcers, diarrhoea, haemorrhage abdominal pain, vision changes or trauma.
He had history of pain in multiple small joints off and on since last 10-15 years for which he used to take painkillers frequently. In the course of time he also developed deformity of fingers of both the hands, but he never approached any doctor or hospital for these complaints. Since last 4-5 months, the joint pain had increased for which he was hospitalized two months back and was given symptomatic treatment. However, no investigations were done. There was no history of diabetes, hypertension, bronchial asthma, tuberculosis, blood transfusion or surgery in the past.
He was a vegetarian. His bladder and bowel habits were normal but his appetite was reduced. He was chronic bidi smoker since last 15-20 years and smoked 5-7 bidis per day. There was no other addiction.
General examination revealed mild pedal edema on both the lower limbs. There was no icterus, pallor, lymphadenopathy, clubbing or cyanosis. Vitals were within normal range. Local examination revealed dry gangrene over pulp of ring, middle and index fingers on the left hand and pulp of great toe and little finger on right hand. Approx. 1.5 x 1.5 cm ulcer was seen over dorsum of great toe of left foot. There was another ulcer, 1 x 1 cm in size over left dorsal foot at lower end of great toe. The ulcers were superficial with sloping edges, indurated, non tender, painless, with no discharge or bleeding. The patient was not able to extend the hands completely or hold anything tightly. Higher mental functions, motor system and reflexes were normal. Sensations and arterial pulsations of both the upper and lower limbs were normal. Examination of other systems was unremarkable.
At the time of admission, his hemoglobin was 11.5 gm%, white blood cells were 16070/ cu.mm and platelets were 407000/ cu.mm. Urine routine microscopy, renal and liver function tests were within normal limits. ESR was 54 mm/hr, RA factor was elevated to 256 IU/ml, CRP was 33 mg/l and S. albumin was 2.7 gm/dl. pANCA was positive and Anti CCP titre was >200 U/ml.

USG abdomen showed moderate right sided hydronephrosis with raised cortical echogenicity. X ray of right hand AP Oblique view revealed reduced joint space in 2nd and 3rd carpo-metacarpal joints with periarticular osteopenia. Left lower limb arterio-venous doppler showed intimo-medial thickening with normal color uptake wave form in common femoral artery, superficial femoral artery, popliteal artery, anterior tibial artery and dorsalis pedis artery. Nerve conduction study showed severe axonal sensorimotor polyneuropathy. Biopsy from the ulcer revealed hyperkeratosis with parakeratosis with neutrophilic abscesses. Dermis showed exuberant granulation tissue with no evidence of vasculitis. Nerve biopsy taken from right sural nerve was normal. Based on above findings, the patient was diagnosed as rheumatoid arthritis with vasculitis with neuropathy.
He was given empirical broad spectrum antibiotics (third generation cephalosporins) with symptomatic and supportive treatment. After confirmation of diagnosis, hydroxychloroquine, methotrexate and prednisolone were started. Pregabalin and other supportive treatment with fluid and multivitamins were also given. Cyclophosphamide was given once a month. Regular ulcer dressings were done. Repeat white blood cells count after five days of admission decreased to 9140/ cu.mm after treatment. The patient improved symptomatically and was discharged with advise to followup.
Discussion
Forty percent of Rheumatoid Arthritis (RA) patients develop extraarticular manifestations which results in increasing morbidity and mortality. Systemic Rheumatoid Vasculitis (RV) is a rare complication of RA with 1% incidence rate. It is characterized by inflammation of mid-sized arteries and capillaries [1]. Almost 90% cases of RV present with cutaneous manifestation (e.g; nail-fold lesions, palpable purpura and leg ulcers) [2]. Scleritis (0.3–6.3%), pericarditis (<10%), aortitis, pulmonary vasculitis and necrotizing glomerulonephritis are seen less commonly (8%).
A long standing history of RA (generally >10 years in duration), male sex, smoking, rheumatoid nodules and HLA class I and class II genotypes have been reported to be the risk factors for RV which is seen mostly in rheumatoid factor seropositivite cases [3-5]. A case report and literature review by Kanoko S et al observed that 4% of active noninfectious aortitis cases, had RA [6,7]. Although, at the time of presentation of RV, disease activity of RA is low (burnt out), RV in itself has a particularly poor outcome [8] with five year mortality estimated to be about 40% and is attributed to immune complex deposits (detected at vaculitis onset) [1]. leading to inflammation of vessel walls and end-organ damage [3,9].
Vasculitic neuropathy may present as mononeuritis multiplex or distal symmetric sensory neuropathy [10]; distal symmetric sensory or sensorimotor pattern is more commonly seen. A study suggested that ischemia due to necrotizing vasculitis of vasa nervorum was the main cause of peripheral neuropathy in rheumatoid vasculitis [10].
Cyclophosphamide and prednisone have been used in cases of severe systemic RA vasculitis but both may be considerably toxic [11]. Rituximab and glucocorticoids combination has lower toxicity and better response rates and preserves fertility, hence it is preferred over cyclophosphamide in patients at risk of cancer, renal failure, non compliant and young patients. Rituximab and cyclophosmamide can replace each other in case of lack of response to either after two months of treatment [11]. There are no head to head randomized controlled studies comparing cyclophosphamide and rituximab for treatment of RV.
