
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Imaging in a rare case of neonatal arterial tortuosity syndrome
MC Inserra1*; A Di Mari2; G Passaniti3; MT Cannizzaro1; G La Rosa4; D Poli5; P Gitto5; L Patane6; P Romeo7
1CAST Radiology Department, A.U.O. Policlinico “G.Rodolico-San Marco”, Via S. Sofia 78, 95123 Catania, Italy.
2Department of Medical Surgical Sciences and Advanced Technologies “GF Ingrassia”, University Hospital Policlinico “G. Rodolico-San Marco”, Catania, Italy.
3Division of Cardiology, A.O.U. Policlinico “G. Rodolico - San Marco”, Catania, Italy.
4Department of Medical Surgical Sciences and Advanced Technologies “GF Ingrassia”, University Hospital Policlinico “G. Rodolico-San Marco”, Catania, Italy.
5CCPM-Centro Cardiologico Pediatrico del Mediterraneo “Bambino Gesù” di Taormina, Italy.
6Innovation, Medical Imaging, Science, Robotics, Artificial Intelligence and Business Management.
7Radiology Department of AO “San Marco”, A.U.O. Policlinico “G.Rodolico-San Marco”, Catania, Italy.
*Corresponding Author : Maria Cristina Inserra
CAST Radiology Department, A.U.O. Policlinico “G.Rodolico-San Marco”, Via S. Sofia 78, 95123 Catania, Italy. Tel: 3928433562
Email: c.inserra@yahoo.it
Received : Jun 19, 2023
Accepted : Jul 05, 2023
Published : Jul 12, 2023
Archived : www.jcimcr.org
Copyright : © Inserra MC (2023).
Abstract
Arterial Tortuosity Syndrome (ATS) is a very rare autosomal recessive disorder, that affects the connective tissue. The incidence of ATS is not well known and to date only 106 patients have been described in literature.
ATS affects medium and large sizes arteries, leading to a widespread elongation and to an intensification of the average vessel tortuousness, responsible of several loops and kinks.
As other connective tissue disorders, ATS can present with joint laxity, hernias, pectus excavatum, scoliosis or other muscle-skeletal abnormalities and ocular defects.
Due to the extreme variability of clinical symptoms and to the fact that ATS has no curative management, prompt diagnosis is of tremendous importance, to primary prevent disease’s associated complications. In this situation, imaging techniques have a central role.
We describe a rare case of a male newborn with tortuosity and lengthening of the main arterial and venous medium and large caliber branches with associated aortic coarctation that passed away prematurely. In newborn with ATS, the finding of aortic Coarctation (CoA) has rarely been described in literature.
Keywords: Arterial tortuosity syndrome; SLC2A10; Coarctation of the aorta; Connective tissue disorder; Aortic elongation sign.
Citation: Inserra MC, Di Mari A, Passaniti G, Cannizzaro MT, La Rosa G, et al. Imaging in a rare case of neonatal arterial tortuosity syndrome. J Clin Images Med Case Rep. 2023; 4(7): 2496.
Introduction
ATS (OMIM 208050) is a very rare autosomal recessive disorder, that affects the connective tissue, which was first described in 1967 by Ertugrul [1].
The incidence of ATS is not well known and, to date, only 106 patients have been described in literature, but its incidence is supposed to be even higher due to the very large and difficult to identify manifestation spectrum [2]. ATS is related to the mutation of gene SLC2A10 (chromosome 20q13.2), which encodes for the glucose transporter GLUT10. The exact role of GLUT10 in the pathogenesis of the disorder remains to be fully clarified. Previous evidence revealed that GLUT10 acts as an intracellular transporter of dehydroascorbic acid, that functions as a hydroxylation cofactor for prolyl and lysyl residues, which is crucial for elastin and collagen maturation [3]. Additionally, GLUT-10 deficiency alters the canonical pathway of transforming growth factor beta (TGF-beta), involved in the disorganization of different proteins of the extracellular matrix, which are essential for the structural integrity of different connective tissues, including the walls of blood vessels [2].
Specifically, ATS affects medium and large sizes arteries, leading to a widespread elongation and to an intensification of the average vessel tortuousness, responsible of several loops and kinks, with a predisposition to dissection and aneurysms. Evidence of CoA in association with ATS is a condition rarely found with only a few cases described in the literature [4,5].
