
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 4
Management of aortoesophageal fistula & pseudoaneurysm induced by impacted chicken bone
Philip Berry1; Usman Raja2; Cara Baker3; Sreelakshmi Kotha1*; Morad Sallam4
1Department of Gastroenterology, Guy’s and St Thomas’ Foundation Trust, London, United Kingdom.
2Department of Interventional Radiology, Guy’s and St Thomas’ Foundation Trust, London, United Kingdom.
3Department of Gastrointestinal Surgery, Guy’s and St Thomas’ Foundation Trust, London, United Kingdom.
4Department of Vascular Surgery, Guy’s and St Thomas’ Foundation Trust, London, United Kingdom.
*Corresponding Author : Sreelakshmi Kotha
Department of Gastroenterology, Guy’s and St Thomas’ Hospital, London, UK.
Tel: 00447949871727
Email: sreelakshmi-kotha@yahoo.com
Received : Jun 08, 2023
Accepted : Jun 30, 2023
Published : Jul 07, 2023
Archived : www.jcimcr.org
Copyright : © Kotha S (2023).
Abstract
Although foreign body ingestion and food bolus obstruction are frequently encountered gastrointestinal emergencies, the management of sharp objects in the oesophagus remains highly challenging due to the risk of perforation. We present the case of a 44-year-old patient with an impacted chicken bone penetrating into the aortic arch. The importance of a swift and effective multidisciplinary approach involving interventional radiology, vascular surgery, upper gastrointestinal surgery and endoscopy was illustrated.
Citation: Berry P, Raja U, Baker C, Kotha S, Sallam M. Management of aortoesophageal fistula & pseudoaneurysm induced by impacted chicken bone. J Clin Images Med Case Rep. 2023; 4(7): 2490.
Introduction
Food Bolus Obstruction (FBO) and Foreign Body Ingestion (FBI) account for 4% of emergency gastroscopies [1]. FBO is common in adults and can include animal bones, dentures and food mass (‘steakhouse syndrome’), whereas FBI is mostly seen in paediatric population. Most cases of FBO have an underlying oesophageal pathology like eosinophilic oesophagitis, motility disorder or anatomical abnormality such as diverticula or known strictures. Symptoms include dysphagia, retrosternal pain, odynophagia and vomiting.
Case presentation
A 44 year-old patient was admitted following a collapse in a supermarket requiring bystander cardiopulmonary resuscitation with return of spontaneous circulation. Relatives reported he had complained of chest discomfort following a chicken meal two days before. There was no significant past medical or surgical history. The patient was intubated and ventilated, apyrexic, and cardiovascularly stable. All systems were normal on examination Investigations revealed haemoglobin 88 g/L, white cell count of 7.9 x 109 /L, C-reactive protein 62 mg/L and normal renal/liver function. Electrocardiogram was normal. Chest x-ray was not informative. Thoraco-abdominal Computed Tomography (CT) scan demonstrated a ‘V’ shaped object lodged in the lumen of the upper oesophagus penetrating through to the wall of the aortic arch and a small pseudoaneurysm arising from the arch’s medial aspect (Figure 1A & 1B).
Initial management
Following discussion with surgical, Interventional Radiology (IR) and vascular teams, an endoscopic approach in theatres with IR and surgical backup was adopted. 3-dimensional reconstruction of the foreign body allowed pre-procedural planning including preferred direction of endoscopic extraction. At endoscopy, the uppermost limb of the bone was seen to traverse the oesophageal lumen with both ends penetrating the mucosa (Figure 1C). The apex of the ‘V’ was secured with graspers and the bone was removed at the previously agreed angle (Figure 1D). There was no visible luminal bleeding, and no aortic leak on an on table angiogram. Within 24 h the patient developed melaena with a 2 g/L drop in haemoglobin. CT angiogram indicated likely aortic adventitial tear, and emergency Thoracic Endovascular Aortic Repair (TEVAR) was performed. Following extubation the patient developed left sided weakness. Magnetic resonance imaging confirmed multiple infarcts involving the right anterior and middle cerebral artery territories. He was commenced on 300 mg of aspirin and stroke team was consulted. He was commenced on nasojejunal feeding.
