
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 4
Liver biochemical profile and antibiotic susceptibility pattern of Salmonella enterica serovar Typhi among patients attending Dschang district hospital, Cameroon
Jean-De-Dieu Tamokou*; Tito Aloys Ndima Etouke; Josiane Claire Lambou Sonkoue; Nafissetou Ndam Mewouo; Pénuel Gaius Djofang; Brice Parfait Waffeu Tagne; Elvire Damaris Kwapnang Nzounkeu
Research Unit of Microbiology and Antimicrobial Substances, Department of Biochemistry, Faculty of Science, University of Dschang, P.O. Box 67 Dschang, Cameroon.
*Corresponding Author : Jean-De-Dieu Tamokou
Research Unit of Microbiology and Antimicrobial Substances, Department of Biochemistry, Faculty of Science, University of Dschang, P.O. Box 67 Dschang, Cameroon.
Tel: +237 677 000 897
Email: jtamokou@yahoo.fr &
jean.tamokou@univ-dschang.org
Received : Jun 22, 2023
Accepted : Jul 13, 2023
Published : Jul 20, 2023
Archived : www.jcimcr.org
Copyright : © Tamokou JDD (2023).
Abstract
Background: Enteric fever usually leads to hepato-cellular necrosis, a likely cause of alteration in liver biochemical markers in the serum. Further, the emergence of multi-drug-resistant Salmonella to common antibiotics, has complicated the treatment and management of this infection. The present study aims at evaluating the effect of Salmonella Typhi infection on biochemical markers of hepatic injury, and to determine the antibiotic susceptibility pattern of isolates.
Methods: A cross-sectional survey was conducted from March to June 2021 on 110 consented volunteer’s patients. Their socio-demographic, clinical and life style characteristics as well as risk factors were collected using questionnaires. Liver biochemical parameters such as Alanine Transaminase (ALT), Alkaline Phosphatase (PAL) and Total Bilirubin (TB) were analyzed in serum. The antibiotic susceptibility pattern of S. enterica serovar Typhi isolated from stool culture was evaluated.
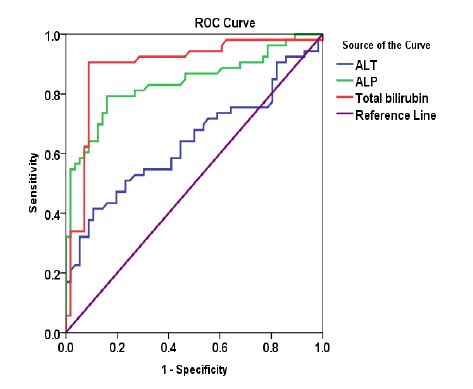
Results: Significant associations between S. Typhi infection and liver biochemical parameters were revealed by Receiver Operating Characteristic (ROC) curve analysis with area under the curves (95% CI) of 0.64 (0.534 - 0.746), 0.838 (0.76 - 0.917), and 0.893 (0.825 - 0.961) for ALT, ALP and TB, respectively. Antibiotics ofloxacin (100%) and levofloxacin (100%) were active against all the S. Typhi isolates. In contrast, the presence of Multi-Drug-Resistant (MDR) Salmonella Typhi was observed in the study population.
Conclusion: The present findings underline the involvement of S. Typhi in the modification of liver biochemical parameters. Data also highlighted the imperative need of conducting a rational prescription of antibiotics based on the local antibacterial susceptibility pattern.
Keywords: Typhoid fever; ALT; PAL; Total bilirubin; Risk factors; Antibiogram; MDR salmonella typhi.
Citation: Tamokou JD, Ndima Etouke TA, Lambou Sonkoue JC, Ndam Mewouo N, Djofang PG, et al. Liver biochemical profile and antibiotic susceptibility pattern of Salmonella enterica serovar Typhi among patients attending Dschang district hospital, Cameroon. J Clin Images Med Case Rep. 2023; 4(7): 2508.
