
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 4
Cerebral hemispheric tumors in children: Clinical features, pathology, radiology & its management
Gouda Amiya Kumar1; Tiwari Swaminath Umashankar2; Mishra Sudhansu Sekhar1; Das Bidyut Prava3*
1Deptartment of Neurosurgery, SCB Medical College, Cuttack, Odisha, India.
2Deptartment of Neurosurgery, Kalinga Institute of Medical Science, Bhubaneswar, Odisha, India.
3Head of the Department of Pathology, F.M. Medical College & Hospital, Balasore, Odisha, India.
*Corresponding Author : Das Bidyut Prava
Head of the Department of Pathology, F.M. Medical College & Hospital, Balasore, Odisha.
Plot No.: B-1512, CDA, Sector-6, Markatnagar, Cuttack, Odisha, Pin-753014.
Email: drbidyutpravadas24@gmail.com
Received : Jun 25, 2023
Accepted : Jul 13, 2023
Published : Jul 20, 2023
Archived : www.jcimcr.org
Copyright : © Prava DB (2023).
Abstract
Introduction: Brain tumors are the commonest tumors (20-22%) in children after leukemia’s (30%) and have a number of specific features compared to adults.
Aims & objectives: To study the incidence & distribution of cerebral hemispheric tumors, its various clinical presentation, imaging characteristics, pathological features and outcome after advocated treatment.
Material & methods: This includes 18 cases of cerebral hemispheric tumors admitted to the department of Neurosurgery, SCB Medical College & Hospital, Cuttack between October 2019 to December 2021. Pre-operative workup included a detailed neurological examination and imaging studies with CT & MRI as per requirement. Extent of resection by post op CT was done & tumor was confirmed by neuropathologist of our institute. The outcome was analysed with respect to age, gender, extent of resection, tumor location and his pathology report.
Discussion: Hemispheric Glioma in children is relatively uncommon and malignant gliomas are still rarer. In our study 12.5% cases were GBM. The childhood primary GBM resembles their adult counter parts with regards to clinical history and show no evidence of previous low grade astrocytoma and share similar histopathological features. However the pattern of genetic alterations in paediatric primary GBMs appear to be district from those of adult GBM.
Conclusion: In our study male & female children were equally affected. Most common clinical features was headache followed by vomiting. Right lobe was more commonly involved followed by parietal lobe. Astrocytoma was most common in males than females while choroid plexus papilloma was more common in female. Ependymoma & PNET have equal incidence in male & female children.
Large majority of cases showed P53 protein expression & loss of P16 & P 27 pro expression.
Keywords: Hemispheric glioma; Glioblastomultiforma; Astrocytoma.
Citation: Kumar GA, Umashankar TS, Sekhar MS, Prava DB. Cerebral hemispheric tumors in children: Clinical features, pathology, radiology & its management. J Clin Images Med Case Rep. 2023; 4(7): 2507.
Introduction
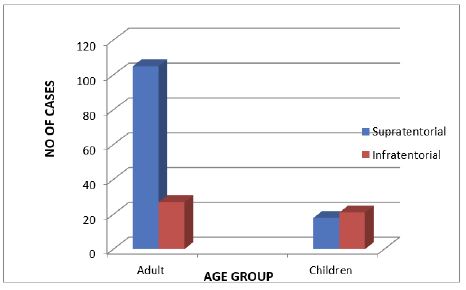
Brain tumors are the commonest tumors (20-22%) in children after leukemia’s (30%), although they are still the leading cause of cancer deaths and have a number of specific features compared to adults. Overall, there is an equal incidence of supratentorial and infratentorial tumors in the pediatric population. About 60% of supratentorial tumors are glial-based, and the vast majority (80%) are low-grade in nature. Cerebral hemispheric tumors in children are a diverse group of lesions. Presenting signs and symptoms vary extensively according to tumor location and tumor aggressiveness.
In general, the symptoms at initial presentation reflect the location of the lesion. The duration of symptoms often predict the aggressiveness of the tumor, with high-grade tumors producing symptoms over a shorter time course. Tumors in the temporal lobe often manifest as seizures, whereas tumors located in the frontal lobe may first give rise to personality changes or headaches. Some symptoms, such as nausea and vomiting, are non-localizing and their cause may be misdiagnosed as a gastrointestinal disease or migraine headaches. The clinical signs are multiple and non-specific and depend on the site of the tumor and age of the child. These include signs of Raised Intracranial Pressure (RICP) and various neurological signs (epilepsy, visual and endocrine disturbances, ataxia, and cranial nerve palsies). Signs are more misleading in young children (macrocephaly, bulging of the fontanelles, feeding difficulties, failure to acquire new skills, hypotonia and irritability). In the end, verification requires neuroimaging of the brain, and the decision to start with a Computed Tomography (CT) or Magnetic Resonance Imaging (MRI) examination depends on the acuity of presentation.
