
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Negative pressure pulmonary oedema and alveolar haemorrhage due to upper airway obstruction after parathyroidectomy
Christian M Beilstein*; Dominque Engel; Lutz E Lehmann; Patrick Y Wuethrich
Department of Anaesthesiology and Pain Medicine, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland.
*Corresponding Author : Christian M Beilstein
Department of Anaesthesiology and Pain Medicine, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland.
Tel: 0041-31-632 21 11;
Email: Christian.Beilstein@insel.ch
Received : Jun 02, 2023
Accepted : Jun 26, 2023
Published : Jul 03, 2023
Archived : www.jcimcr.org
Copyright : © Beilstein CM (2023).
Abstract
A 36-year old female underwent elective parathyroidectomy at a Swiss tertiary teaching hospital for primary hyperparathyroid-ism. Induction, surgery and extubation were uneventful. During transfer to the post-anaesthetic care unit, some retching was interpreted as vomiting. At arrival, she was apnoeic and unresponsive but with palpable pulse. During bag mask ventilation, a subtle in- and expiratory stridor was audible. After application of naloxone, spontaneous ventilation resumed and the patient regained consciousness. The surgical site was unremarkable. A chest X-ray showed pulmonary oedema, arterial blood gas analysis severe hypoxaemia and hypercapnia. Assuming a negative pressure pulmonary oedema, Non-Invasive Ventilation (NIV) was initiated for two hours. 15 minutes thereafter, she experienced hypertension and foamy haemoptysis. NIV was restarted, intravenous nitro-glycerine and furosemide given. After two hours with clinical recovery and normalised gas exchange, treatment was weaned. Due to the stridor, most likely cause of upper airway obstruction was laryngospasm. Differential diagnosis was airway collapse due to residual anaesthetics. Negative pressure pulmonary oedema due to upper airway obstruction is a rare but potentially severe complication usually occurring in young, healthy patients after laryngospasm. Upper airway obstruction might present atypically, delaying recognition and treatment. If treated adequately, negative pressure pulmonary oedema usually resolves without sequelae.
Keywords: General anaesthesia; Pulmonary oedema; Non-invasive ventilation; Laryngospasm.
Citation: Beilstein CM, Engel D, Lehmann LE, Wuethrich PY. Negative pressure pulmonary oedema and alveolar haemorrhage due to upper airway obstruction after parathyroidectomy. J Clin Images Med Case Rep. 2023; 4(7): 2481.
Introduction
Negative pressure pulmonary oedema (also called post-obstructive pulmonary oedema) is a rare but potentially severe complication usually occurring in young, healthy patients undergoing general anaesthesia. It may happen in up to 0.1% of all general anaesthetics and usually resolves within 24 hours [1]. In adults, the most frequent cause is laryngospasm; others are tube obstruction due to secretions or biting, bleeding or airway oedema [2,3]. Detection of laryngospasm might be difficult due to atypical presentation in up to 23% [4]. Negative pressure pulmonary oedema might be associated with pulmonary haemorrhage and require invasive or non-invasive mechanical ventilation for up to three days [5-7]. Differential diagnosis includes aspiration pneumonitis, pulmonary embolism, anaphylaxis, volume overload and cardiogenic or neurogenic pulmonary oedema [8]. Besides the previously described negative pressure pulmonary oedema due to acute airway obstruction (Type I), the literature describes a more rare form: after resolution of a chronic airway obstruction, formerly producing intrinsic PEEP being eliminated by removing the airway obstruction (Type II) [8].