Introduction
Enteric fever is a systemic infection caused by Gram-negative bacilli Salmonella enterica serovars Typhi and Paratyphi [1]. Salmonella species are facultative anaerobic bacteria and oxidase positive. They are usually motile, lactose negative, urease negative, citrate positive and acetyl methyl carbinol negative. S. enterica usually causes a localized infection of the gastrointestinal tract but can also proliferate in the reticulo-endothelial system, leading to systemic infection and death. The World Health Organization estimates that there are 11 to 20 million cases of typhoid fevers per year and about 161,000 deaths from typhoid fever annually [2]. Infection is contracted through ingestion of contaminated water and food by Salmonella species and usually from feco-oral origin. Therefore, the occurrence of typhoid fever is perceived as an indicator of poor personal and environmental hygiene. The course of the disease may be minor but sometimes fatal as result of cellular and biochemical alterations [3,4], that follow the infection. Indeed, there is a unique relationship between S. enterica and macrophages of the liver, spleen, intestinal lymphoid follicles and mesenteric lymph nodes that may be responsible for the pathogenesis of this infection. Functionally active cytokines (TNF alpha, IL-1, alpha and beta interferons) are synthesized by macrophages and are important sources of arachidonic acid metabolites and reactive oxygen intermediate species [5]. The derived products may contribute to cell necrosis, recruitment of other inflammatory cells, immune stimulation, vascular instability, initiation of the clotting mechanism, and other abnormalities associated with typhoid fever [5]. Liver injury is one of the complications that was early reported during typhoid fever [6], followed by increased numbers of cardiovascular diseases [7]. However, there are contrasting effects of Salmonella enterica infection on metabolic parameters.
Typhoid and paratyphoid fevers remain a public health problem despite availability and accessibility to potential antibiotics, added to discovery and development of new antibacterial drugs. Indeed, Salmonella species have rapidly become resistant to antibiotics including ampicillin, ceftriaxone and cotrimoxazole and to previously effective drugs such as ciprofloxacin [8]. Resistance to conventional antibiotic agents is recognized as one of the greatest challenges that physicians have to overcome in the management of typhoid fever [9]. S. enterica serotypes Typhi and Paratyphi, in particular, multi-resistant strains are relatively ubiquitous and are the causative agents of many endemic infections in the community [10]. It is generally accepted that the initial development of antibiotic resistant strains results from the misuse and abuse of antibacterial drugs, hence the need for respecting treatment protocols during the administration of antibiotics is required. Determination of antibiotic susceptibility profile of local Salmonella isolates remains crucial to physicians for the selection of appropriate antibiotics to treat patients. Nevertheless, given the time required for availability of antibiogram results that usually last for days and even weeks, depending on the availability of resources in health facilities concerned, an epidemiological update on the local susceptibility profile of Salmonella isolates is imperative to ensuring prompt treatment of infection without worsening the disease, and to prevent antibiotic resistance. The present study aimed at evaluating the effect of Salmonella Typhi infection on liver biochemical parameters and determining the antibiotic susceptibility pattern of isolates among patients visit Dschang district hospital in Cameroon, for medical care.
Materials and methods
Study design, population, and sampling method
A cross-sectional hospital based survey was carried out in the Laboratory of the Dschang District Hospital from March to June 2021. The study protocol was approved by the National Committee for Ethics in Human Health (CNERSH), Yaounde, Cameroon (ref: 2020/11/73/CE/CNERSH/SP). All participants willingly provided informed consent either by signing or placing their thumbprint on the consent form. Based on the inclusion criteria (being positive to Salmonella infection or not, being at least 21 years old and giving a favorable opinion for free participation in the study) and the non inclusion criteria (being pregnant, being patients on antibiotic therapy whose spectrum of action included Salmonella Typhi and Paratyphi, and having a pre-history of specific disorders like liver diseases, malaria, diabetes, cardiovascular diseases and kidney failure and having refused to sign informed consent), 134 participants were eligible for the study. Among them, subjects with hemolyzed blood serum and who did not provide the full amount of information required (n=24) were excluded from the analysis. Finally, 110 participants were included. Serum and stool samples were collected from 110 patients who agreed and provided consent to participate in the study. TyphiDot® IGM and IgG test was used to separate patients into two groups based on their serological status. The investigation was approved by the Ethics Review and Consultancy National Committee of Cameroon. The research was carried out in accordance with the principles of the Helsinki Declaration.