Unlike adults, metastases are very rare in children. Brain tumors are almost invariably primary and extra-axial tumors are extremely rare. Hemispheric tumors constitute approximately 15% of tumors and often cause epilepsy. The site provides a guide as the type of tumor. Tumors are classified by their histological type and grade (level of malignancy) in the WHO 2007 classification Grades 1 and 2 are benign tumors and grades 3 and 4 are malignant. There is considerable heterogeneity in histological types in children, both benign and malignant. Superficial hemispheric tumors are Ganglioglioma, DNET (dysembryoblastic neuronal tumor), Pleomorphic xanthoastrocytoma, Angiocentricglioma, and Oligodendroglioma while Deep hemispheric tumors are Embryonic tumor, Malignant glioma and Ependymoma.
Treatment depends on the histological grade and type and on the staging assessment but also on the child’s age. Tumors in children under 6 months old carry a poor prognosis because of the higher incidence of malignancy, larger tumor size and the contraindication to radiotherapy because of the adverse effects on the developing brain. Surgery for brain gliomas has become more and more aggressive. This is based on clinical data that support better patient survival and quality of life after gross total removal of both low- and high-grade lesions. However, the resection of tumors located in eloquent brain areas, such as the rolandic region and frontotemporal speech areas, requires the identification of functional cortical and subcortical areas that must be respected during surgery. Moreover, the dogmatic assumption that tumoral tissue could not retain function has been repeatedly questioned by neurophysiologic and functional magnetic resonance imaging studies. In response to the need for a safe surgery in eloquent brain areas, the past decade has seen the development of a number of techniques to map brain functions, including, but not limited to functional magnetic resonance imaging, magnetoencephalography and positron emission tomography. The neurophysiologic contribution to brain mapping has been evident since the late 19th century with the pioneering work of Fritsch and Hitzig and Bartholow. In the 20th century, Penfield and colleagues made invaluable contributions through intraoperative mapping of the sensorimotor cortex, whose findings have been substantiated by a number of recent studies.
Our understanding of the molecular genetics and epigenetic abnormalities in these different lesions has improved significantly over the past decade, allowing us to better predict the clinical course. The better understanding has opened the door for molecularly targeted therapy and has demonstrated the importance of sending fresh tumor to the pathologist for banking in every case. In all cases, these lesions need to be aggressively resected with the least amount of morbidity. Fortunately, advancements in intraoperative navigation and intraoperative MRI have led to improved surgical resections with fewer neurological deficits or complications.
There are very few published reports on the pediatric cerebral hemispheric tumors in India and hence the present study therefore attempts to profile the hospital based pediatric cerebral hemispheric tumors with the objective to determine the morphological pattern, the frequency of distribution of cerebral hemispheric tumors in children below eighteen years of age.
Aims & objectives
1. To study the incidence and distribution of cerebral hemispheric tumors in children.
2. To study the various clinical presentations of cerebral hemispheric tumors in children.
3. To study the various imaging features of cerebral hemispheric tumors in children.
4. To study the outcome after advocated treatment of cerebral hemispheric tumors in children.
Materials and methods
18 cases of cerebral hemispheric tumors were admitted in Department of neurosurgery, SCB Medical College Cuttack between October 2019 to December 2021 included in this study. Informed and Written consent taken from all the participants. There hospital record reviewed retrospectively including follow-up notes and imaging studies.
Preoperative workup included a detailed neurological examination and imaging studies with CT and MRI as per requirement. Extent of resection by post op CT within 24 hours if feasible and the tumor was confirmed by neuropathologist of our institute.
The patient underwent regular follow-up and clinical examination at each visit. Recurrent tumor was judged according to findings on imaging studies which was taken at regular interval or appearance of symptoms. The outcome was analysed with respect to following variable: Age, gender, extent of resection, tumor location, and the histopatholgy report.
Inclusion criteria
• Tumors located in cerebral hemisphere.