Case presentation
A 36-year old female of African origin (height: 167 cm, weight: 76 kg) underwent elective parathyroidectomy at a Swiss tertiary teaching hospital for primary hyperparathyroidism. She had a gastric bypass about one year before this surgery but was other-wise healthy. The hyperparathyroidism was an incidental finding during bariatric workup. Total intravenous general anaesthesia was induced using fentanyl, propofol and suxamethonium as an indication for rapid sequence induction was given. To facilitate monitoring of the recurrent laryngeal nerve, no further neuromuscular blocking drugs were administered. During laryngoscopy, airway secretions mandated a second attempt, but tracheal intubation was otherwise uneventful (percentage of glottis opening < 75% using video laryngoscopy, C-MAC™). Depth of anaesthesia was measured using processed electroencephalogram (BIS™), and recovery from neuromuscular blockade was confirmed prior to incision. Surgery lasted 43 minutes, and in total 500 mcg of intravenous fentanyl were given. At the surgeon’s request, 40 mg of intravenous methylprednisolone were added. Extubation was performed when the patient was breathing on command and opened her eyes. During transfer to the postanaesthetic care unit (PACU), the patient started to retch. This was interpreted by a young resident as early vomiting, so she was turned on her right side. At PACU arrival, the patient was apnoeic, unresponsive and saturation was undetectable, but pulse was palpable. During the immediately commenced bag mask ventilation, a subtle in- and expiratory stridor was audible. After application of naloxone for presumed opioid overdose, spontaneous ventilation resumed, saturation recovered to 90% and the patient regained conscious-ness without neurologic deficits. A chest X-ray showed marked pulmonary oedema (Figure 1), the blood gas analysis revealed severe hypoxaemia and hypercapnia (Horowitz index 52, Table 1).
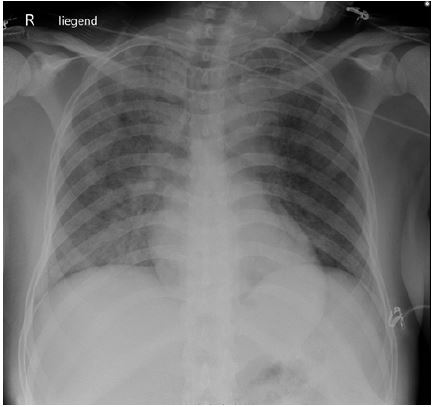
Table 1: Arterial blood gas analyses.
| Time point | Admission | + 90 minutes | + 300 minutes |
|---|---|---|---|
| Haemoglobin (g l-1) | 128 | 124 | 123 |
| Sodium (mmol l-1) | 143 | 141 | 142 |
| Potassium (mmol l-1) | 4.3 | 3.7 | 3.7 |
| Chloride (mmol l-1) | 109 | 110 | 105 |
| Calcium, ionised (mmol l-1) | 1.4 | 1.28 | 1.17 |
| Glucose (mmol l-1) | 8.5 | 7.2 | 9.1 |
| Lactate (mmol l-1) | 2.6 | 0.9 | 1.1 |
| pH | 7.212 | 7.354 | 7.414 |
| pO2 (mmHg) | 52 | 77 | 122 |
| O2 saturation (%) | 80 | 95 | 98 |
| pCO2 (mmHg) | 67 | 48 | 42 |
| Bicarbonate (mmol l-1) | 21.7 | 24.7 | 26.4 |
| Base excess (mmol l-1) | -0.5 | 1.0 | 2.4 |
| fiO2 | 100 | 35% | 35% |
| Horovitz index (pO2/fiO2) 1 | 52 | 220 | 349 |
1calculated value.
Assuming a negative pressure pulmonary oedema, the surprisingly asymptomatic patient was treated with non-invasive ventila-tion (NIV) for two hours (PEEP 5 mmHg, pressure support 5 mmHg, fiO2 35%) with good tolerability. Gas exchange improved, but was still impaired (Horowitz index 220, Table 1). After cessation of NIV based on improvement of gas exchange and formi-dable clinical appearance, the patient experienced an episode of arterial hypertension and foamy haemoptysis within 15 minutes. Therefore, NIV was restarted, intravenous furosemide given and a continuous infusion of nitro-glycerine started. After two more hours of NIV, treatment was stopped after complete clinical recovery and normalisation of gas exchange (Horowitz index 349, Table 1). The patient was weaned off intravenous medication and discharged to the surgical ward the next morning. In standard postoperative Ear-Nose-Throat (ENT) assessment, fibre-optic laryngoscopy revealed a hypo mobile left vocal cord not present preoperatively. She left hospital the following day after full recovery.