Collection of blood, biochemical and serological analyses
Blood collection was specifically done by a qualified laboratory technician. The antecubical vein of the forearm was selected and disinfected with a cotton wool swab impregnated with 70% alcohol. Five millilitres (5 mL) of venous blood were collected into a dry tube pre-labelled with an anonymised patient codes. The blood sample was allowed to clot completely before centrifugation at 3000 rpm for 15 min. Serum was separated from the clot into tightly screwed microfuge tubes and stored at -20°C. These frozen sera were later analyzed for assessment of the biochemical parameters. Serum Alanine Transaminase (ALT), Alkaline Phosphatase (ALP) and Total Bilirubin (TB) were measured using the method described in INMESCO commercial kits (INMESCO Gmbh- Germany), following manufacturer’s instructions.
Procedure for TiphyDot IgM and IgG test
TyphiDot IgM and IgG test (TyphiDot; Malaysian Biodiagnostic Research SDN BHD, Kuala Lumpur, Malaysia) is a dot ELISA kit that detects IgM and IgG antibodies against the Outer Membrane Protein (OMP) of the Salmonella Typhi. This test becomes positive within 2 to 3 days of infection and separately identifies IgM and IgG antibodies. The test is based on the presence of specific IgM and IgG antibodies to a specific 50 kDa OMP antigen, which is impregnated on nitrocellulose strips. The reaction tray was divided into 2 columns marked as G and M. Then, 250 μL of sample diluent was dispensed in each well and 2.50 μL of test /control was added followed by incubation for 20 minutes. The strips were washed with phosphate-buffered saline thrice, then, 250 μL of anti-human IgG and IgM was dispensed in each well and further incubated for 15 minutes. The wells were washed again, dispensed with 250 μL of colour development solution, and incubated for 15 minutes. A positive IgM was interpreted clinically as acute typhoidal illness, while IgM and IgG positive were taken as acute typhoidal illness in middle stage of infection and IgG positive was interpreted as chronic carrier or previous infection or reinfection.
Stool collection, isolation and identification of Salmonella enterica serovar Typhi
Stool vials were provided to patients and they were instructed on collection. The samples were quickly transported to the Laboratory of the Dschang District Hospital for microbiological analysis. Three grams of stools were introduced into 3 mL of sterile physiological saline and mixed. Then, 1 mL of the mixture was removed aseptically and inoculated into enriched selenite broth (9 mL) and incubated at 37°C for 24 h. In the presence of turbidity / bacteria, aliquot from stool culture bottles were sub-cultured onto a SS agar plate to obtain pure isolates. These pure isolates were inoculated in nutrient agar slant and stored at +4°C for further characterization and identifi cation. Identification of bacteria from positive culture plates was done with the use of standard microbiology techniques which included colony morphology, Gram stain, biochemical tests and serotyping [11]. The Analytical Profle Index (API 20E) was used to support the bacterial identifcation process (bioMerieux, France).
Antibiotic susceptibility testing
In vitro susceptibility of Salmonella isolates against antibiotics was performed using Kirby Bauer Agar Diffusion Method [12]. Antibacterial activity of antibiotics against Salmonella isolates was evaluated by measuring the clear zone of growth inhibition on agar surface around the discs. Results of disc diffusion tests were then interpreted using the M100-S25 scale [13]. Each assay was done in triplicate. The antibiotics tested were penicillins (ampicillin and amoxicillin), cephalosporins (ceftriaxone), fluoroquinolones (ciprofloxacin, ofloxacin, norfloxacin and levofloxacin), phenicols (chloramphenicol) and tetracycline (minocycline). Salmonella Typhi isolates were regarded as Multidrug Resistant (MDR) when they were resistant to one or more antibiotics in three or more classes of antimicrobials that the isolate is expected to be susceptible.