• Patient age less than 18 years
Exclusion criteria
1. Patient age more than 18 years.
2. Patients who did not give consent for the study.
3. Patient with CNS lesions other than cerebral hemispheric tumors
Observations
Out of 171 cases of brain tumors operated in the department of Neurosurgery, SCB Medical College & Hospital, Cuttack during the period from October 2019 to December 2021, there were 18 cases of hemispheric tumors in children.
Table 1: Incidence of brain tumors in children & adults.
| Location | Adult | Children | Total | |||
|---|---|---|---|---|---|---|
| Supratentorial | 105 | 61.40 % | 18 | 10.5 % | 123 | 71.92 % |
| Infratentorial | 27 | 15.78 % | 21 | 12.28 % | 48 | 28.08 % |
| Total | 132 | 77.18 % | 39 | 22.78 | 171 | 100 % |
Age
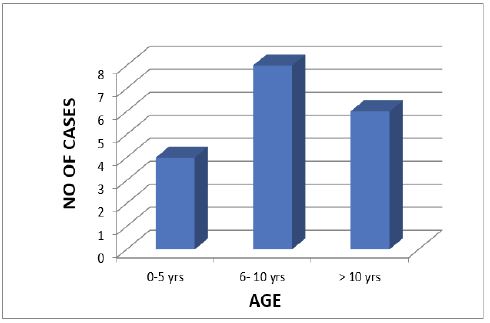
Nearly 80 % of pediatric supratentorial tumors were seen above the age of five, with nearly fifty percent of all tumors occurring between the age of 06 to 10 years, making it the most frequently affected age group (Table 2).
Table 2: Age distribution of cerebral hemispheric tumors in children.
| Age | 0-5 yrs | 6- 10 yrs | > 10 yrs |
|---|---|---|---|
| No of cases | 4 | 8 | 6 |
Sex
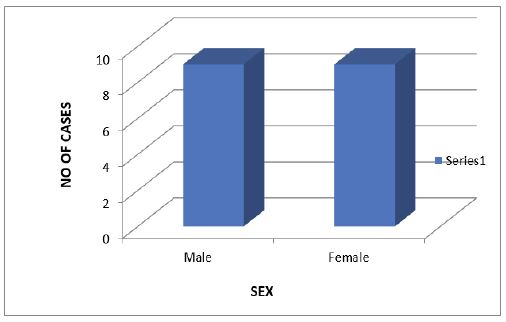
In our series the male to female ratio is 1:1 in all age group (Table 3)
Table 3: Sex incidence of hemispheric tumors in children.
| Sex | No of cases | |
|---|---|---|
| Male | 9 | 50 % |
| Female | 9 | 50% |
| Total | 18 | 100% |
Symptoms and signs
The clinical presentation depends on the site of tumor, biological behaviour and aggressiveness of tumors. Symptoms may be caused by local mass effect as well as due to increased intracranial tension (Table 4).
Table 4: Clinical features of hemispheric tumors in children (n=18).
| Symptoms and signs | No of patients | Percentage |
|---|---|---|
| Headache | 13 | 72.22 % |
| vomiting | 11 | 61.11 % |
| Seizure | 7 | 38.88 % |
| Hemiparesis | 6 | 33.33 % |
| Pappilodema | 5 | 27.77 % |
| Visual impairement | 4 | 22.22 % |
| Altered sensorium | 4 | 22.22 % |
Table 5: Hemispheric distribution of tumor in children.
| Hemisphere | No of cases | Percentage |
|---|---|---|
| Right | 11 | 61.11% |
| Left | 7 | 38.88% |
| Total | 18 | 100% |
Clinical features of hemispheric tumors in children
Headache (72.22%) and Vomiting (61.11%) were the most common symptoms in our study. Diminution of vision was present in 22.22% of patients at the time of presentation.
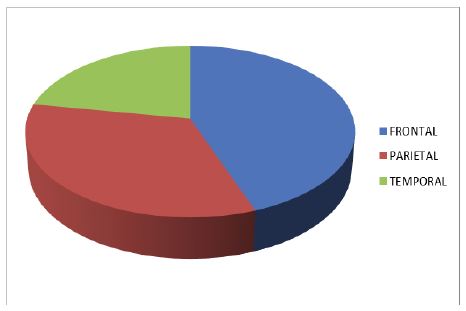
Location of hemispheric tumors in children
Cortical lobes are the most common site for hemispheric tumors followed by lateral ventricle. No tumor was found in the thalamic area in this study.
