
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Recurrent ischemic stroke due to internal carotid artery dissection
Jing Zheng*; Jing Zuo; Yue Wan
Department of Neurology, Hubei No.3 People’s Hospital of Jianghan University, 26 Zhongshan St, Qiaokou District, Wuhan, 430000, China.
*Corresponding Author : Jing Zheng
Department of Neurology, Hubei No.3 People’s Hospital Of Jianghan University, 26 Zhongshan St, Qiaokou District, Wuhan, 430000, China.
Email: 404212544@qq.com
Received : Jun 16, 2023
Accepted : Jul 06, 2023
Published : Jul 13, 2023
Archived : www.jcimcr.org
Copyright : © Zheng J (2023).
Abstract
A 73-year-old male was admitted to the neurology department complaining of right hemiparesis lasting for 19 hours. At admission, Magnetic Resonance Imaging (MRI) showed acute ischemia in the left cerebral hemisphere, but brain MR angiography and ultrasonography of the carotid artery were unremarkable. Dual antiplatelet therapy was started, but on hospital day 5, he suddenly fallen into lethargy and manifested right paralysis. Emergency digital subtraction angiography revealed severe stenosis in left internal carotid artery and complete embolic occlusion of the left middle cerebral artery, and intracranial thrombectomy was performed to achieve reperfusion. Repeat ultrasonography of the carotid artery detected findings of a double-lumen and intimal flap, which were thought to be a dissection. Elective stenting of the dissected carotid artery with 2 overlapping stents was performed 14 days later.
Abbreviations: MRI: Magnetic Resonance Imaging; MRA: Magnetic Resonance Angiography; DSA: Digital Subtraction Angiography; CTA: Computed Tomography Angiography; CT: Computed Tomography.
Citation: Zheng J, Zuo J, Wan Y. Recurrent ischemic stroke due to internal carotid artery dissection. J Clin Images Med Case Rep. 2023; 4(7): 2498.
Introduction
Carotid artery dissection accounts for 2-3% of all ischaemic strokes, but it may account for up to 25% in young strokes [1]. A tear in the intima leads blood leaking into the arterial wall, forming mural hematoma, the hematoma can expand towards the intima causing vessel narrowing, or towards the adventitia resulting in pseudoaneurysm [2]. Embolisation and hemodynamic failure are presumed pathogenesis of dissection strokes, artery-to-artery embolism of a thrombus formed at the dissected nidus is the major mechanism [3], this has been demonstrated by transcranial Dopplor detecting cerebral microembolism in acute carotid artery dissection [3,4]. Most strokes occurred in the first two weeks after dissection, recurrent ischaemic events were rare, the risk was reported to be less than 3% [2]. We report a case of recurrent embolic ischaemic stroke due to cervical carotid artery dissection successfully treated with endovascular thrombectomy.
Case presentation
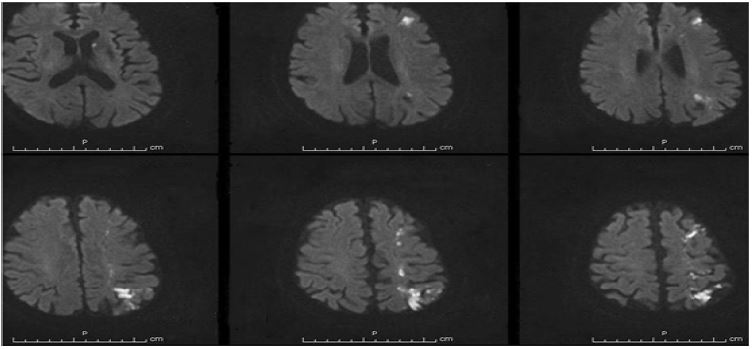
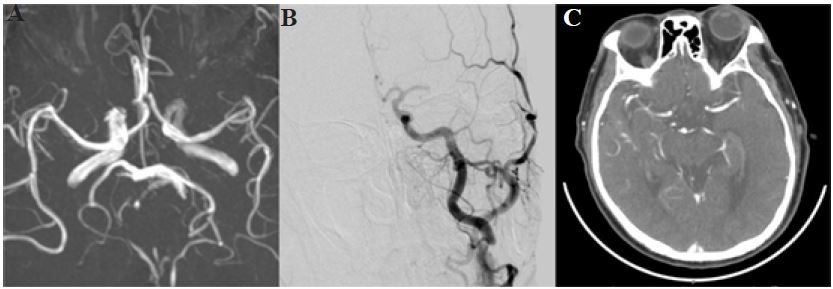
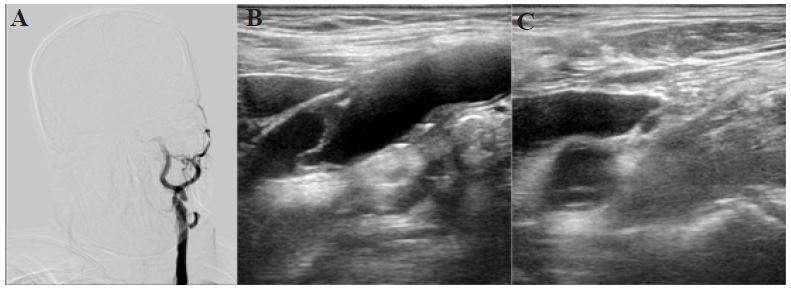
