
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Multicystic encephalomalacia following intrauterine single fetal death in second-trimester and subsequent fetofetal transfusion syndrome in monochorionic twin pregnancy: A case report
Bahman Rasuli¹*; Elahe Zaremehrjardi²
1Jame Jam Imaging Center, Tehran University of Medical Sciences, Shahriar, Tehran, Iran.
2Imam Khomeini Hospital, Medical Faculty of Tehran University of Medical Sciences, Tehran, Iran.
*Corresponding Author : Bahman Rasuli
Jame Jam Imaging Center, Tehran University of Medical Sciences, Shahriar, Tehran, Iran.
Email: bahman_rasuli@yahoo.com
Received : Jun 08, 2023
Accepted : Jul 11, 2023
Published : Jul 18, 2023
Archived : www.jcimcr.org
Copyright : © Rasuli B (2023).
Abstract
Background: Multicystic encephalomalacia is a condition of cerebral necrosis followed by the formation of cystic lesions of varying sized starting from the periventricular area and may extending to the cerebral cortex. This disorder may happens in surviving cotwins after the second and third-trimester intrauterine fetal death of one twin in monochorionic pregnancies. We present a case of multicystic encephalomalacia following cotwin’s fetal death in the second trimester diagnosed by sonography and magnetic resonance imaging in a monochorionic twin pregnancy.
Case presentation: A 22-year-old nulliparous woman had an unplanned monochorionic diamniotic twin pregnancy. Two alive fetuses with single placenta were seen at ultrasound anomaly scan with a 3 days discrepancy and weight. Her next perinatal visit was at 29 weeks of gestation, that pregnancy was complicated by fetofetal transfusion syndrome in which discordant amniotic fluid volumes were found. One fetus was demised and the other baby was found to have multicystic encephalomalacia by prenatal ultrasound exam and confirmed by magnetic resonance imaging.
Conclusion: The frequency of neurologic complications in the survivors of monochorionic twin pregnancy after the co-twin death in the second and third trimesters is not clear because of double death. Thus obstetricians should be careful regarding the possibility of hypoxic-ischemic injury and fetofetal transfusion in the survivors. Prenatal ultrasound is a valuable tool for the early finding of intracranial lesions and needs fetal MRI to confirm the brain lesion.
Keywords: Multicystic encephalomalacia; Monochorionic twins; Neurologic damage; Magnetic resonance imaging.
Abbreviations: MCDA: Monochorionic diamniotic; MCE: Multicystic encephalomalacia.
Citation: Rasuli B, Zaremehrjardi E. Multicystic encephalomalacia following intrauterine single fetal death in second-trimester and subsequent fetofetal transfusion syndrome in monochorionic twin pregnancy: a case report. J Clin Images Med Case Rep. 2023; 4(7): 2503.
Background
Multicystic encephalomalacia is characterized by cystic lesions of variable size in the brain parenchyma periventricular area and the probability of development onto the cortex region. The hypoxic or ischemic injury leads to liquefactive necrosis followed by the formation of gliotic cyst walls having an admixture of microglia [1].
Survivors of twin monochorionic pregnancy complicated by the demise of the co-twin and fetofetal transfusion syndrome will show brain injuries. So chorionicity is a crucial determinant factor of fetal outcomes in twin pregnancies. In other words, monochorionic twin pregnancies carry a particularly higher risk of perinatal loss compared with dichorionic pregnancies. Sharing of fetoplacental circulation in monochorionic twin pregnancy is the underlying cause of further specific complications including fetofetal transfusion syndrome, selective fetal intrauterine growth restriction, and co-twin death [2].
Considering the neurologic sequelae in the survivor following monochorionic co-twin death is thought to be a rare complication so the accurate frequency is not clear and the clinicopathologic study is not adequate. Here we report a case of neurologic complications in surviving intrauterine fetus following cotwin’s death in the second trimester and subsequent fetofetal transfusion syndrome in a monochorionic twin pregnancy.
Case presentation
A healthy 22-year-old nulliparous Iranian lady had an unexpected monochorionic diamniotic twin pregnancy. Two fetuses were seen at 9-week ultrasound scan with crown-rump length measurements appropriate for gestational age which was estimated by the last menstrual period. The scan revealed a single placental mass, one intertwin membrane with a T-sign, and two amniotic sacs. At 18 weeks gestation, an anomaly scan except for the discrepancy between the twins’ gestational age (3 days) and weight (204 gr and 313 gr) showed no abnormality. The amniotic fluid and fetal doppler of both twins were normal without ultrasound obvious features of fetofetal transfusion. Regarding the discrepancy between the twins, The patient was informed that the ultrasound findings need to be visited at short-term intervals. She had poor health and a low socioeconomic condition and didn’t visit until 29 weeks that she was referred from a health center because of occasional abdominal pains radiating to the groins and an uncertain diagnosis of preterm labor.
