
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Combined hepatocellular and cholangiocarcinoma: A rare pathological diagnosis, clinically mimicking its parent phenotypes
Arunima Ghosh; Indra Jeet Gupta*; Shally Batham; MLB Bhatt; Rajeev Gupta
Department of Radiotherapy, King George’s Medical University, Lucknow, Uttar Pradesh, 226003, India.
*Corresponding Author : Indra Jeet Gupta
Department of Radiotherapy, King George’s Medical University Lucknow, Uttar Pradesh, 226003, India.
Email: drindrajeetgupta@gmail.com
Received : Jun 14, 2023
Accepted : Jul 05, 2023
Published : Jul 12, 2023
Archived : www.jcimcr.org
Copyright : © Indra JG (2023).
Abstract
A middle-aged female presented with vague abdominal symptoms that after diagnostic and staging work up was revealed to be an advanced case of combined hepatocellular and cholangiocarcinoma (cHCC-CCA). She was started on systemic chemotherapy inspite of which experienced disease progression. cHCC-CCA is a rare histopathalogical entity making it a diagnostic challenge. Treatment for advanced disease is not well established and prognosis is poor.
Keywords: Hepatocellular carcinoma; Cholangiocarcinoma; Rare tumor.
Citation: Arunima G, Indra JG, Shally B, Bhatt MLB, Rajeev G. Combined hepatocellular and cholangiocarcinoma: A rare pathological diagnosis, clinically mimicking its parent phenotypes. J Clin Images Med Case Rep. 2023; 4(7): 2495.
Introduction
Cholangiocarcionomas (CCAs) are classified based on their anatomic location as intrahepatic CCA (iCCA), perihilar CCA or distal CCA. Combined hepatocellular-cholangiocarcinomas (cHCC-CCA), a distinct subtype of hepatic malignancy are rare cancers which account for 1-4.7% of all primary liver cancers [1]. cHCC-CCA It has unequivocal features of both hepatocytic and cholangiocytic differentiation and manifested features of hepatic stem/progenitor cells [2].
Risk factors for cHCC-CCA are ill defined; may include Hepatitis B Virus (HBV) or Hepatitis C Virus (HCV) infection, alcohol consumption, and primary sclerosing cholangitis with male predominance noted in some studies.
Preoperative radiological diagnosis is difficult and biopsy with immunohistochemical examination is needed to confirm diagnosis. Most patients present with symptoms of advanced disease like jaundice, fatigue, fever, abdominal discomfort and distension [3]. Lesions resembling HCCs may show arterial phase hyperenhancement (APHE) with a corresponding washout appearance (i.e. HCC mimickers) whereas lesions resembling ICCs may show gradual APHE in the periphery of tumor [4].
Treatment of choice for patients with limited disease is hepatic resection with hilar lymph node (LN) dissection as LN metastases are found in over 70% patients. There’s limited literature available to guide clinicians on systemic management of this disease as patients usually present in advanced stages when the disease is inoperable [3].
Case presentation
A middle aged premenopausal female presented with complains of indigestion and vague upper abdominal pain since 4 months. There was no history of alcohol or drug use or any high-risk behavior.
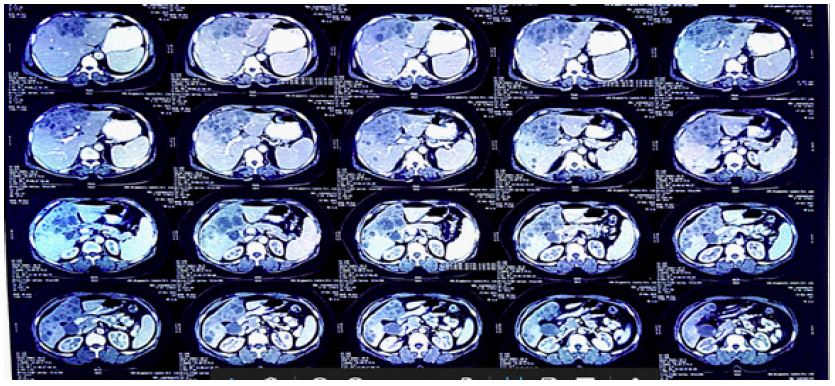
Initial ultrasound of abdomen revealed a 118 x 67 x 99 mm ill-defined heterogeneous, hypoechoic mass in left lobe of liver with few satellite nodular lesions in both liver lobes. The gall bladder lumen was distended, filled with multiple calculi. Abdominal CT scan revealed borderline hepatomegaly with fatty infiltration of liver with ill-defined heterogeneously enhancing 11 x 7 cm lesion involving segments IV and VIII of right lobe of liver. Multiple satellite lesions were noted in liver along with enlarged periportal LN. Enhancing soft tissue lesions were seen in anterior and posterior walls of gall bladder along with cholelithiasis (Figure 1).

Microscopic examination of ultrasound-guided biopsy of liver mass revealed a malignant carcinoma infiltrating the liver parenchyma. On immunohistochemistry studies, the hepatocellular component stained positive for CK19, Arginase, Heppar1 whereas the cholangiocarcinoma component stained positive for CK19, Arginase, CK7, Berep4, Claudin, Glypican (Figure 2). Both components were negative for PAX8, WT1, CK20, CEA. The final diagnosis was Combined Hepatocellular and Cholangiocarcinoma.
18F-FDG PET-CT showed multiple, FDG avid predominantly hypodense lesions in liver, largest conglomerated mass of size 7.5 x 10 cm involving segment IV, V and VIII of liver (SUV max 18.37). The gall bladder was distended and showed multiple soft tissue lesions adherent to its anterior and posterior wall (SUV max 7.8). Few FDG avid periportal LN along with multiple deposits in the omentum and mesentery were noted.