It is necessary to suspect ATS in newborns that present with typical facial features (micrognatia, convex nasal ridge, hypertelorism, high palate), musculoskeletal alterations joint laxity (76%), hernias, pectus excavatum (28%), scoliosis or other muscle-skeletal abnormalities and ocular defects, especially if, after imaging examination, an increased vascular tortuosity is evidenced [5,6].
The main cardiovascular findings reported in literature are aortic tortuosity (92%), tortuosity of other arteries (80%), aortic root aneurysm (16%), pulmonary artery stenosis (57%), focal stenosis of the aorta (24%), autonomic dysfunction (18%), aortic and arterial aneurysms, stenosis of the aortic valve and pulmonary arteries and ischemic or hemorrhagic events [5].
Due to the generalized abnormalities caused by ATS, early diagnosis is of fundamental importance, in order to try to prevent life-threatening complications.
However, diagnostic criteria are still not well established. Therefore, the diagnostic pathway begins with a strong clinical suspect, continues with advanced imaging multimodality techniques (radiography, echocardiography, Computed Tomography Angiography (CTA) evaluation and/or Magnetic Resonance (MRI) angiography) and ends with the genetic research of SLC2A10 mutation.
We describe the rare case of a newborn with typical facial features, increased skin folds, showing typical imaging results of ATS in CTA with aortic coarctation that died about two month and 15 days from birth due to severe picture of diffuse ischemia.
Case presentation
We present the case of a male infant, born at 37 weeks of gestation (W.G) by urgent cesarean section for growth arrest.
His birth weight was 2,250 g (3th percentile), length 47 cm (10th percentile), and occipitofrontal circumference (OFC) 34 cm (3th percentile).
Family history was unremarkable. He was first child to healthy non-consanguineous parents originating from southern Italy.
Patient’s prenatal echocardiographic study showed evidence of complex congenital heart disease.
At birth he was hemodynamically stable and in spontaneous breathing and he was admitted to the Neonatal Cardiologic Intensive Care at birth for further investigations and appropriate treatment.
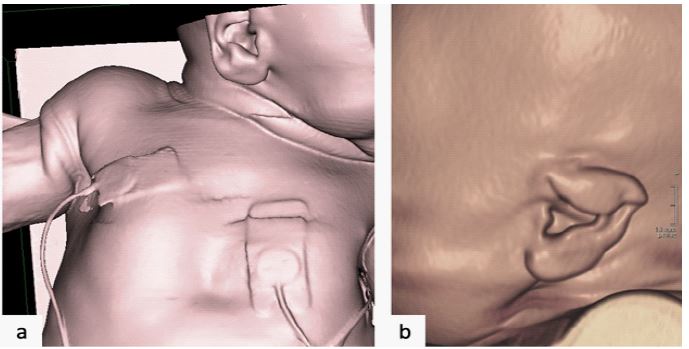
On physical examination, the newborn presented dysmorphic facial features (wide folded ears and narrow maxilla), increased skin plication, acrocyanosis, minimal chest excavation, joint hypermobility (Figure 1), hands pronated and flexed, feet twisted.
The cardiac auscultation displayed a continuous murmur (systolic-diastolic murmur) due to Patent Ductus Arteriosus (PDA).
Transthoracic Echocardiogram (TTE) was performed and showed tortuosity at the origins of the great vessels that appeared elongated, with ill-defined course, patent foramen ovale with bidirectional shunt, no left or right ventricular outflow tract obstruction, mitral valve dysplasia with mild regurgitation and mild aortic regurgitation, left ventricular hypertrophy, pulmonary branches with Crossed Pulmonary Arteries (CPAs), without stenosis on the trunk or branches and PDA.
Aortic arch demonstrates reduced caliber in its extremely tortuous course with evidence of significant turbulence on Doppler and increased caliber of ascending aorta.
In view of these findings, at fourth day of life day of life a Multidetector Computed Tomography (MDCT) angiography examination was performed with a multi-detector CT (GE Lightspeed Plus 16-Slice) and Multiplanar Reconstruction (MPR), Maximal Intensity Projection (MIP) and three-dimensional (3D volume rendering-VR- and surface rendering-SR) reconstructions were done.