Discussion
This patient suffered a rare but severe complication after general anaesthesia, requiring prompt recognition and effective treat-ment: upper airway obstruction with consecutive negative pressure pulmonary oedema. As there was no bleeding at the surgical site and a subtle stridor audible during bag mask ventilation, airway obstruction was most likely caused by laryngospasm. Potentially, an overdose of anaesthetics and/or opioids, leading to low consciousness and airway collapse, might have been causal or contributing in this case. The unilateral vocal cord palsy revealed the following day is unlikely to be the only cause, as acute bilateral vocal cord palsy is required for airway obstruction.
In absence of a surgical complication such as bleeding, primary therapy is rapid relief of airway obstruction by jaw thrust, bag mask ventilation and gentle airway suctioning if needed. In severe cases of laryngospasm, induction or deepening of anaesthesia or neuromuscular blockade might be necessary to restore airway patency. Thereafter, positive pressure ventilation (invasive or non-invasive) is the mainstay of treatment in case of negative pressure pulmonary oedema. Supportive measures can be diuretics and vasodilators, although evidence is weak [2]. To exclude other causes of pulmonary oedema, investigations such as electrocardiogram, echocardiography, markers of myocardial ischaemia or further imaging may be indicated, although not required in this case. Negative pressure pulmonary oedema usually resolves within 24 hours without sequelae if treated adequately, but might require treatment for up to 72 hours.
The upper airway obstruction was initially not detected in this case but rather interpreted as retching and early vomiting. This highlights the importance of being aware of abnormal presentations of laryngospasm and maintaining high vigilance regarding airway patency even in young and healthy patients after general anaesthesia. This is especially true during the transfer process, when clinicians are distracted by protocol completion, location change or handover.
Conclusion
High vigilance regarding airway patency is required during all treatment phases, especially during transfer, even in young and healthy patients. In case of negative pressure pulmonary oedema, it may be advisable to wait for complete normalisation of gas exchange before cessation of treatment to prevent relapsing symptomatology as experienced in this case.
Declarations
Author contributions: Writing-original draft preparation, C.B.; writing-review and editing, C.B., D.E., L.L., P.W. All authors have read and agreed to the published version of the manuscript.”
Funding: This research received no external funding.
Institutional review board statement: Not applicable.
Informed consent statement: Written informed consent has been obtained from the patient to publish this paper.
Conflicts of interest: The authors declare no conflict of interest.
References
- McConkey PP. Postobstructive pulmonary oedema--a case series and review. Anaesth Intensive Care. 2000; 28: 72-76.
- Alb M, Tsagogiorgas C, Meinhardt JP. [Negative-Pressure Pulmonary Edema (NPPE)]. Anasthesiol Intensivmed Notfallmed Schmerzther. 2006; 41: 64-78.
- Lang SA, Duncan PG, Shephard DA, Ha HC. Pulmonary oedema associated with airway obstruction. Can J Anaesth. 1990; 37: 210-218.
- Visvanathan T, Kluger MT, Webb RK, Westhorpe RN. Crisis management during anaesthesia: laryngospasm. Quality & Safety in Health Care. 2005; 14: e3.
- Patel AR, Bersten AD. Pulmonary haemorrhage associated with negative-pressure pulmonary oedema: A case report. Crit Care Resusc. 2006; 8: 115-116.
- Andersen C, Kancir CB, Nielsen KD. Laryngospasm-induced pulmonary oedema. Acta Anaesthesiol Scand. 1988; 32: 710-711.
- Majewski J, Górnik-Właszczuk E, Koczy B, Szczygieł R. [Negative pressure pulmonary oedema and haemorrhage]. Anestezjologia Intensywna Terapia. 2010; 42: 90-93.
- Udeshi A, Cantie SM, Pierre E. Postobstructive pulmonary edema. J Crit Care. 2010; 25: 538.e1-.e5.