As there are no specific guidelines at present for the treatment of rheumatoid vasculitis, proper treatment of RA to prevent development of extravascular complications becomes important, a decrease in rheumatoid vasculitis was observed with the increased use of methotrexate, corticosteroids and DMARDs [9] and when hydroxychloroquine was combined with low dose aspirin [1]. However, the effect of biologics on incidence of RV has been varied [12].
Another common complication of long standing RA is Lower Extremity (LE) ulcers mostly located above malleolus, on tips of toes and on the plantar aspect of heads of metatarsals [13]. Self The point prevalence of LE ulcers in RA has been reported to be 3.13% [13]. Age, pressure (due to ill fitting shoes, foot deformity and appliances), immobility, reduced ankle movement, venous thrombosis, increased disease activity and current glucocorticoid therapy have been suggested as the risk factors [14]. Risk due to vasculitis and duration of disease was found to be different in different studies [13,14]. RA itself increases risk of mortality when mostly due to cardiovascular events [15]. Another study reported that mortality rate in patients of RA with LE ulcers was twice as compared to those without LE ulcers.
By virtue of their location and course, LE ulcers lead to deterioration in quality of life of RA patients. Many may need surgical limb amputation significantly increasing the morbidity. They need to be managed using multi-disciplinary approach involving rheumatologists, wound care nurse, podiatrist and other disciplines such as vascular medicine or dermatology as needed.
Our case had three risk factors for development of RV; long history (untreated), male gender and smoking and presented with gangrenous tips of fingers due to vasculitis, Other than being seropositive RA, this case was also left untreated for long so may be an example of extra articular manifestations due to lack of treatment. He also had LE ulcers, one of the most common manifestations of RV. However, unlike the previous reports which suggested ischemic mechanism to be the most likely cause of nerve involvement in rheumatoid vasculitis, the biopsy of ulcers in our case did not show any evidence of vasculitis.
Conclusion
This case emphasizes the importance of timely diagnosis and good lower extremity examination with proper treatment of RA in time. Awarenesss of extraarticular complications and their impact on quality of life may improve access and compliance to treatment, thereby reducing the associated morbidity and mortality.
References
- Vasculitis associated with rheumatoid arthritis: A case–control study. Rheumatology. 2014; 53: 890–899.
- Scott DG, Bacon PA, Tribe CR. Systemic rheumatoid vasculitis: A clinical and laboratory study of 50 cases. Medicine (Baltimore). 1981; 60: 288.
- Voskuyl AE, Zwinderman AH, Westedt ML, et al. Factors associated with the development of vasculitis in rheumatoid arthritis: results of a case-control study. Ann Rheum Dis. 1996; 55: 190.
- Geirsson AJ, Sturfelt G, Truedsson L. Clinical and serological features of severe vasculitis in rheumatoid arthritis: prognostic implications. Ann Rheum Dis. 1987; 46: 727.
- Mongan ES, Cass RM, Jacox RF, et al. A study of the relation of seronegative and seropositive rheumatoid arthritis to each other and to necrotizing vasculitis. Am J Med. 1969; 47: 23.
- Okhravi N, Odufuwa B, McCluskey P, et al. Surv Ophthalmol. 2005; 50: 351.
- Kaneko S, Yamashita H, Sugimori Y, et al. Rheumatoid arthritis-associated aortitis: a case report and literature review. Springerplus. 2014; 3: 509.
- Helmick CG, Felson DT, Lawrence RC, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the USA- Part I. Arthritis & Rheum. 2008; 58: 15–25.
- Myasoedova E, Crowson CS, Turesson C, et al. Incidence of extraarticular rheumatoid arthritis in Olmsted County, Minnesota, in 1995-2007 versus 1985-1994: a population-based study. J Rheumatol. 2011; 38: 983.
- Puéchal X, Said G, Hilliquin P, et al. Peripheral neuropathy with necrotizing vasculitis in rheumatoid arthritis. A clinicopathologic and prognostic study of thirty-two patients. Arthritis Rheum. 1995; 38: 1618.
- Hellmann M, Jung N, Owczarczyk K, et al. Successful treatment of rheumatoid vasculitis-associated cutaneous ulcers using rituximab in two patients with rheumatoid arthritis. Rheumatology (oxford). 2008; 47: 929–930.
- Voskuyl AE, Zwinderman AH, Westedt ML, et al. The mortality of rheumatoid vasculitis compared with rheumatoid arthritis. Arthritis Rheum. 1996; 39: 266.
- Firth J, Hale C, Helliwell P, Hill J, Nelson EA. The prevalence of foot ulceration in patients with rheumatoid arthritis. Arthritis Rheum. 2008; 59: 200–205.
- Adlene J Jebakumar, P Deepak Udayakumar, Cynthia S. Crowson. Occurrence and Impact of Lower Extremity Ulcer in Rheumatoid Arthritis - A Population Based Study. J Rheumatol. 2014; 41: 437–443.
- Gabriel SE. Cardiovascular morbidity and mortality in rheumatoid arthritis. Am J Med. 2008; 121: S9–14.