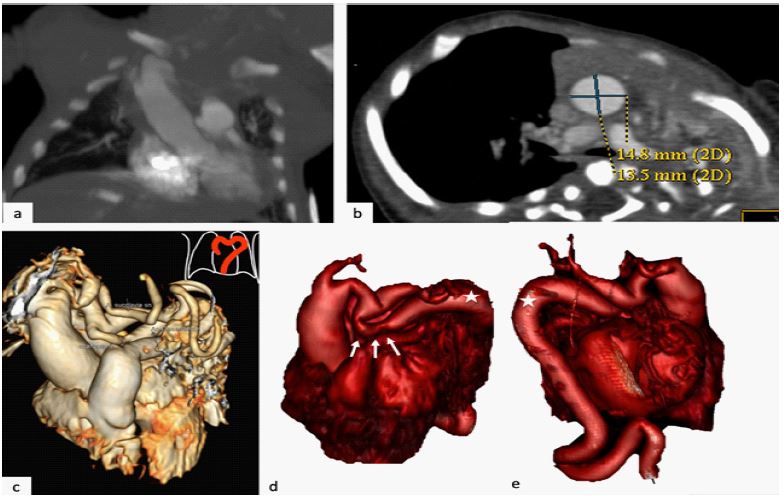
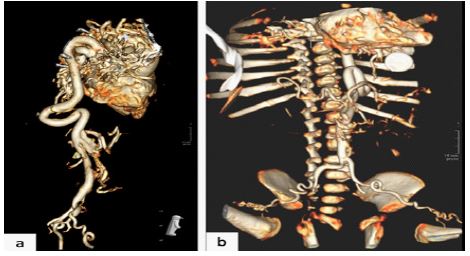
The CT scan revealed widespread tortuosity, kinking, looping, coiling and elongation of arterial and venous tree; we found an ascending aorta of augmented caliber, 14.8 mm x 13.5 mm (Z score + 5.08) and also elongated (Figure 2); aortic arch appeared elongated, with an irregular path (located higher and to the right than normal and with quadrangular morphology) (Figure 2).
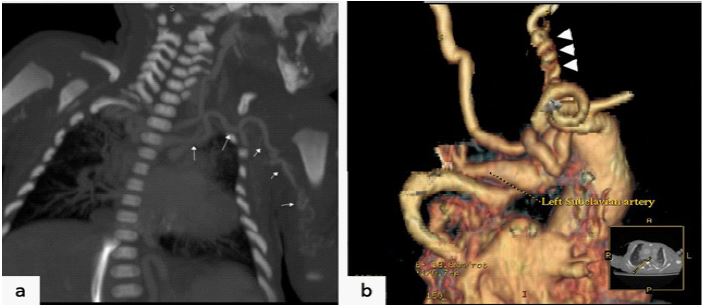
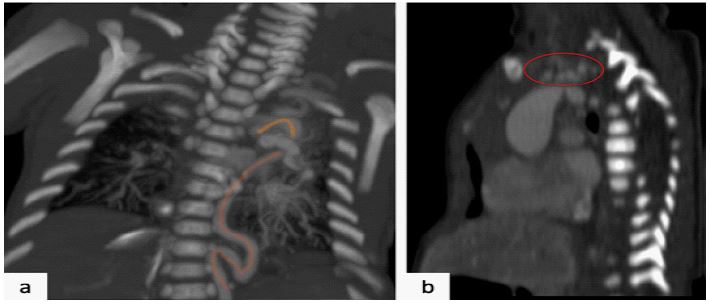
Origin of the supra-aortic trunks were normal, but these vessels appeared extremely elongated and tortuous, especially the subclavian arteries and the carotid arteries, that showed a “corkscrew appearance” in proximal and medium portions (Figure 3), with focal and multiple narrowing and widening and with progressive increase of tortuosity to the control CTs. Descending aorta displayed to be coarctated, with abrupt narrowing at the isthmus, extended for about 2 cm (Figure 2). The proximal descending aorta also appeared with altered course, longer than normal and lateralized (Figure 4), with tendency to extend to the left hemithorax (about 3 cm from the vertebral soma in the context of the rib cage) resulting in bronchial compression and lung collapse (Figure 5); It also presented right-sided kink near the diaphragmatic hiatus (Figure 3).
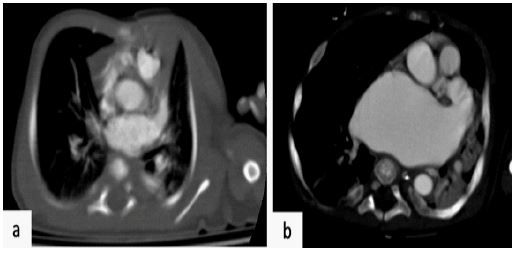
Main pulmonary artery appeared to be of a regular caliber (Z score + 0,95) with early bifurcation (inverted V shape configuration at the axial CT scan) and relative elongation and narrowing of right and left pulmonary arteries; left pulmonary artery presents mid distal narrowing followed by ectasia of the branch itself; hyper-arborized the distal circles of both the pulmonary arterial district (in the sub hilar site) (Figure 6).