Right hemisphere was more commonly involved (61.11%) than left hemisphere (38.88%). Among the cortical lobes, frontal lobe was most commonly involved followed by parietal and temporal lobe.
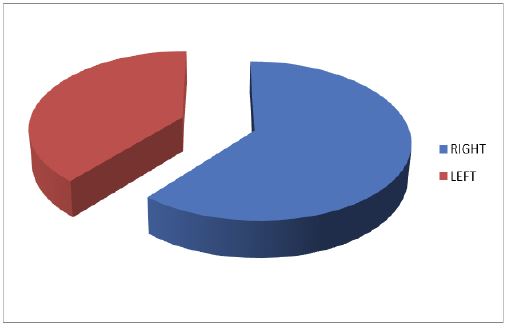
Table 6: Lobar distribution of tumor in children.
| Cortical lobe | No of cases | Percentage |
|---|---|---|
| Frontal | 8 | 44.44 |
| Parietal | 6 | 33.33 |
| Temporal | 4 | 22.22 |
| Total | 18 | 100% |
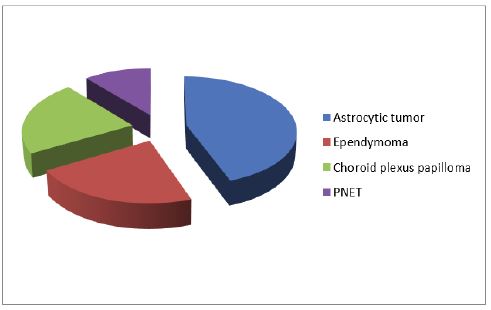
Pathology
In this study cases of astrocytoma was 8 (44.4%), ependymoma 4 (22.2%), choroid plexus papilloma 4 (22.2%) and PNET was 2 (11.1%) in number.
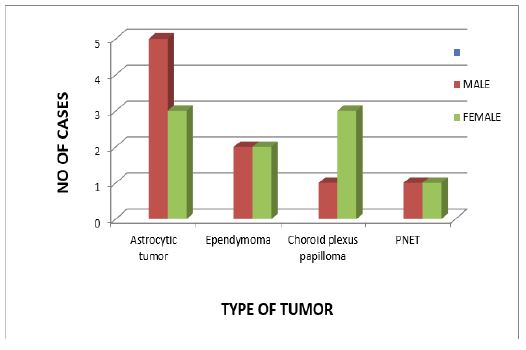
Sex incidence of different types of hemispheric tumors in children
In our study astrocytoma was more common in male while choroid plexus papilloma was predominant in female. Ependymoma and PNET had equal incidence in male and female.
The duration of symptoms prior to admission is from 2 days to 4 yrs depending on tumor types. Mean clinical history was 2.7 months. The mean clinical history was is 2 months for glioma, 4 months for PNET and more than 14 months for pilocytic astrocytoma.
Table 7: Pathology of hemispheric tumors in children (n = 18).
| Type of tumor | Total | M | F | M:F | Age range | MC age group |
|---|---|---|---|---|---|---|
| All types | 18 | 9 | 9 | 1:1 | 7 m- 17 yrs | 6–10 yr & 11-15 yr |
| Astrocytic tumor | 8 | 5 | 3 | 5:3 | 1.5-17 yr | 6-10 yr |
| Ependymoma | 4 | 2 | 2 | 1:1 | 3-12 yr | 4-7 yr |
| Choroid plexus papilloma | 4 | 1 | 3 | 1:3 | 2-6 yr | 3-5 yr |
| PNET | 2 | 1 | 1 | 1:1 | 4-5 yr | 2-5 yr |
In our study the most common age group for Astrocytoma was 6 to 10 years, for Ependymomas 4 to 7 years, for choroid plexus pappiloma 3 to 5 years and for PNET 2 to 5 years.
Out of 18 cases Gross total resection resection was possible in 6 cases and Near total resection in 8 cases leaving minimal tumor near neural or vascular structure and in 4 cases Subtotal resection was done according to the location and type of tumor. Squash cytology and Frozen section was done routinely to evaluate nature of tumor during surgery. Post operative chemotherapy / radiotherapy was given in 12 cases.
In keeping with most other studies (Table 8), the cerebral hemispheric tumors were more than infratentorial tumors in children.
