
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
An unusual instance of acquired intraoral cavernous lymphangioma
Neetu Jain1*; Shashi Keshwar1; Ashish Shrestha1; Padamraj Neupane1; Anjani Kumar Yadav2; Iccha Kumar Maharjan3
1Department of Oral Pathology, College of Dental Surgery, B.P. Koirala Institute of Health Sciences, Dharan, Nepal.
2Department of Oral and Maxillofacial Surgery, College of Dental Surgery, B.P. Koirala Institute of Health Sciences, Dharan, Nepal.
3Department of Oral Medicine and Radiology, College of Dental Surgery, B.P. Koirala Institute of Health Sciences, Dharan, Nepal.
*Corresponding Author : Neetu Jain
Department of Oral Pathology, College of Dental Surgery, BP. Koirala Institute of Health Sciences, Dharan, Nepal.
Phone: +97-79804002736;
Email: neetu.jain@bpkihs.edu
Received : Jun 05, 2023
Accepted : Jun 23, 2023
Published : Jun 30, 2023
Archived : www.jcimcr.org
Copyright : © Jain N (2023).
Abstract
Lymphangiomas refers to hamartoma group and can be defined as rare congenital deformities caused by aberrant lymphatic vessel development, typically appear in infancy and the early years of childhood. They are rarely detected in the oral cavity and are typically found in the head and neck. Clinically, lymphangiomas can appear as localized or widespread growths that can expand to generate macroglossia of the tongue, which can cause speech impairment, mastication issues, airway obstruction, and other probable maxillofacial structure defects. Here, we disclose an acquired case of lymphangioma circumscripta in a 19 year old patient.
Keywords: Hamartoma; Lymphangioma; Macroglossia; Tongue.
Citation: Jain N, Keshwar S, Shrestha A, Neupane P, Yadav AK, et al. An unusual instance of acquired intraoral cavernous lymphangioma. J Clin Images Med Case Rep. 2023; 4(6): 2479.
Introduction
The term “hamartoma” refers to a benign, unifocal or multifocal, developmental aberration that consists of a mixture of cytologically normal, mature, local tissues and cells and displays an unorganized architectural outline with a predominance of one of the elements [1]. Lymphangioma refers to hamartomatous entities emerging from aberrant lymphatics which stop to drain into other lymphatics or veins, therefore causing lymph stagnation leading in the development of enormous cyst-like dilated lymphatics [2]. The majority of cases are seen in the anterior 2/3 of the dorsal part of the tongue, with the oral cavity being an infrequently implicated region. However, the palate, face, gingiva, lips, and alveolar ridges may also be affected on rare occasions [3]. Clinically, superficial lesions show up as raised nodules, vesicles that are pink, yellow, or translucent when aggregated, and over time due to subsequent hemorrhage, the lesion turns crimson or purple. The deeper lesions, however, present as soft, scattered lumps with normal color [4,5]. The anterior two-thirds of the tongue-involving oral lymphangiomas frequently result in macroglossia hence needs special attention [6].
Case presentation
A 19-year-old woman reported complaining about a wound that has been there for six years. Initially sneaky increasing in size, without pain, scorching, or discomfort having hard meals and with no history of trauma. No prior history of bleeding or pus discharge, night time pain or any pertinent medical background and no significant negative habits were reported. Single, palpable, bilateral submandibular lymph nodes measuring approximately 9 x 7 mm2, non-tender, roughly round to oval in form, hard, and movable was also observed.