The remaining arteries and venous vessels of the medium and small caliber also appeared tortuous especially the femoral arteries bilaterally with corkscrew appearance.
Circumscribed image of plausible diaphragmatic laxity in paracaval site welcoming share of adipose is also appreciated.
In relation to the angio CT findings, suspicion of ATS was placed and clinical instrumental monitoring of right sup limb and lower limb PA and SpO2 was performed every 4 h.
Initial DNA analysis was performed from DNA extracted from peripheral blood samples from the child, array Comparative Genomic Hybridization (CGH) was carried out to excluded Ehlers-Danlos syndrome, based on the negative finding, the exons and intronic flanking regions of SLC2A10 gene were amplified and direct sequencing was performed and confirmed the diagnosis of ATS. Therefore, heparins therapy was started.
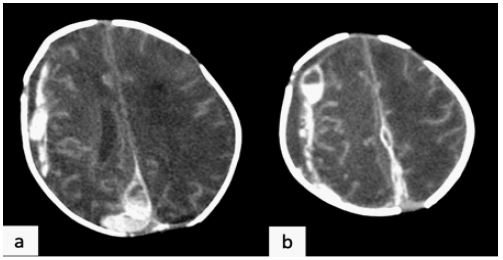
Subsequently, as of day 17 from birth, two CT scans were performed during the follow-up and following the detection of delayed neurological development of the child and a worsening of clinical symptoms. CT images showed a progressive increase in vessel tortuosity, encephalic ischemia (Figure 8) and marked left atrial dilation (Figure 9).
The newborn died about two month and 15 days from birth for severe picture of diffuse ischemia.


Discussion
ATS is considered rare (< 1:1,000,000 live births) autosomal recessive genetic disease; with and an M/F ratio of 1:1 [2].
First authors that described this syndrome named it “Ehlers-Danlos syndrome with multiple pulmonary artery stenoses and tortuous systemic arteries.”, underlying the similarity between these two conditions, such a pathology in fact enters in differential diagnosis with different connective diseases, for the very similar vascular, connective tissue changes and clinical presentation like Marfan syndrome, Williams Beuren syndrome, Ehlers Danlos syndrome, hereditary cutis laxa syndromes, Loeys-Dietz Syndrome (LDS), and lethal syndromic vasculopathy associated with a novel mutation in FBLN4; the latter are associated with greater vascular involvement [2,3].
Evidence of marked vascular tortuosity should prompt a search, species in newborn or young subjects, underlying inherited arteriopathies; in this case is crucial to know and recognize other specific findings associated with each of these conditions and subsequently perform a targeted genetic analysis for final confirmation, with possible substantial impact for the patient and its family.
Imaging is of fundamental importance as it allows us to make a diagnosis, to evaluate the onset of complications and to complete a preoperative assessment, as often such subjects need to undergo surgery. Two different quantitative methods exist for measuring arterial tortuosity. The most widely used is Tortuosity Index (TI) defined as the percent ratio of calculated shortest distance between the end points divided by actual length of the arterial segment considered. Fundamental for the radiologist to describe the vascular anatomy, providing the index of tortuosity and a quantitative evaluation of aneurysms dilations (Z score and Aortic ratio) that allows to have a quantitative evaluation of the data found, early identification of cases of non-manifest tortuosity, screening of family members; it also enables for better communication between the different specialists [6,7].
In his study, Venkatraman Bhat describes the spectrum of features of ATS, identified by common imaging modalities (chest X-ray, echocardiography, CTA and MRI imaging) that can help in the recognition of such a pathological condition and that we have highlighted in our case [8].
A “aortic elongation sign” at Antero-Posterior (AP) chest radiography with elongation of aorta leading to prominent aortic knuckle can be observed in a young patient, “meandering vessel sign” (Figure 4), evident at Coronal CT or A-P chest radiography with tortuous arteries coursing beyond the normal distribution, extending to adjacent anatomical areas, ”cluster of vessels sign” (Figure 4), expressed tortuosity of origins of great arteries leading to cluster of vessels on cross section at C T sagittal/axial images, “V” sign of pulmonary bifurcation (at Coronal CT ) or Inverted “ V sign “ of pulmonary bifurcation at Axial CT expressed early bifurcation of pulmonary arteries, often with narrowing of origin [8].