Table 8: Comparision of present data with other series.
| Study | Region (no. of cases) | Age (yrs) | MC tumor | 2nd | 3rd | M:F | Mean age | Hemispheric % | Infratentorial % |
|---|---|---|---|---|---|---|---|---|---|
| Rickert et al, 2001 | Germany (340) | < 18 | Astro (47.3%) | Cranio (5.6%) | NA | 1.56:1 | NA | 53.3 | 46.7 |
| Wong TT et al,002 | Taiwan (986) | < 18 | Astro (31.1%) | Gct (14%) | Cranio (8.3%) | 1.4:1 | 7.8 | 58.3 | 41.1 |
| Ahmed N et al, 2006 | Pakistan (81) | < 15 | PNET (49.4%) | Astro (34.6%) | MG (5%) | 2.5:1 | 8.8 | 33.3 | 66.7 |
| Peris-Bonet et al, 2007 | Europe (19,531). | < 15 | Astro (40%) | PNET (40% | NA | 1.1:1 | NA | NA | NA |
| Zhang R et al, 2007 | China (763) | < 18 | Astro (25%) | Cranio (12.8%) | GCT (8.9%) | 1.56:1 | 12.68 | 62.4 | 31.1 |
| Zhou D et al 2008 | China (1485) | < 18 | Astro(30.5%) | Cranio (18.5%) | GCT (7.8%) | 1.6:1 | NA | 57.1 | 35.2 |
| A Narasimhaiah et al, 2011 | India (1043 | Astro(47.3%) | Cranio (9.7%) | NA | 1.7:1 | 10.9 | 53.3 | 40.6 | |
| Our study | Scb (18) | < 18 | Astro (44.4%) | Ependy&cpp (22.2% each) | PNET (11.11%) | 1:1 | 6-10 yrs | 50.8 | 49 |
Follow up
Total 18 cases of hemispheric tumors in children were operated. 4 cases were lost to follow up. Total 3 deaths occurred in this study with a follow up of 2 years. A case of GBM read mitted within 6 months for recurrence, was re operated but he was again admitted within 3 months with recurrence with features of raised intracranial pressure and died. Two patients, of ependymoma and one choroid plexus papilloma died within 4 months of surgery. One patient of PNET developed post operative hydrocephalus for which right MPVP shunt was inserted.
Glioblastomamultiforme (GBM) are invariably associated with poor prognosis, with median survival of 10-12 months (Kleihues P et al 2000) [1] and 5 yr survival is still rare and is reported to be around 4-5% (McLendon et al 2003).
P Deb et al. 2005, found 6 cases of GBM with long term survival of more than 5 years. The factors that possibly led to long term survival could be younger age, female sex, and aggressive surgical resection, in conjunction with features like focal oligodendroglial component, giant cell GBM, lack of small anaplastic cells, areas with extensive GFAP reactivity and a low proliferation index with high p53 immunopositivity.
Pediatric high grade gliomas (World Health Organisation grade III and IV Astrocytomas) remains the tumor with very poor prognosis for which novel therapeutic strategy are needed. Poly ADP-ribose polymerase (PARP) is known to have multiple functions in tumors, including single strand DNA repair and induction of caspase – independent apoptosis. PARP is expressed at high levels in many pediatric high grade gliomas, and in these tumors, the ability of PARP to activate AIF appears to have been lost.
According to Stuart J Smith et al 2011, PARP represents a promising therapeutic target for these lesions and warrants evaluation in clinical trials.
Treatment
Management of hydrocephalus
Because most patients present with symptoms of increased ICP secondary to hydrocephalus, the initial step is to decide whether CSF drainage is required. In the presence of a decline in neurologic function, however, an external ventricular drain should be inserted immediately, before definitive tumor management. Placement of a ventriculoperitoneal shunt, although an acceptable alternative, does not allow external CSF drainage and ICP monitoring in the intraoperative and postoperative setting.
Operative treatment
For both CPP and CPC, GTR is associated with the most favorable outcome in patients with such tumors. Although treatment in each case must be individualized, the following steps are part of most surgical plans: (1) temporary or permanent resolution of hydrocephalus, (2) identification of the arterial supply, and (3) planning the surgical approach to allow access to the vascular supply and maximal exposure of the tumor.
The two features of choroid plexus tumors that can make resection exceedingly difficult are vascularity and large size. Piecemeal resection is usually associated with increased blood loss. The most effective strategy is early identification and ligation of the feeding artery. In general, en bloc excision is recommended, although this may not be feasible with very large tumors. If the tumor has to be removed in part, then gradual and gentle coagulation of the fronds of the tumor allows its manipulation without excessive bleeding and enables shrinkage of the tumor, thereby creating additional space around the periphery of the mass.