A 73-year-old male with a history of hypertension and diabetes manifesting with right hemiparesis lasting for 19 hours was admitted to the neurology department. He denied head or neck trauma. On admission, diffusion-weighted Magnetic Resonance Imaging (MRI) demonstrated acute ischemia in the left basal ganglion, frontal and parietal cortex in a watershed distribution (Figure 1). Brain Magnetic Resonance Angiography (MRA) and ultrasonography of the carotid artery didn’t show marked narrowing of vessels (Figure 2A). No evidence of cardiac embolism was found by electrocardiograph and transthoracic echocardiography. Dual antiplatelet therapy was started, his right upper extremity weakness deteriorated the next day. Head Computed Tomography (CT) revealed no hemorrhage. Tirofiban was infused and the deterioration of right upper extremity weakness resolved soon. But on hospital day 5, he suddenly fallen into lethargy and developed aphasia, left gaze palsy, and right paralysis. Emergency Digital Subtraction Angiography (DSA) revealed severe stenosis in the cervical segment of the left internal carotid artery (Figure 3A) and complete embolic occlusion of the left middle cerebral artery (Figure 2B), and intracranial thrombectomy was performed to achieve revascularization of the left middle artery, then he was transferred to the neurology intensive care unit. Repeat ultrasonography revealed severe stenosis in the initial segment of the left internal carotid artery with findings of a double-lumen and intimal flap (Figure 3B,3C), which were thought to be a dissection. Post-procedurally, the patient was clear in consciousness and the neurological examination showed hemiparesis of right extremities. Head CT angiography showed complete recanalization of the left middle cerebral artery (Figure 2C). Our patient was anticoagulated with low-molecular-weight heparin and antiplatelet drugs were discontinued. Elective stenting of the dissected carotid artery with 2 overlapping stents was performed to prevent recurrent ischemic stroke.
Outcome and follow-up
His remaining deficit was mild weakness of the right upper extremity at discharge on dual antiplatelet therapy. The follow-up after a year showed no recurrence.
Discussion
Our patient was ultimately diagnosed with ischaemic stroke related to carotid artery dissection, despite treated with antiplatelet drugs, embolic occlusion of the left middle cerebral artery occurred and emergency mechanical thrombectomy was required. The reported sensitivity of ultrasound for diagnosing stroke patients with carotid artery dissection was high, but the sensitivity decreased when the dissection only causing low-grade stenosis [5]. Ultrasound assessment is non-invasive and based on hemodynamic criteria, it’s difficult to differentiate the increased velocity from dissection to another pathological stenosis in a 50% stenosis [6]. We speculated that the hemodynamic compromise was mild and only lead to a low-degree stenosis in the early stage of a dissection, and the situation that the sonographer couldn’t detect high-velocity stenosis signals may result to the false-negative finding in our case. Carotid ultrasound morphologic imaging findings of a double lumen with a vein overlying the artery can be excluded by smooth probe pressure that causes a vein to collapse [5].