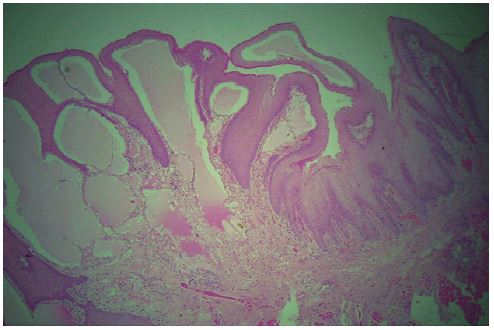
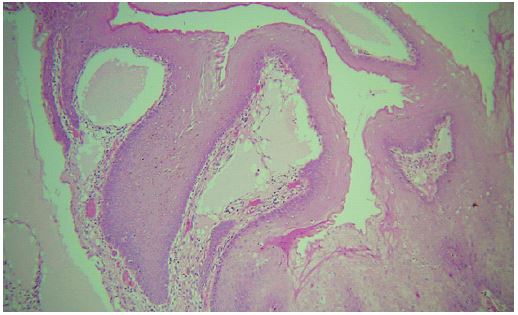
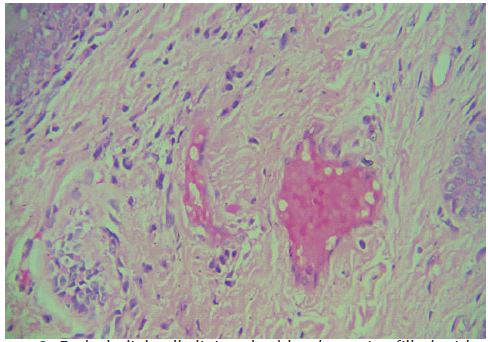
A biopsy with excision was carried out. The obtained specimen displayed a hyperplastic and parakeratotic stratified squamous epithelium with irregular rete ridges and papillomatous growth. Adjacent to the epithelial lining, there were areas with diffuse infiltration of amorphous, homogenous eosinophilic material lined by a single layer of endothelial cells with flattened, plump nuclei indicative of lymphatics of varying sizes with no sign of a capsule lining. Plasma lymphocytic infiltration also seemed to be present in the fibro-cellular stroma that underlies connective tissue. There were numerous endothelial cells lining the blood arteries, which were filled with engorged RBCs. Adipocytes, muscular fibres, and clumps of small salivary gland acini were visible in the deep section. Based on the above mentioned features an oral lymphangioma diagnosis was made. As there were large dilated lymphatic vessels, it was categorized as cavernous lymphangioma.



Discussion
Redenbacher initially described lymphangiomas in 1828; they are benign hamartomatous abnormalitie [7]. Two potential theories have been proposed to explain the etiopathogenesis of lymphangiomas. The primary understanding is that the lymphatic system progresses from five sacs of the venous system and endothelial out-pouching’s that spread outward from the jugular sac to create the lymphatic system. It is explained by a second school of thought that the lymphatic system originates from mesenchymal splits in the venous net and spreads in a centripetal manner to the jugular sac [8-10]. The obstructed lymphatic tubes that result from surgery, inflammation, infection, or trauma may be the acquired etiology of lymphangioma or lymphangiectasis. But in the above reported acquired case of lymphangioma there was no history of trauma, surgery or infection. The classification of lymphangiomas as real tumors or hamartomas, which are typically deformities brought on by the sequestration of lymphatic tissues that fail to establish normal connection with the lymphatic system and may cause proliferation, is under dispute [11].
In the oral cavity tongue is the most common site for the lesion to occur, involvement of anterior dorsal portion of the tongue often leads to macroglossia and uneven nodularity of the tongue’s surface with gray and pink projections which are superficial and gives pebbly appearance that looks like a collection of translucent vesicles or look of “frog eggs” or tapioca pudding are pathological characteristics of lymphangiomas of the tongue which was also evident in our reported case. These patients will experience speech difficulties, poor oral hygiene, and tongue bleeding due to oral trauma [12-14].
Typically, the deep lesions appear as submucosal masses. The deep lesions typically manifest as masses of diffuse growth, and depending on the anatomical location, they may cause damages like tissue swelling, obstruction of the upper airways, pain, tongue protrusion, sialorrhea, jaw deformity, as well as challenges with chewing, speaking, and performing oral hygiene [10,15].
Although in most instance the lesion is congenital or seen during early years of childhood, we reported the case in a 19 year old female.
Histopathologically, there are several different types of Lymphangiomas [16].
• Lymphangioma simplex (capillary lymphangioma) consists of small, capillary sized vessels
• Cavernous lymphangioma composed of large, dilatedlymphatic vessels
• Cystic lymphangioma (cystic hygroma) exhibits largemacroscopic cystic spaces.
• Benign lymphoendothelioma (lymphatic channel appears to be dissecting through dense collagen bundles)
Additionally, this is categorized into macrocystic (cavities greater than or equal to 2 cm), microcystic (cavities smaller than or equal to 2 cm), and mixed, which combines these two categories [17]. Genetic conditions such Turner, Edwards, Down, Noonan, and Patau syndromes are seen in conjunction with congenital lymphangiomas [12].