The primary goal of CP tumor surgery is to achieve a gross total resection and to alleviate any hydrocephalus. The tumor location necessitates an approach through normal neuron parenchyma, except in some fourth ventricular lesions.
The standard surgical technique of internal debulking leads to massive bleeding and endangers the life of the patients, hence early vascular pedicle control has been strongly recommended.
Most patients with CPPs can expect long-term survival. The length of survival with CPC, however, is much worse. In a large meta-analysis, the rates of 1, 5, and 10 year survival were 90%, 81%, and 77%, respectively, with CPP, in comparison with only 71%, 41%, and 35%, respectively, with CPC.
For the lower grade papillomas, surgical resection may be the only treatment required. In the more aggressive carcinomas, gross total resection with adjuvant chemotherapy or radiation will offer the best opportunity for cure.
Postoperative chemotherapy for carcinoma does improve survival rates, and intensive chemotherapy is often used with the aim of delaying or avoiding radiation.
Progression from papilloma to carcinoma has been reported. Although both tumors have been shown to metastasize, the survival rate of patients with papilloma is significantly higher.
Discussion
Brain tumors are the leading cause of cancer related death and account for 20% to 30% of all childhood cancers. CNS tumors are the most common neoplasm among those 0-17 years old, with an average annual age adjusted incidence rate of 5.42 per 100,000. In our study male & female ratio was 1:1 in all age group. Gliomas may occur at any age but most commonly encountered in adults and old age. Review of current literature indicates an overall pediatric CNS glioma incidence 20%-30% of all pediatric cancers. There is slight male predominance with female/male ratio is 1:1.5. We observed that there is slight male predominance in glioma that is 1:1.3. Tumors with higher grade, more unfavourable locations, and poorer prognosis have generally occurred in younger than 3 years. Overall, the most common CNS tumor seen in child hood are: Astrocytomas, Ependymomas, and germ cell tumors. Glioma account for 50-60% and PNET 1.9%. we also observed that gliomas being the more common tumor followed in decreasing order PNET, and choroid plexus papillomas. Childhood high grade lesions are characteristically known to have nonspecific symptomatology. The elasticity of skull and non cooperation makes diagnosis difficult. Quite often a local swelling of cranial vault may be the first sign in many children. Common clinical manifestation in hemispheric pediatric tumors include signs of raised ICP, focal neurological deficits, seizures and other rare symptoms and signs based on their location. We also observed raised ICP being the predominant presenting symptom, followed by seizures and focal deficits in deceasing order. Few patients had visual symptoms also.
Overall, frontal lobe is frequently affected (8.6%), followed by temporal (6.4%), parietal (4.0%) and occipital lobe (1.1%) account for 20.1% of all tumors. For malignant tumors, frontal (23.2%) lobe was most commonly involved cerebral lobe followed by temporal (17%), parietal (10.9%), and occipital (2.9%) account for 54% of tumors. In this study the most frequently affected lobes are frontal followed by parietal lobe.
Glioma represents approximately 28% of all tumors and 80% of malignant forms where approximately 47.9% of tumors in patients less than 19 years of age. There is decline in the incidence rate of gliomas and embryonal tumors type between age group 0-19, whereas incidence of PNET is highest in the 0-4 age group. We have observed all PNETs before 14 years of age and decreasing glioma incidence in 14 – 18 years of age. However, in both age groups glioma was the most common hemispheric CNS tumor.
Glioblastoma is the second most frequently reported histology and the most common malignant tumor. Glioblastoma accounts for 15.4% of all primary brain tumors and 45.6% of primary malignant brain tumors. Glioblastomas are more common in older adults and less common in children and comprise approximately 3% of all CNS tumors reported in 0-19 years of age. Glioblastoma has been found in 19.4% among high grade lesions and is 1.6 times more frequent in males. Relative survival estimates for glioblastomas are quite low and only 5% of patient survive five years post diagnosis. Most of the studies on high grade gliomas reported 5 year event free survival of 46% with combined chemo-radiotherapy and 18% when treated with radiotherapy alone [8-11]. One year progression free survival of glioblastoma is 15% in this series and two years progression free survival 23.8% and 5 years PFS 10.2% in grade III.