Statistical analysis
Data were entered into a form designed on Epi info v3.4.0, then exported to Statistical Package for Social Sciences (SPSS) 16.0 for statistical analysis. The study participants were divided into groups according to the results of their serological Typhidot test. The sero-prevalence of Salmonella infection in the studied population was calculated as the proportion of serologically positive IgM and IgM/IgG samples among all samples tested. The Pearson Chi-square or Fisher’s exact test when necessary was used to compare the relative frequencies of socio-demographic, clinical and life style characteristics between S. Typhi positive and negative groups for participants. Data on biochemical parameters were expressed as the mean ± Standard Deviation (SD). Cut-off values provided by the kits were used to classify the participant as abnormal (value above the reference range) and normal (value within the reference range). The means of biochemical parameters of the categories within each socio-demographic variable were subjected to analysis of variance and when a difference existed, the test of Waller Duncan at the threshold of probability 5% was used to separate these averages. The bivariate correlation of Pearson was used to determine the strength of relationship between biochemical parameters, while the Receiver Operating Characteristic (ROC) curve analysis was performed to measure the association between variations of the biochemical parameters and the infectious status of the patients.
Results
Effect of sociodemographic and clinical factors on Salmonella Typhi infection
The present study involved a population of 110 volunteers of both sexes (44 men and 66 women) with a mean age of 33.90 ± 13.42 years (Table 1). The TyphiDot® IGM and IgG test revealed 53 patients as positive for S. Typhi, giving an overall Salmonella Typhi sero-prevalence of 48.18% in the study population. From bivariate analysis, the source of drinking water was a factor significantly associated with S. Typhi infection (p = 0.045). A great proportion of participants (11/13) of those who reported to be rely on other untrusted sources of water was tested positive for S. Typhi. For other variables, although the difference between their distribution within both groups of participants, we noted that females, that were the most represented (60%) displayed high sero-prevalence (51.52%) than males (43.18%).
Liver biochemical profile of the study population
Regardless of the gender or the age, analysis of biochemical data shows that alanine aminotransferase (ALT), Alkaline Phosphatase (ALP) and Total Bilirubin (BT) levels are significantly (p < 0.05) higher in the group of S. Typhi positive patients compared to the S. Typhi negative patients (Table 2).
Because considering the average per group may hide abnormalities, we determined the prevalence of abnormalities according to S. Typhi status (Table 3). A significant association was observed between abnormality of each of the three biochemical parameters analysed and the seroprevalence of S. Typhi. All the sixteen individuals with abnormal ALT were tested positive for S. Typhi. Higher prevalences of abnormal (hyper) ALT (30.18%), ALP (69.81%) and TB (84.9%) were found among S. Typhi positive individuals than their respective negatives (0%, 5.26% and 17.54%).
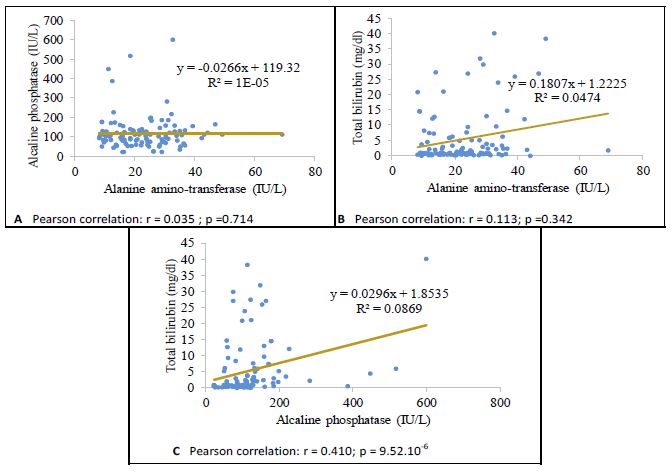
Bivariate analysis (Figure 1) of the biochemical parameters revealed no correlation between total bilirubin and ALT (r=0.113; p=0.342), as well as ALP vs ALT (r=0.035; p=0.714). However, a positive moderate correlation was observed between TB vs ALP (r=0.410, p < 0.001).
