
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Isolated atlanto-occipital joint effusion presenting as cervicogenic vertigo
Sandeep Kumar1*; Nishi Gupta2; Preeti Madaan³
1Bharti ENT & Vertigo Clinic, UE-2, Jamalpur, Ludhiana-141010, India.
2Dr Shroff’s Charity Eye Hospital, Daryaganj, New Delhi-110002, India.
3Physiotherapist, The Ottawa Hospital, Civic Campus, Ottawa, ON, K1Y4E9, Canada.
*Corresponding Author : Dr. Sandeep Kumar
Bharti ENT & Vertigo Clinic, UE2, Jamalpur, Ludhiana-141010, India.
Ph: +91-981-419-4046;
Email: dr.sandeepsharma.ent@gmail.com
Received : Jun 18, 2023
Accepted : Jul 04, 2023
Published : Jul 11, 2023
Archived : www.jcimcr.org
Copyright : © Kumar S (2023).
Abstract
Objective: Cervical Vertigo is a controversial entity. Here we present an un reported case of Isolated Atlanto Occipital Joint effusion as a cause of Vertigo.
Case report: A 45-year-old male presented with imbalance, ataxia, swaying, quick spins, and oscillopsia, especially when turning his head. There were no oculomotor findings on videonystagmography. Magnetic resonance imaging for craniovertebral junction anomalies revealed atlanto-occipital joint effusion on the side on which the patient complained of quick spins on head turning. The patient was managed successfully with steroids and anti- inflammatory drugs.
Conclusions: To the best of our knowledge, this is the first case of isolated atlanto-occipital joint effusion as a cause of vertigo. The only other such case reported till date presented as migraine. We describe the clinical features, diagnosis, pathophysiology involved and importance of relevant imaging in such a case.
Keywords: Atlanto occipital joint; Craniovertebral junction; Cervical vertigo.
Citation: Kumar S, Gupta N, Madaan P. Isolated atlanto-occipital joint effusion presenting as cervicogenic vertigo. J Clin Images Med Case Rep. 2023; 4(7): 2494.
Introduction
Cervicogenic vertigo is a controversial entity. It usually manifests as ataxia and unsteadiness of gait. Vertigo of the spinning type is rare and difficult to explain on the basis of cervical spine defects. Still, clinicians do encounter rare cases where it becomes necessary to rule out causes related to the cervical spine.
The diagnosis becomes all the more important because many of these causes are easily treatable, as in our case. This is a unique case of vertigo due to atlanto occipital joint effusion.
Materials & methods
A 45-year-old male was referred to us with a history of vertigo not responding to treatment. There was no history of diabetes or hypertension. His symptoms started suddenly with a clicking sound in his neck when he tried to tilt his head backward to tie his turban.
He used to have a momentary feeling of falling backward while standing from a sitting position, especially after bending down to pray. He had imbalance and sideways swaying while walking, along with oscillopsia and the illusion of spinning on turning the car around a round a bout. When turning his head quickly to the left, he used to have problems focusing on objects and with sudden, quick spins, while on the right, there were no such symptoms. He also used to get mild oscillopsia while running.
His general physical examination was normal. Pure-to neaudiometry showed bilater allow-frequency sensori neural hearing loss at 500 Hz. Rhomberg was negative, but modified Rhomberg was positive, with sway not restricted to a particular side. Examination of various oculomotor and positional tests on Videonystagmography (VNG) did not reveal any abnormalities.
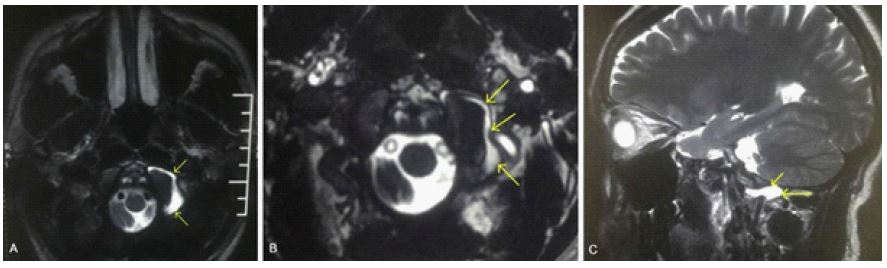
Since the patient’s complaints were linked to head and body motions manifesting when turning the car or standing up from a bending position, a magnetic resonance imaging of the brain and Cranio- Vertebral Junction was ordered. It revealed an isolated atlanto-occipital joint effusion on the left side (Figure 1).
On blood investigations, his erythrocytese dimentation rate was 8 mm/st hour, his C-reactive protein was 2.06 mg%, and his quantitative rheumatoid factor was 13.6 IU/ML. He was put on steroids and anti-inflammatory drugs for two weeks. The patient responded well to the treatment, with complete resolution of all his symptoms. After along follow-up off our years, the patient is symptom free with no episodes of recurrence.
Discussion
Brandt et al label cervical vertigo a controversial disorder. There is no reliable clinical test to demonstrate its independent existence [1]. Therefore, it is important to rule out other causes of vertigo like trauma, perilymph fistula cerebellar or spinal ataxia, vestibular paroxysmia, bilateral vestibulopathy, benign paroxysmal positional vertigo, etc. before labelling a patient as having cervical vertigo [1]. Various cranio vertebral junction afflictions, like Arnold chairi malformation, at lanto-occipital joint dislocation, or trauma in this region, have been reported to cause vertigo and dizziness.