On a microscopic level, Lymphangioma is distinguished by dilated lymph channels that produce a single or several cystic areas. The nearby soft tissues will frequently become diffusely infiltrated by the arteries. Another distinguishing trait of Lymphangioma is the presence of benign lymphoid aggregates in the channel walls. Endothelial cells line the channels. In addition to lymphatic fluid, red blood cells, neutrophils, macrophages, and lymphocytes may also be present in the lumen. In our case, similar histopathologic characteristics were also present. In the deeper layers of the mucosa, dilated lymphatic vessels with thicker muscle walls may be visible [18].
A mix of traditional clinical characteristics, histological analysis, and some imaging techniques are used to make the diagnosis of lymphangioma. The imaging modalities ultrasonography and angiography are frequently employed [19].
For surgical planning, the lesion’s extension needs to be precisely demarcated. Unilocular or multilocular cystic masses with smooth, thin, thick, or uneven walls are frequently seen on ultrasound imaging [20]. On T1-weighted Magnetic Resonance (MR) images, lymphangioma is isointense to muscle and hyper intense to fat. According to research, MR imaging clearly distinguishes the malignant lesion extension from ultrasound and Computer Tomography (CT) scans [20].
Numerous conditions are on the differential diagnosis list, including primary muscle hypertrophy, congenital hypothyroidism, hemangioma, and neurofibromatosis [21]. Aesthetic, occlusal, functional, and psychosocial lymphangioma problems can have an impact on individuals, particularly those in the pediatric age group [22]. Ludwig’s angina, sadly, can occasionally develop when an infection arises [23]. Additional documented surgical problems include seroma development, recurrent cellulitis, mild bleeding, and lymph fluid leaking [24].
Tongue lymphangiomas have been treated using a variety of therapeutic techniques. The preservation of taste perception, restoration of the tongue’s size for articulation, and cosmetics are the key goals of treatment for tongue lymphangiomas.The several treatment options for lymphangioma include laser surgery with Nd YAG, CO2 and radiofrequency tissue ablation technology. They also include radiation therapy, cryotherapy, electrocautery, sclerotherapy, steroid administration, embolization, and ligation. The preferred course of treatment for lymphangiomas that are encapsulated or partially confined is surgical excision [25,26]. Encapsulation is not always complete, hence it becomes inevitable for cells to infiltrate nearby tissues. If important structures are not harmed, a successful treatment needs the presence of a border of normal tissue [27]. Because of its infiltrative nature, reoccurrence is frequent. The recurrence rate for lymphangiomas is 39%, according to the research of Orvidas and Kasperbauer. A regular follow-up is therefore required [28].
Conclusion
In the oral cavity, acquired cavernous lymphangioma are not very common. We have highlighted this example to clear up the fact that, although if the lesion is primarily congenital, it should be taken into account in later life. Macroglossia and further consequences can be avoided with early detection and treatment. An accurate diagnosis of the lesions will be provided by appropriate clinical and histopathological evaluation.
Declarations
Data availability: Data can be provided on reader’s request.
Contributors: Neetu Jain, Shashi Keshwar, Ashish Shrestha, PadamRaj Neupane, Anjani Kumar Yadav, Iccha Kumar Maharjan.
Patient consent: Obtained.
Financial support and sponsorship: Nil.
Conflicts of interest: There are no conflicts of interest.
References
- Patil S, Rao RS, Majumdar B. Hamartomas of the oral cavity. Journal of International Society of Preventive and Community Dentistry. 2015; 5: 347-353.
- Joshi PS, Hongal B, Sanadi A. Cystic lymphangioma: A differential diagnosis. Journal of Oral and Maxillofacial Pathology: JOMFP. 2015; 19: 393.
- Gupta S, Ahuja P, Rehani U, Singh V. Lymphangioma of cheek region–an unusual presentation. Journal of oral biology and craniofacial research. 2011; 1: 47-49.
- Goswami M, Singh S, Gokkulakrishnan S, Singh A. Lymphangioma of the tongue. National Journal of Maxillofacial Surgery. 2011; 2: 86
- Bhayya H, Pavani D, Tejasvi MA, Geetha P. Oral lymphangioma: A rare case report. Contemporary clinical dentistry. 2015; 6: 584.
- Sunil S, Gopakumar D, Sreenivasan BS. Oral lymphangioma–Case reports and review of literature. Contemporary clinical dentistry. 2012; 3: 116.