Ultrasound examination at 29 weeks of gestation showed the pregnancy was complicated by fetofetal transfusion syndrome. One fetus was demised with oligohydramnios, invisible bladder, echogenic bowel loops, and biophysical profile of zero, and the other baby was found to have polyhydramnios (a maximum amniotic pool depth of 11 cm), increased cardiothoracic ratio, significant tricuspid regurgitation and reverse flow in ductus venosus. Besides, ultrasonography exam of the alive fetus showed a diffuse pattern of small sonolucent areas with unusual echogenicity due to cystic cavity appearances around the cerebral ventricles of the surviving twin conducting to the assumptive diagnosis of multicystic encephalomalacia (Figure 1).
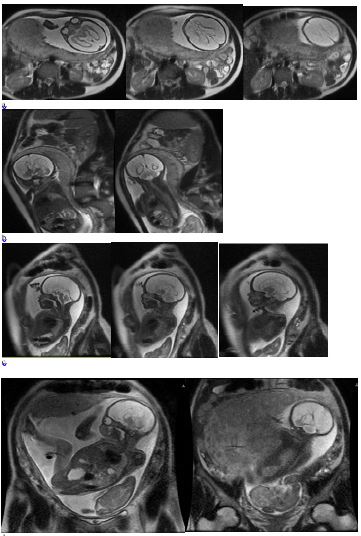
Magnetic resonance imaging of the brain proved the diagnosis of extensive multicystic encephalomalacia. There was diffuse and severe white matter volume loss at the bilateral cerebrum, severe and diffuse thinning of the corpus callosum, and ex-vacuo dilatation of lateral ventricles (Figure 2). Cerebellar hemispheres were spared.
The patient was advised for immediate delivery because of a poor outcome pregnancy but the mother insist on the continuation of the pregnancy because of her belief and left the clinic. 4 weeks later at 33 weeks of gestational age, she came back to the hospital with a rupture of amniotic membranes, watery discharge, and intermittent crampy abdominal pain. 4 hours later two babies were born by vaginal delivery without cardiac activity.

Discussion
Single intrauterine fetal death in monochorionic twin pregnancy may be associated with a severe neurological outcome in surviving cotwin. Although some theories have been presented to depict the exact pathogenesis of the brain lesions found in survivor cotwin, including fetofetal hemorrhage, preceding twin-to-twin transfusion syndrome, and congenital malformations, it is now well established that acute fetofetal hemorrhage is the main phenomenon involved in the development of brain lesions in survivor cotwin [2].
This report showed the prenatal neurological consequences in the survivors of monochorionic twin pregnancy complicated by single intrauterine death in the second trimester of gestation followed by fetofetal transfusion syndrome.
Twin-to-twin transfusion syndrome also known as fetofetal transfusion syndrome is a serious complication that arises in approximately 15% of monochorionic twin pregnancies [3,4]. Because of a discrepancy between the blood flow of the placental arteriovenous anastomoses, we will encounter hypovolaemia/hypotension in the donor twin and hypervolemia/hypertension in another recipient fetus [5]. Consequently, in subjects of monochorionic twin pregnancy with a severe fetofetal transfusion syndrome, cerebral injury to both donors and recipients is highly probable. According to the literature, the prevalence of cerebral lesions and the incidence of long-term neurological morbidity were reported in 13–35% [6,7] and 10–25% [6] respectively.
Hillman et al. [8] in their systemic review study indicated that among the surviving monochorionic twins after the death of cotwin, abnormal postnatal cranial imaging and neurodevelopmental impairment are seen at 34% and 26% of cases respectively. They explained the presence of acute and brief transfusional events from the live fetus to the dead fetus through the placental vascular anastomoses leading to hypoperfusion and subsequent hypoxic-ischemic brain injury. The time and duration of brain hypoperfusion play a crucial role in the anatomical distribution and pattern of cerebral hypoxic-ischaemic lesions [9]. Multicystic encephalomalacia (MCE) or parenchymal hemorrhage is the consequence of hypotensive insult before 28 weeks of gestation similar to our case.
Multicystic encephalomalacia refers to varying-sized cystic lesions in the brain parenchyma and can be seen in developing fetuses or infants and needs to be distinguished from porencephaly and hydranencephaly. As mentioned earlier, hypoxic or ischemic insults make liquefactive necrosis of brain parenchyma and subsequent formation of cystic lesions that start at the periventricular area and may extend onto the cortex [1].
Neurological complications in survivors of single monochorionic cotwin death are thought to be rare because of double death in this period [10].
However, in a couple of case reports, brain damage is reported in the surviving co-twins following single fetal death in monochorionic twin pregnancies [11-13].
As mentioned earlier, if this condition is observed in the brain of the survived cotwins of monochorionic pregnancy following cotwin death it would be associated with poor clinical outcomes and irreversible brain damage which manifests as severe developmental delay, epilepsy, microcephaly, spastic hemiplegia, or tetraplegia [14-17].
Finally, although it is difficult to anticipate the neurological outcomes in surviving cotwin related to single intrauterine death and/or fetofetal transfusion syndrome, it is important to keep this entity in mind when single fetal death occurred in monochorionic cotwin pregnancies. Moreover, obstetricians should be well familiar with the development and anatomy of the fetal brain so that if they see neurological complications in surviving twins following the death of the co-twin in monochorionic pregnancies, they can guide the pregnant mother and make the right decision to terminate the pregnancy.