Embryonal tumors are the most frequently reported tumor type in children ages 0-4 years and the second most common tumor type overall in 0-19 years. Relative survival estimates for embryonal tumors are low but vary significantly by histology. Reviews of literatures reveal that 10 years survival for PNET is 42.6%. 25.9% for ATRT whereas in our observation PNET being third most frequent tumor with one and two year progression free survival is 50% and 25% respectively. In the present study there was no significant benefit either chemotherapy or chemo and radiotherapy in overall survival except in added 3 months longitivity by giving radiotherapy in PNET patient.
Studies done in India by A. Narasimhaiah, Rajsekhar et al. 2011 in 1043 patient found hemispheric tumors in 53.3% and infratentorial tumors in 40.6% [2].
Cho et al 2011, from Japan and Makino et al. 2010, of korea also found that cerebral hemispheric tumours predominant than infratentorial tumors [3].
Ricket et al. 2001, of Germany studied on 340 cases and reported hemispheric tumors in 53.3% and infratentorial tumors in 46.7% [4].
Zhang R et al 2007, of China studied on 763 cases and found 62.4% of hemispheric tumors and 31.11% of infratentorial tumors [5].
Zhou D et al, 2005 from china studied 1485 cases and found 57.1% of hemispheric tumor and 35, 0.2% of infratentorial tumors [6].
However, Ahmed et al, 2007 of Pakistan studied 81 cases and found 33.3% hemispheric tumors and 66.7% infratentorial tumors [7].
In our study, the number of infratentorial tumors (53.84%) were more than supratentorial tumors (46.15%) in children.
The male to female ratio in our study is 1:1. However there is male prepdominence in other studies done in India and abroad.
A Narasimhaiah, Rajsekhar et al, 2011 studied 1043 patient and found male to female ratio of 1.7 :1 [2].
In our study the male to female ratio is 1:1. However there is male predominanace in other studies done in India and abroad. A. Narsimhaiah, Rajsekhar et al, 2011 have found male predominance in the ratio of 1.7:1 among 1043 patients [2]. Peris- Bonet et al, 2006 studied 19531 cases ad found male to female ratio of 1.1:1. Ahmed N et al, 2007 studied in Pakistan and found maximum male preponderance at a ratio of 2.5:1. This is more likely to represent a reflection of the gender bias present in the subcontinent rather than a true regional difference. We have also observed male preponderance in astrocytic tumor [7].
The signs and symptoms were headache (81.3%), vomiting (65.6%), visual impairment (34.4%), hemiparesis (25%), papillodema (21.9%), seizure (15.5%), altered sensorium in 15.5%. in a study of Mahapatra and Nandi (1985), they have reported 78% of children suffer from headache and vomiting.
In our study astrocytic tumors are 25%, PNET is 15.6%. A. Narasimhaiah, (47.3%), ependymomas (4.8%). The overall frequency of astrocytomas in Europe is around 40% (Peris-Bonet et al, 2006 Rickert et al, 2001) [4] and varies between 25% and 35 % in other Asian countries like Japan (Makino K, et al 2010) [3], China (Zhang R et al 2007, Zhou D et al 2005) [5,6] Korea (Cho et al 2002), and Pakistan (Ahmed N et al 2007) [7]. Pilocytic astrocytoma was the most common (22.33%) similar to other studies (Peris-Bonet R et al 2006). Pilocytic astrocytoma is common in the cerebellum (38.1%), optic chiasm (27.9%), supratentorial region (19.4%) and brainstem (9.3%) (AK Mahapatra, Kurawale et al 2011).
Ahmed N et al, 2007 found PNET to be most common 49 % in their study followed by astrocytictumors are the most common between 25 to 47 % [7-11].
Hemispheric glioma in children is relatively uncommon in childhood, 7-9% of childhood intracranial tumor. Malignant gliomas are much rarer in children than in adults, comprising only 5% to 10% of childhood intracranial neoplasms. In our study 12.5% cases are GBM which is quite high as compared to other studies due to small size of the patients, while A. Narasimhaiah, Rajsekhar et al, 2011 [2] found 8.7% of all astrocytomas in their studies of 1083 patients, and 17.2% by Cho et al, 2002. As we have total of 8 cases of astrocytic tumors which are a small number, any opinion about percent of GBM cannot be given and this needs a larger study. Frontal lobe was the commonly involved. Main presenting symptoms of GBM in our study were headache (85%), hemiparesis 66 %, nausea or vomiting (65%), and seizures (35%), pappilodema (45%) was the most common physical finding.