Endothelial injury causes platelet aggregation and activation of the coagulation cascade leading to thrombus formation, and antiplatelet drugs inhibiting platelet aggregation or anticoagulation drugs inhibiting coagulation cascade can reduce new thromus formation in the dissected wall [2]. Warfarin-Aspirin Recurrent Stroke Study (WARSS) found no superiority of warfarin over aspirin in preventing recurrent ischaemic stroke [7], but it is more common to use anticoagulation therapy rather than antiplatelet therapy in clinical practice. Most recurrent strokes after dissection are thromboembolic [8], and the sudden neurological deterioration in our case was because of continued embolism arising from the dissected cervical carotid artery.
Though blood flow of the intracranial circulation could be promptly restored after stenting dissected carotid artery without approaching the occluded small middle cerebral artery branch in rare case, but the thrombi narrowed the middle cerebral artery lumen abruptly in our patient, there was no time for intracranial collaterals to be established, the “distal-to-proximal” recanalization approach was adopted to hasten early brain reperfusion and reduce core infarct volume in the tandem occlusions [9]. Emergency stenting for dissected artery in tandem occlusion strokes during endovascular thrombectomy was safe and had high rates of successful reperfusion, but it was not associated with better clinical outcome [10]. The timing and necessity of carotid artery stenting should be considered cautiously, but in patients with severe residual stenosis after intracranial recanalization, insufficient compensation of Willis circle or potential sequential thrombus,carotid artery stent should be performed [10]. Considering successful intracranial reperfusion was achieved and potential risk of intracranial hemorrhage in our patient, mechanical thrombectomy was firstly performed, and elective carotid artery stenting was performed 14 days later.
Learning points
Correct and timely diagnosis of carotid artery dissection is challenging, it is suspected on clinical symptoms and confirmed by neuroimaging techniques. Despite confirmed diagnosis of carotid artery dissection, the management decision should base on individual factors and neuroimaging characteristics. Endovascular therapy has been a promising and emergency option when antithrombotic therapy failed to prevent new ischaemic events.
Declarations
Conflict of interest disclosures: None.
Patient consent for publication: Consent obtained directly from patient.
Ethics approval: Not applicable.
References
- Weimar C, Kraywinkel K, Hagemeister C. German Stroke Study Collaboration. Recurrent stroke after cervical artery dissection. J Neurol Neurosurg Psychiatry. 2010; 81: 869-873.
- Blum CA, Yaghi S. Cervical artery dissection: A review of the epidemiology, pathophysiology, treatment, and outcome. Arch Neurosci. 2015; 2: e26670-82.
- Investigators CT, Peycke J, Willson M. Antiplatelet treatment compared with anticoagulation treatment for Cervical Artery Dissection (CADISS): A randomised trial. Lancet Neurol. 2015; 14: 361-367.
- Molina CA, Alvarez-Sabín J, Schonewille W, Montaner J, Rovira A, et al. Cerebral microembolism in acute spontaneous internal carotid artery dissection. Neurology. 2000; 55: 1738-1740.
- Sturzenegger M, Mattle HP, Rivoir A, Baumgartner RW. Ultrasound findings in carotid artery dissection: analysis of 43 patients. Neurology. 1995; 45: 691-698.
- Benninger DH, Georgiadis D, Gandjour J, Baumgartner RW. Accuracy of color duplex ultrasound diagnosis of spontaneous carotid dissection causing ischemia. Stroke. 2006; 37: 377-381.
- Mohr JP, Thompson JL, Lazar RM. Warfarin-Aspirin Recurrent Stroke Study Group. A comparison of warfarin and aspirin for the prevention of recurrent ischemic stroke. N Engl J Med. 2001; 345: 1444-1451.
- Schievink WI. The treatment of spontaneous carotid and vertebral artery dissections. Curr Opin Cardiol. 2000; 15: 316-321.
- Jensen J, Salottolo K, Frei D. Comprehensive analysis of intra-arterial treatment for acute ischemic stroke due to cervical artery dissection. J Neurointerv Surg. 2017; 9: 654-658.
- Marnat G, Lapergue B, Sibon I. Safety and Outcome of Carotid Dissection Stenting. During the Treatment of Tandem Occlusions: A Pooled Analysis of TITAN and ETIS. Stroke 2020; 51: 3713-3718.