Patient’s blood work revealed normal counts and serum chemistries including liver function tests. Serum alpha fetoprotein was raised to 233 IU/ml, serum CA 19.9 was 15958 U/ml,
serum CA 125 was 15.20 U/ml and serum CEA was 0.65 ng/ml. Lab tests ruled out any viral infections
Patient underwent six cycles systemic chemotherapy with gemcitabine and cisplatin post which a triple phase CT scan of abdomen showed an exophytic soft tissue lesion in fundal region in posterior wall of gall bladder and gross hepatomegaly with multiple lesions in both lobes of liver.
As disease was progressive, patient was then given two cycles of gemcitabine and oxaliplatin.
A month later, patient presented with abdominal distension. Abdominal ultrasound showed progressive disease hepatobiliary disease along with a 53 x 58 mm mass lesion seen in right adnexal region. Left ovary was bulky with an eccentric solid nodular lesion of 30 x 29 mm in size. There was diffuse omental thickening with nodularity. Moderate free fluid was present in peritoneal cavity.
Patient underwent therapeutic and diagnostic ascitic tapping. About two litres of ascitic fluid was drained and sent for examination which showed malignant cells.
In view of non-responsiveness of disease to treatment, patient was started on best supportive care and died a few weeks later.
Discussion
The diagnosis of cHCC-CCA is challenging for clinicians, radiologists and pathologists. Moeini et al confirmed that cHCC-CCAs represent a heterogeneous group of tumors ranging from a more stem-cell like type characterized by features of poor prognosis to a classical type with common lineage of HCC and ICC components [2].
Immunohistochemical markers are needed to confirm distinction between iCCA and HCC. Immunohistochemical markers that are indicative of hepatocellular differentiation include HepPar-1 (hepatocyte in paraffin 1), Arginase-1, Alpha-Fetoprotein (AFP), pCEA (canalicular) and CD10 (canalicular). Markers indicative of biliary differentiation include CK7, CK19 and Epithelial Membrane Antigen (EMA) [5]. Histological mimickers of iCCA include intrahepatic metastases from other primary tumours, such as gastric or pancreatic carcinomas and inflammatory diseases like IgG4-associated cholangitis [6].
Non-surgical treatments are not well discussed in literature. cHCC-CCAs are less vascular and much more fibrotic than HCC, thus less likely to respond to non-surgical treatment options like Transarterial chemoembolisation (TACE) and Percutaneous Ethanol Injection (PEI) [3]. Few case reports have suggested use of combinations of chemotherapy agents like cisplatin, gemcitabine, 5-fluorouracil and doxorubicin [7].
Some studies have shown poorer survival of patients with cHCC-CCA compared to that of HCC or CC patients with median survival of cHCC-CCA 7.9 months vs. 10.8 months for HCC and 8.2 months for ICC. Lymphovascular invasion and presence of satellite metastases are predictors of poor surgical outcome. Inoperable patients have poor survival, usually less than 2 years [8]. Intrahepatic bile duct dilatation, increased CA19.9 levels and an increased Child Pugh score are related to poor prognosis and early death in these patients [9]. It remains unclear whether conventional treatments for HCCs, including surgical resection, liver transplantation, locoregional therapy, or systematic agents, can also be used as treatments for cHCC-CCA.
Our patient had advanced disease at diagnosis and being surgically unresectable was started on chemotherapy. She experienced disease progression even on second line chemotherapy and eventually succumbed to her disease.
Further studies are needed to investigate appropriate treatment plan in patients with advanced cHCC-CCA, the role of biological markers and targeted therapy.
References
- Kim TH, Kim H, Joo I, Lee JM. Combined Hepatocellular-Cholangiocarcinoma: Changes in the 2019 World Health Organization Histological Classification System and Potential Impact on Imaging-Based Diagnosis. Korean J Radiol. 2020; 21: 1115-1125.
- Moeini A, Sia D, Zhang Z, Camprecios G, Stueck A, et al. Mixed hepatocellular cholangiocarcinoma tumors: Cholangiolocellular carcinoma is a distinct molecular entity. J Hepatol. 2017; 66: 952-961
- Kassahun WT, Hauss J. Management of combined hepatocellular and cholangiocarcinoma. Int J Clin Pract. 2008; 62: 1271-1278.
- Honda H, Ochiai K, Adachi E, Yasumori K, Hayashi T, et al. Hepatocellular carcinoma: Correlation of CT, angiographic, and histopathologic findings. Radiology. 1993; 189: 857-862.
- Brunt E, Aishima S, Clavien PA, Fowler K, Goodman Z, et al. cHCC-CCA: Consensus terminology for primary liver carcinomas with both hepatocytic and cholangiocytic differentation. Hepatology. 2018; 68: 113-126.
- Kendall T, Verheij J, Gaudio E, Evert M, Guido M, et al. Anatomical, histomorphological and molecular classification of cholangiocarcinoma. Liver Int. 2019; 39: 7-18.
- Kim JH, Lee YG, Lee J, Jung CK, Kim HT, et al. [A case of combined hepatocellular-cholangiocarcinoma with sarcomatous transformation and second primary colon cancer]. Korean J Hepatol. 2004; 10: 142-147.
- Jarnagin WR, Weber S, Tickoo SK, Koea JB, Obiekwe S, et al. Combined hepatocellular and cholangiocarcinoma: Demographic, clinical, and prognostic factors. Cancer. 2002; 94: 2040-2046.
- Lee JH, Chung GE, Yu SJ, Hwang SY, Kim JS, Kim HY, et al. Long-term prognosis of combined hepatocellular and cholangiocarcinoma after curative resection comparison with hepatocellular carcinoma and cholangiocarcinoma. J Clin Gastroenterol. 2011; 45: 69-75.