- Kurude AA, Phiske MM, Kolekar KK, Nayak CS. Lymphangiomas: rare presentations in oral cavity and scrotum in pediatric age group. Indian Journal of Dermatology, Venereology and Leprology. 2020; 86: 230.
- Suen JY. Treatment of oral cavity vascular malformations using the neodymium: YAG laser. Archives of Otolaryngology–Head & Neck Surgery. 1989; 115: 1329-1333.
- Hong JP, Lee MY, Kim EK, Seo DH. Giant lymphangioma of the tongue. Journal of Craniofacial Surgery. 2009; 20: 252-254
- Jian XC. Surgical management of lymphangiomatous or lymphangiohemangiomatousmacroglossia. Journal of oral and maxillofacial surgery. 2005; 63: 15-19.
- Weiss SW. Tumors of lymph vessels. Enzinger and Weiss’s soft tissue tumors. 2001: 955-983.
- Shulman LP, Emerson DS, Felker RE, Phillips OP, Simpson JL, Elias S. High frequency of cytogenetic abnormalities in fetuses with cystic hygroma diagnosed in the first trimester. Obstetrics & Gynecology. 1992; 80: 80-82.
- Colangeli W, Facchini V, Kapitonov A, Zappalà M, Bozza F, Becelli R, et al. Cystic lymphangioma in adult: A case report and a review of the literature. Journal of Surgical Case Reports. 2020; 2020: rjaa179.
- Neville BW, Damm DD, Allen CM, Bouquet JE. Soft tissue tumors. In: Neville BW, editor. Oral and Maxillofacial Pathology. 2nded. New Delhi, Philadelphia: Saunders Publishers. 2002; 475 477.
- Balakrishnan A, Bailey CM. Lymphagioma of the tongue. A review of pathogenesis, treatment and the use of surface laser photocoagulation. The Journal of Laryngology & Otology. 1991; 105: 924-929.
- Rajendran R, Sundaram S. Shafer’s textbook of oral pathology. (6th edn), Elsevier India, 2009; 12: 146-148.
- Brad Neville, Douglas D Damm, Carl Allen, Angela Chi, et al. Oral and Maxillofacial Pathology. WB Saunders, Philadelphia. 1995; 395.
- Leboulanger N, Roger G, Caze A, Enjolras O, Denoyelle F, Garabedian EN, et al. Utility of radiofrequency ablation for haemorrhagic lingual lymphangioma. International journal of pediatric otorhinolaryngology. 2008; 72: 953-958.
- cAlvany JP, Jorizzo JL, Zanolli D, Auringer S, Prichard E, et al. Magnetic resonance imaging in the evaluation of lymphangiomacircumscriptum. Archives of dermatology. 1993; 129: 194-197.
- Yoganna SS, Prasad RG, Sekar B. Oral lymphangioma of the buccal mucosa a rare case report. Journal of pharmacy &bioallied sciences. 2014; 6: S188.
- Pui MH, Li ZP, Chen W, Chen JH. Lymphangioma: imaging diagnosis. Australasian radiology. 1997; 41: 324-328.
- Greenberg M, Glick M, Ship J. Burket’s oral medicine. Elevent Edition. BC Decker Inc.; 2008; 140.
- Uguru C, Edafioghor F, Uguru N. Lymphangioma of the tongue with macroglossia: a case report. Nigerian Journal of Medicine: Journal of the National Association of Resident Doctors of Nigeria. 2011; 20: 166-168.
- Tasca RA, Myatt HM, Beckenham EJ. Lymphangioma of the tongue presenting as Ludwig’s angina. International journal of pediatric otorhinolaryngology. 1999; 51: 201-205.
- Hancock BJ. st-vil d, luks fi, di lorEnzo M, Blan Chard h. Complications of lymphangiomas in children. J Pediatr Surg. 1992; 27: 220-224.
- Kennedy TL. Cystic hygroma‐lymphangioma: A rare and still unclear entity. The Laryngoscope. 1989; 99: 1-0.
- Puri N. Treatment options of lymphangioma circumscriptum. Indian Dermatology Online Journal. 2015; 6: 293-294.
- Schefter RP, Olsen KD, Gaffey TA. Cervical lymphangioma in the adult. Otolaryngology–Head and Neck Surgery. 1985; 93: 65-69.
- Orvidas LJ, Kasperbauer JL. Pediatric lymphangiomas of the head and neck. Annals of Otology, Rhinology & Laryngology. 2000; 109: 411-421.