The primary glioblastoma, which typically affect older patients, are characterized by amplification of epidermal growth factor receptor gene (EGFR) along with deletion or mutation of phosphate and tensin homolog tumor suppressor gene (PTEN), a negative regulator of the phosphatidyl inositol 3 kinase/Akt signalling pathway. In contrast, secondary GBMs, which evolve from low grade lesions and occur in younger individuals, often have mutations of the tumor suppression gene TP53 but only infrequently have amplification of EGFR or alterations of PTEN.
The childhood pri GBM resembles their adult counterparts with regard to clinical history; they show no evidence of previous low grade astrocytoma, and they share similar histomorphological features. However, the patterns of genetic alterations in pediatric primary GBMs appear to be distinct from those in adult GBMs. The alterations of PTEN and amplification of EGFR were uncommon. A large majority of cases showed p53 protein expression. Loss of p16 and p27 expression was observed in a significant number of cases (vaishali Suri, Chitrasarkar et al 2009).
Summary and conclusion
Out of 171 cases of brain tumor in children admitted in the Dept. of Neurosurgery, SCB Medical College & Hospital, Cuttack during the period of study 18 were cerebral hemispheric tumors in children. In our study brain tumors in children were 22.78% while cerebral hemispheric tumors in children was 10.5%. The most common age group was 6 to 10 yrs and male as well as females were equally affected. The most common clinical feature was headache (72.22%) followed by vomiting (61.11%). The right lobe was more commonly involved (61.11%) than left lobe (38.88%) and the frontal lobe (44.44%) was more commonly involved followed by parietal lobe (33.33%). Astrocytomas was most common tumors found. Astrocytomas were more common in males than females while choroid plexus papilloma was more common in females. The Ependymoma and PNET has equal incidence in both male and female.
Cerebral hemispheric tumors in children are not uncommon but despite all the advances the overall survival and tumor progression did not differ significantly. This study had small sample size of 18 cases only largely because of Corona pandemic this precludes any definite conclusions.
References
- Kleihues P, Louis DN, Scheithauer BW, Rorke LB, Reifenberger G, et al. WHO classification of tumors, pathology and genetics of tumors of the nervous system. Lyon, France: IARC Press; 2000; 29-39.
- A Narasimhaiah, V Rajsekhar, Chyne R, Prasad MSN, Chacko AG, et al. Pediatric tumors of the central nervous system: A retrospective study of 1043 cases from a tertiary care center in south india: Childs Nerv. System. 2011: 27: 12571263.
- Makino K, KuratsuJ, Nakamura H, Yano S, Kumamoto BTG. Population based epidemiological study of primary intracranial tumors in childhood. Childs Nerv Syst. 2010; 26: 1029-1034.
- Rickert CH, Paulus W. Epidemiology of central nervous system tumors in childhood and adolescence based on the new WHO classification. Childs Nerv Syst. 2001; 17: 503-511.
- Zhang R, Shen WQ, Zhou LF. Primary pediatric CNS tumors statics: Study of 763 cases in a single institution. Zhonghua Yi Xue Za Zhi. 2007: 87: 442-447.
- Zhou D, Zhang Y, Liu H, Luo S, Luo L, et al. Epidemiology of nervous system tumors in children: a survey of 1485 cases in Beijng Tiantan Hospital from 2001 to 2005. Padiatric neurosurg. 2008; 44: 97-103.
- Ahmed N, Sadik S, Bhurgri Y, Shakoor KA. Pediatric brain tumors at a tertiary care hospital in Karachi. Asian Pac J Cancer Prev. 2007; 8: 399-404.
- Raffel C, Frederick L, O Fallon JR, Atherton-Skaff P, Perry A, et al. Analysis of oncogene and tumor suppressor gene alterations in pediatric malignant astrocytomas re-veals reduced survival for patients with PTEN mutations. Clin Cancer Res. 1999; 5: 4085-4090.
- Cheng Y, Ng HK, Zhang SF, Ding M, Pang JC, et al. Genetic alterations in pediatric high-grade astrocytomas. Hum Pathol. 1999; 30: 1284-1290.
- Khatua S, Jalali R. Recent advancesin the treatment of childhood brain tumors. Pediatr Hematol Onco. 2005; 22: 361-367.
- Jones DT, Witt O, Pfister SM. MAPK pathway activation in pilocytic astrocytoma. Cell Mol Life Sci. 2012; 69: 1799-1811.