Awareness of early sign of arterial tortuosity and recognition of the described marks lead to early diagnosis of clinically asymptomatic cases of ATS. In this context, MDCT evaluation appears to be the best choice in the investigation of ATS patients.
Evidence of CoA in patients with aortic ATS is a rare condition described in literature in only one adult patient [9]. It is important to identify and describe why it could benefit of surgical treatment in selected patients. In our case, the patient presented coarctation of the descending aorta, with abrupt narrowing to the isthmus, extended to about 2 cm, which led to a progressive increase in blood pressure in the heart chambers of the left and progressive expansion of the left atrium.
Mortality was originally estimated at 40% before age 5 [10]. However, subsequent studies suggest lower death rates [11]. Still, the prognosis may be severe. The major causes of death are respiratory failure, ventricular hypertrophy resulting in generalized heart failure, myocarditis and ischemic events. In our case, the patient had a progressive clinical deterioration with the development of pulmonary hypertension, electrocardiographic alterations consequential to the progressive atrial dilation and subsequent ischemic events that led to early death.
Conclusion
Arterial tortuosity syndrome with CoA is a very rare condition. It is crucial to maintain high diagnostic suspicion because of overlap with other connective tissue disorders.
Imaging plays a central role in the diagnosis and detection of complications. Radiologists should be aware of the imaging features of ATS as for timely diagnosis. If high vascular tortuosity is found, it is critical to suspect an underlying genetic disorder. Consequently, the use of the tortuosity index helps to provide a quantitative figure for this parameter. Radiologists must be familiar with the imaging features of ATS for a prompt diagnosis.
Declarations
Authors’ contributions: Each author committed a substantial contribution to the conception or design of the work and to revise it critically for important intellectual content. In addition, each author approved the final version to be published. Conversely, each author agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ethical approval: All patients (or their relatives/legal guardians) have freely provided written consent for their images to be published and shared for scientific purposes.
Conflict of interest: None declared.
References
- Ertugrul A. Diffuse tortuosity and lengthening of the arteries. Circulation. 1967; 36: 400-407.
- Callewaert B, De Paepe A, Coucke P. Arterial Tortuosity Syndrome. Adam MP, Mirzaa GM, Pagon RA, et al., editors. In: Gene Reviews®. Seattle (WA): University of Washington, Seattle. 2014; 1993-2023.
- Lee YC, Huang HY, Chang CJ, Cheng CH, Chen YT. Mitochondrial GLUT10 facilitates dehydroascorbic acid import and protects cells against oxidative stress: Mechanistic insight into arterial tortuosity syndrome. Hum Mol Genet. 2010; 19: 3721-3733.
- Asafu Adjaye Frimpong G, Aboagye E, Tannor EK, Chigbu NCC, Daboner VT. Coarctation of the Aorta with Arterial Tortuosity Syndrome - A Case Report with Cinematic Rendering. Int Med Case Rep J. 2022; 15: 349-354.
- Beyens A, Albuisson J, Boel A, Al-Essa M, Al-Manea W, et al. Arterial tortuosity syndrome: 40 new families and literature review. Genet Med. 2018; 20: 1236-1245.
- Farkas A, Steiner M, Giles H, Miller K. Arterial tortuosity syndrome: An extremely rare disease presenting as a mimic of pulmonary sling. Radiol Case Rep. 2017; 13: 295-298.
- Ciurica S, Lopez-Sublet M, Loeys BL, Radhouani I, Natarajan N, et al. Arterial Tortuosity. Hypertension. 2019; 73: 951-960.
- Bhat V. Arterial Tortuosity Syndrome: An Approach through Imaging Perspective. J Clin Imaging Sci. 2014; 4: 44.
- Asafu Adjaye Frimpong G, Aboagye E, Tannor EK, Chigbu NCC, Daboner VT. Coarctation of the Aorta with Arterial Tortuosity Syndrome-A Case Report with Cinematic Rendering. Int Med Case Rep J. 2022; 15: 349-354.
- Wessels MW, Catsman-Berrevoets CE, Mancini GM, Breuning MH, Hoogeboom JJM, et al. Three new families with arterial tortuosity syndrome. Am J Med Genet A. 2004; 131: 134-143.
- Callewaert BL, Willaert A, Kerstjens-Frederikse WS, De Backer J, Devriendt K, et al. Arterial tortuosity syndrome: clinical and molecular findings in 12 newly identified families. Hum Mutat. 2008; 29: 150-158.