For body and spatial orientation, both the position of the head in space (as judged by the vestibular system) and the position of the head in relation to the body (as judged by neck afferents) are of utmost importance [1]. Similarly, for correct perception of head and trunk rotations in space, combined information from both neck and vestibular stimulation is required [2]. Deep, short intervertebral neck muscles responsible for neck proprioception are richly supplied by muscle spindles³. Neck afferents synapse in vestibular nuclei and become integrated with the Vestibulo ocular reflex [1]. There is intense visual-vestibular-proprioceptive convergence at all levels of the central vestibular system, which is necessary for multisensory interaction in spatial orientation and postural control. The neck not only modulates body posture but also stabilizes the head in space by cervico colic reflexes, which are integrated with vestibulo colic reflexes [5,6].
Unilateral irritation or lesional deficit of neck input, as seen in our case, could cause a bilateral bone imbalance leading to the disturbed integration of visual, vestibular, and neck, i.e., body input [1].
It has been described by various authors who demonstrated that the unilateral vibration of posterior neck muscles elicits an apparent head motion and move met of the visual target to the contralateral side [7,8].
They also described that the local anesthesia of upper cervical roots and muscles causes somato sensory cervical tone imbalance, leading to light headedness, ataxia, and past pointing in humans and falls, rolling over, and ataxia in animals
Local anesthesia of deep poster lateral neck tissues in humans usually causes a transient increased ipsilateral and decreased contralateral extensor muscle tone with a tendency to fall. And a deviation of gait and past-pointing towards the injected side [1,9].0
Somato sensory cervical input from the neck converges with vestibular input to mediate multisensory control of orientation, gaze in space, and posture. Therefore, the clinical syndrome of cervical vertigo due to altered upper cervical somato sensory input should include the perceptual symptoms of disorientation, ocular motor signs, and postural Imbalance [1]. All these symptoms, in the form of disorientation, ataxic gait or swaying, oscillopsia on walking and turning the car on round abouts, and quickly turning the neck to the left, were present in our patient.
This causes a mismatch, and thus the symptoms of cervical vertigo are expected to be maximum when the mismatch is maximum, i.e., during active head movements, when expected and actual reafferent input do not match [1]. This was clearly stated by our patient as quick spins and oscillopsia on turning the head to the left, especially, and we know that the head rotations occur mainly at C1-C2 joint [1].
Cervical vertigo is characterized by ataxia and unsteadiness of gait, not by a clear rotational or linear vertigo, as stated by Brandt et al [1]. This was clearly evident in our patient. Papa et al stated that cervical vertigo manifests a sim balance, light-headedness, unsteadiness, the illusion of movement, spinning, or whirling, as seen in this patient.
In practice, most cases of vertigo are falsely labelled as being of cervical origin, even if the patient does not have the signs and symptoms of cervical spondylitis. In our opinion, it is of the utmost importance to have some definite findings to label the vertigo as of cervical origin, as in our case. Such cases, however, are extremely rare, and the majority of cases are labelled as cervical vertigo merely on the basis of an osteophyte in the cervical region. It is important that any case of vertigo that does not present with typical symptoms or signs of a particular disease, e.g., BPPV, undergoes relevant imaging. To the best of our knowledge, this is the first case of vertigo due to an isolated atlanto-occipital joint effusion. There has been a case of migraine with atlanto-occipital joint effusion, but it did not have any signs or symptoms of vertigo [12].
Declarations
Declaration of interest: The authors hereby declare that they have no conflict of interest.
Funding statement: This is to certify that the study is not funded by any organization.
References
- Brandt Thomas VERTIGO-its multisensory syndromes 2nd edition, 2: 441-451.
- Mergner T, Siebold C, Schweigart G, et al. Human perception of horizontal trunk and head rotation in space during vestibular and neck stimulation. Exp Brain Res. 1991; 85: 389–404.
- Cooper S, Daniel PM. Muscle spindles in man; their morphology in lumbricals and the deep muscles of neck. Brain. 1963; 86: 563-586.
- Ukuda T. Studies on human dynamic postures from the view point of postural reflexes. Acta Otolaryngol Suppl. 1961; 161:1-52.
- Peterson BW, Goldberg J, Bilotto G, Fuller JH. Cervicocollic reflex: Its dynamic properties and interaction with vestibular reflexes. J Neurophysiol. 1985; 54: 90- 109.
- Wilson VJ, Boyle R, Fukushima K, Rose PK, Shinoda Y, Sugiuchi Y, Uchino Y, et al. The vestibulocollic reflex. J Vestib Res. 1995; 5:147-170.
- Janet L Taylor, D I Mccloskey, et al. Illusions of head & visual target displacement induced by vibration of neckmuscles, Brain.1991; 114: 755–759.
- Biguer B, Donaldson IM, HeinA, Jeannerod M. Neckmus clevibration modifies the representation of visual motion and direction in man. Brain. 1988; 111: 1405-1424.
- DeJong PT, DeJong JM, Cohen B, Jongkees LB. Ataxia and nystagmus induced by injection of local anesthetics in the Neck. Ann Neurol. 1977; 1: 240-246.
- Papa L, Amodio A, Biffi F, Mandara A. Impact of osteopathic therapy on proprioceptive balance and quality of lifein patients with dizziness. J Body Mov Ther. 2017; 21: 866–872.
- Chu ECP, ChinWL, Bhaumik A. Cervicogenic dizziness. Oxf Med Case Reports. 2019; 2019: 476-478.
- Dusko Kozic, Mladen Bjelan,Vesna Njagulj, Milos Lucic, Marjia Semnic, Sne zana Cupara. Isolated Inflammatory Arthritis of the Atlanto occipital Joint Confused with Migraine. The Journal of Rheumatology. 2013; 40: 2097-2098.