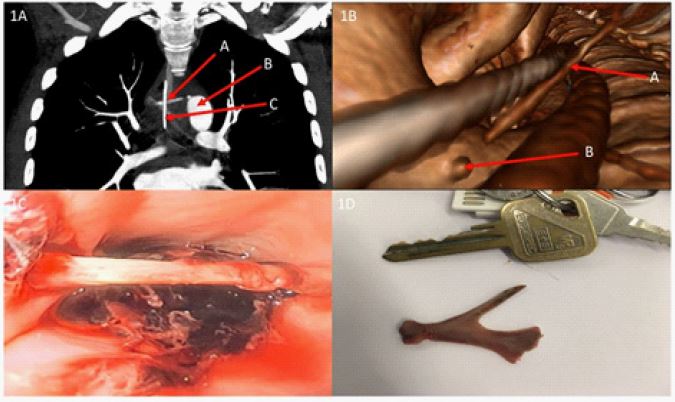
Figure 1B: CT reconstruction: view in a caudal direction shows two tubular structures (oesophageal temperature probe and NG tube) and the upper limb of the bone crossing diagonally (A). The oesophageal walls are not shown. Near the end of the bone there is a small pouch (B) arising from the medial wall of the aorta.
Figure 1C: Endoscopic view: the upper limb of the V-shaped bone is seen, its two ends embedded in the oesophageal mucosa.
Figure 1D: Chicken bone, after removal. A door key is shown for scale. The narrower limb was lying uppermost and was closest to the aorta.
Progression and outcome
Following neurorehabilitation he was discharged 16 days later on dual antiplatelet therapy. Vascular and infectious disease teams recommended 6 weeks of antibiotics and antifungals, delivered through a PICC line in case of graft infection. At 3 months the patient had no residual neurological deficit. He required positron emission tomography scans at 6 months and one year to detect any graft infection; these scans were clear and patient has been discharged.
Discussion
Less than 1% of FBO or FBI presentations require surgery [2]. Risks of life threatening complications like haemorrhage, perforation and injury to surrounding organs is the highest in oesophageal impaction by sharp objects. Hyper-salivation and inability to swallow saliva indicates complete obstruction of oesophagus and requires emergent endoscopy [3]. Endoscopy is recommended within 12 hrs of impaction but within 6 hrs is preferable to avoid perforation and fistula formation [4]. Fizzy drinks and pharmacological agents like glucagon have been shown to be helpful but these should not be used in cases of sharp objects or as alternatives to emergent endoscopy [5,6]. Most complications occur prior to endoscopic retrieval, so careful examination is required. If perforation or injury to vascular organs is suspected, appropriate imaging and discussion with surgical teams to agree a management plan is required. Various endoscopic instruments including caps, over-tubes, snares, forceps and nets can be used to retrieve these objects. Early recognition of perforation may permit endoscopic management with fully covered metal stent placement or closure using clips, thus reserving surgery for the most complex cases.
Summary
→ Collateral history is vital in cases of unexplained collapse.
→ Chest radiographs do not reliably exclude foreign body impaction or perforation.
→ Emergent endoscopic retrieval is indicated within 12 hrs of oesophageal impaction.
→ Early recognition of complications and appropriate imaging is required in cases of sharp foreign bodies.
→ Airway protection prior to emergent endoscopy is strongly recommended.
→ A multidisciplinary approach is required for complex cases.
Declarations
Funding: No funding involved
Disclosures: No conflicts of interest.
Funding: No financial support or competing interests.
Consent: Consent has been received from patient.
References
- Mosca S, Manes G, Martino R, Amitrano L, Bottino V, et al. Endoscopic management of foreign bodies in the upper gastrointestinal tract: report on a series of 414 adult patients. Endoscopy. 2001; 33: 692-696.
- ASGE Standards of Practice Committee. Ikenberry SO, Kue TL, Andersen MA, Appalaneni V, Banerjee S, et al. Management of ingested foreign bodies and food impactions. Gastrointest Endosc. 2011; 73: 1085-1091.
- Ciriza C, García L, Suárez P, Jiménez C, Romero MJ, et al. What predictive parameters best indicate the need for emergent gastrointestinal endoscopy after foreign body ingestion? J Clin Gastroenterol. 2000; 31: 23-28.
- Mosca S. Management and endoscopic techniques in cases of ingestion of foreign bodies. Endoscopy 2000; 32: 272-273.
- Tibbling L, Bjorkhoel A, Jansson E, Stenkvist M. Effect of spasmolytic drugs on esophageal foreign bodies. Dysphagia. 1995; 10: 126-127.
- Lee J, Anderson R. Best evidence topic report. Effervescent agents for oesophageal food bolus impaction. Emerg Med J. 2005; 22: 123-124.