
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Blood and bile: A gastroduodenal artery pseudoaneurysm associated with endoscopic retrograde cholangiopancreatography stent migration
P Ramaraj*; D Veeramootoo; HD De’Ath
Department of Frimley Health NHS Foundation Trust Portsmouth Road, Frimley, Surrey GU16 7UJ, UK.
*Corresponding Author : Prashanth Ramaraj
Department of Frimley Health NHS Foundation Trust Portsmouth Road, Frimley, Surrey GU16 7UJ, UK.
Email: prashanth.ramaraj@nhs.net
Received : Jun 19, 2023
Accepted : Jul 06, 2023
Published : Jul 13, 2023
Archived : www.jcimcr.org
Copyright : © Ramaraj P (2023).
Citation: Ramaraj P, Veeramootoo D, De’Ath HD. Blood and bile: A gastroduodenal artery pseudoaneurysm associated with endoscopic retrograde cholangiopancreatography stent migration. J Clin Images Med Case Rep. 2023; 4(7): 2497.
Description
A man in his mid-forties presented with a two-day history of sudden onset right upper quadrant pain and coffee-ground vomiting. Eight months previously, he underwent successful endoscopic retrograde cholangiopancreatography (ERCP) with biliary stenting for cholangitis and severe gallstone pancreatitis. This was followed by a COVID-delayed uncomplicated laparoscopic cholecystectomy.
On examination, positive findings were tenderness in the epigastrium and melaena. His observations included a blood pressure of 144/101 mmHg, pulse 121 bpm, respiration rate 28/minute, oxygen saturations of 96% on room air and a temperature of 38.2oC. Blood results showed a normal haemoglobin (131 g/L) and alkaline phosphatase (95 IU/L with a raised white cell count (14.2 x 109/L), C-reactive protein (67 mg/L), bilirubin (40 μmol/L), and alanine transaminase (193 IU/L). The working diagnosis was cholangitis with possible upper GI bleeding, so he was started on intravenous antibiotics and a proton-pump inhibitor.
Urgent upper GI endoscopy initially revealed no source of bleeding, with the biliary stent correctly positioned. Abdominal ultrasound scan demonstrated no aerobilia suggestive of stent malfunction, therefore an expedited ERCP was planned.
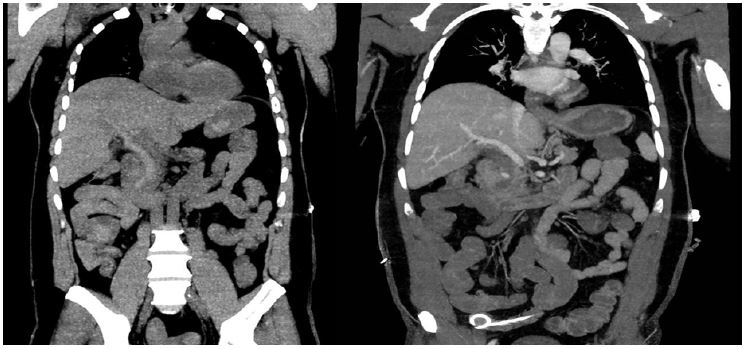
Forty-eight hours after admission, he became suddenly unwell with severe epigastric pain and large volume haematemesis. Due to his haemodynamical instability an urgent computerised tomography angiogram (CTA) was performed (Figure 1).
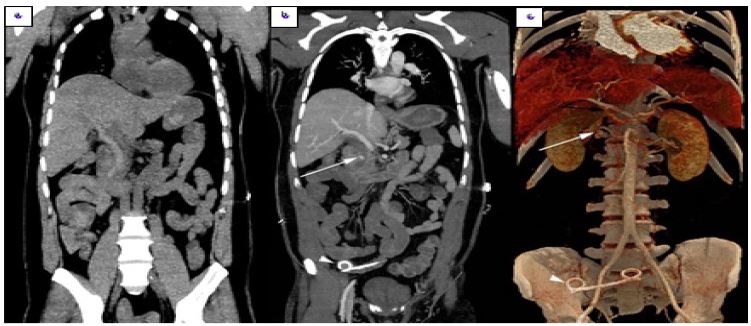
The scan demonstrates evidence of a Gastroduodenal Artery (GDA) pseudoaneurysm rupture into the Common Bile Duct (CBD), leading to blood in the gastrointestinal tract and biliary stent displacement (Figure 2).
GDA pseudoaneurysms are the rarest amongst splanchnic arteries (1.5%), and typically (80%) the result of severe pancreatitis. The risk of rupture is high (75%) and carries a significant mortality rate (21%) [1].
Clinical evidence of GDA pseudoaneurysm rupture into the patient’s CBD was the combination of an upper gastrointestinal (UGI) bleed, abdominal pain, and jaundice, thereby completing Quincke’s triad of haemobilia [2]. All three signs are seen in only 22% of cases. Around 65% of haemobilia is iatrogenic, and most cases present immediately post-procedure (ERCP) [3]. Other causes include gallstones, trauma, biliary varices, hepatitis, and malignancy.
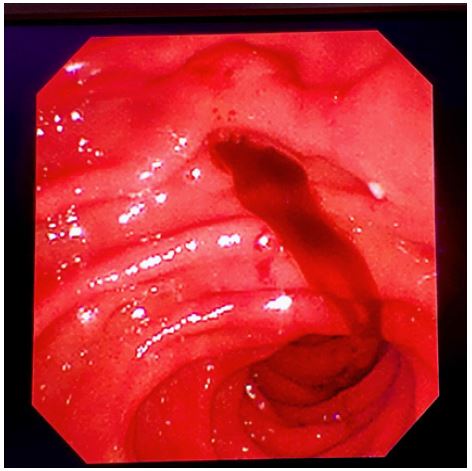
The identification of haemobilia in an UGI bleed includes an OGD demonstrating blood at the ampulla of Vater (Figure 3). CTA is indicated in occult cases. The gold-standard management of GDA pseudoaneurysm rupture is angioembolisation with clinical success rates of 50-80%. Ongoing bleeding requires operative management.
Our patient was resuscitated with blood products and GDA angioembolisation was performed which successfully halted bleeding. He has since remained well and has manifested no further evidence of bleeding. At 30-day and 1 year telephone follow up, there were no concerns.
Declarations
Author contributions: All authors provided and cared for the study patient. Author PR was involved in the data collection, patient consent, literature review, and writing of this manuscript. Authors DV and HD were involved in conception of idea, and the writing and reviewing of the manuscript. All authors fulfil the criteria of authorship per ICMJE Recommendations 2019. There is no one else who fulfils the criteria that has been excluded as an author.
Patient consent and confidentiality: This patient described in this manuscript has provided explicit consent in the form of a signed patient consent form following a consultation.
Funding, data sharing, and conflict of interests: This study is unfunded and there are no conflicts of interests regarding this study. The authors agree to share data related with this study upon reasonable request.
References
- Shanley CJ, Shah NL, Messina LM. Uncommon Splanchnic Artery Aneurysms: Pancreaticoduodenal, Gastroduodenal, Superior Mesenteric, Inferior Mesenteric, and Colic. Ann Vasc Surg. 1996; 10: 506-515.
- Quincke H. Ein Fall von Aneurysma der Leberarterie. Berliner Klin Wochenschrift. 1871; 30: 349-352.
- Green MHA, Duell RM, Johnson CD, Jamieson2 N V. Haemobilia. Br J Surg. 2001; 88: 773-786.