Conclusion
We declare the case of neurological outcomes in surviving fetus of monochorionic twin pregnancy following monochorionic co-twin death in the second trimester. The present case emphasizes the high risk of monochorionic twin pregnancies especially neurological complications in survived twins following cotwin’s death and fetofetal transfusion. Therefore, obstetricians should be cautious and make pregnant women advised properly because of the risk and assess the fetal brain of surviving cotwin using ultrasound and magnetic resonance imaging after the co-twin demise to look for evidence of hypoxic-ischemic injury.
Declarations
Acknowledgments: Not applicable.
Authors’ contributions: Bahman Rasouli and Elahe Zare Mehrjerdi were involved in drafting the manuscript. All authors read and approved the final version of the manuscript.
Funding : No funding was available.
Availability of data and materials : Not applicable.
Ethics approval and consent to participate : Consent for publication Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Competing interests : The authors declare that they have no competing interests.
References
- Madakshira M, Gupta K, Uthamalingam P, Kapatia G, Saini S. Multicystic Encephalomalacia: An Autopsy Report of 4 Cases. Autops Case Rep. 2020; 10(4): e2020208.
- Hirose M. Encephalomalacia in Surviving Twin After Single Fetal Death Diagnosed at 18 Weeks of Gestation in Monochorionic Twin Pregnancy. Am J Case Rep. 2013; 14: 341-4.
- So P, Li K, Yeung T, Sin W. Multicystic Encephalomalacia and Gastrointestinal Injury Following Single Fetal Death in First Trimester and Subsequent Fetofetal Transfusion Syndrome in a Monochorionic Triplet Pregnancy: A Case Report. BMC Pregnancy Childbirth. 2019; 19(1): 311.
- Kilby MD, Baker PN, Critchley HO, Field DJ. Consensusviews arising from the 50th study group: multiple pregnancy. In: Multiple pregnancy. London: RCOG Press; 2006; 283-6.
- Rehan VK, Menticoglou SM. Mechanism of visceral damage in fetofetal transfusion syndrome. Arch Dis Child Fetal Neonatal Ed. 1995; 73(1): 48-50.
- Lopriore E, van Wezel-Meijler G, Middeldorp JM, Sueters M, Vandenbussche FP, Walther FJ. Incidence, origin, and character of cerebral injury in twin-to-twin transfusion syndrome treated with fetoscopic laser surgery. Am J Obstet Gynecol. 2006; 194(5): 1215-20.
- Wee LY, Fisk NM. The twin-twin transfusion syndrome. Semin Neonatol. 2002; 7(3): 187-202.
- Hillman SC, Morris RK, Kilby MD. Co-twin prognosis after single fetal death: a systematic review and meta-analysis. Obstet Gynecol. 2011; 118(4): 928-40.
- Barkovich AJ. Brain and spine injuries in infancy and childhood. Congenital malformations of the brain and the skull in pediatric neuroimaging. Chapters IV and V. In: Barkovich AJ, editor. Pediatric neuroimaging. Third ed. Philadelphia: Lippincott, Williams & Wilkins; 2000; 157-249.
- Malinowski W, Koktysz R, Stawerski P. The case of monochorionic twin gestation complicated by intrauterine demise of one fetus in the first trimester. Twin Res Hum Genet. 2005; 8: 262-66.
- Takahashi H, Baba Y, Matsubara S. Brain damage of surviving co-twin following single fetal death in monochorionic diamniotic twin pregnancy at 8-9 weeks’ gestation. Acta Obstet Gynecol Scand. 2014; 93(12): 1336.
- Weiss JL, Cleary-Goldman J, Tanji K, Budorick N, D’alton ME. Multicystic encephalomalacia after first-trimester intrauterine fetal death in monochorionic twins. Am J Obstet Gynecol. 2004; 190(2): 563-5.
- Suzuki S. Single fetal demise at 10-14 weeks of monochorionic and dichorionic twin pregnancy. J Clin Med Res. 2016; 8(4): 331-3.
- Flodmark O, Wiklund LM. Paediatric neuroradiology. In: Grainger RG, Allison DJ, Adam A, Dixon AK, editors. Grainger and Allison’s diagnostic radiology. 4th ed. Edinburgh: Churchill Livingstone. 2001; 2480-2.
- Ozduman K, Pober BR, Barnes P, Copel JA, Ogle EA, Duncan CC, et al. Fetal stroke. Pediatr Neurol. 2004; 30(3): 15162.
- Weidenheim KM, Bodhireddy SR, Nuovo GJ, Nelson SJ, Dickson DW. Multicystic encephalopathy: review of eight cases with etiologic considerations. J Neuropathol Exp Neurol. 1995; 54(2): 268-75.
- Orejón de Luna G, Mateos Beato F, Simón de las Heras R, Miralles Molina M. Multicystic encephalomalacia. Review of 19 cases. An Esp Pediatr. 1997; 46(1): 33-9.