Regarding the association between biochemical parameters and the seroprevalence of S. Typhi infection, we performed the Receiver Operating Characteristic (ROC) curve analysis and summarised results in Figure 2 and Table 4. The Area Under the Curves (AUC) with their confidence intervals were above 0.5, supporting a significant association between increase in these biochemical parameters with the Typhidot sero-positivity.
Table 1: Distribution of study participants according to their Salmonella Typhi infection status in relationship to sociodemographic and clinical characteristics.
| Characteristics of participants | Category | Frequency (%) | S. Typhi positive | S. Typhi negative | Chi-Square | p-value |
|---|---|---|---|---|---|---|
| N = 110 | n (%) | n (%) | ||||
| Sex | Male | 44 (40%) | 19 (43.18%) | 25 (56.82%) | - | 0.254 |
| Female | 66 (60%) | 34 (51.52%) | 32 (48.48%) | |||
| Age range | ≤ 29 years | 55 (50%) | 25 (45.45%) | 30 (54.55%) | 0.344 | 0.842 |
| 30 – 39 years | 29 (26.36%) | 15 (51.72%) | 14 (48.28%) | |||
| ≥ 40 years | 26 (23.64%) | 13 (50%) | 13 (50%) | |||
| Marietal status | Single | 60 (54.55%) | 25 (41.67%) | 35 (58.33%) | - | 0.096 |
| Married | 50 (45.45%) | 28 (56%) | 22 (44%) | |||
| Profession | Teaching | 16 (14.55%) | 11 (68.75%) | 5 (31.25%) | 4.807 | 0.308 |
| Farming | 11 (10%) | 3 (27.27%) | 8 (72.73%) | |||
| Student | 47 (42.73%) | 22 (46.81%) | 25 (53.19%) | |||
| Housewife | 5 (4.55%) | 2 (40%) | 3 (60%) | |||
| Trader | 31 (28.18%) | 15 (48.39%) | 16 (51.61%) | |||
| Level of education | Uneducated | 52 (47.27%) | 28 (53.85%) | 24 (46.15%) | 3.834 | 0.28 |
| Primary | 6 (5.45%) | 1 (16.67%) | 5 (83.33%) | |||
| Secondary | 16 (14.55%) | 6 (37.5%) | 10 (62.50%) | |||
| University | 36 (32.73%) | 18 (50%) | 18 (50%) | |||
| Source of water | Tap | 46 (41.82%) | 19 (41.3%) | 27 (58.70%) | 8.035 | 0.045* |
| Borehole | 46 (41.82%) | 21 (45.65%) | 25 (54.35%) | |||
| Well | 5 (4.55%) | 2 (40%) | 3 (60%) | |||
| Others | 13 (11.82%) | 11 (84.62%) | 2 (15.38%) | |||
| Life style | ||||||
| Washing fruits and vegetables before consumption | 103 (93.64%) | 103 (66.03%) | 53 (33.97%) | - | 0.541 | |
| Comsumption of food and drink from street vendors | 78 (70.91%) | 78 (64.46%) | 43 (35.54%) | - | 0.191 | |
| Alcohol comsumption | 110 (100%) | 53 (48.18%) | 57 (51.82%) | |||
| Physical activity practise | 79 (71.82%) | 39 (49.37%) | 40 (50.63%) | - | 0.427 | |
| Well leather food before consumption | 107 (97.27%) | 52 (48.6%) | 55 (51.4%) | - | 0.528 | |
| Ice consumtion | 78 (70.91%) | 35 (44.87%) | 43 (55.13%) | - | 0.191 | |
| Consumtion of shellfish | 102 (92.73%) | 47 (46.08%) | 55 (53.92%) | - | 0.113 | |
| Eating with hand | 85 (77.27%) | 40 (47.06%) | 45 (52.94%) | - | 0.418 | |
| Symptoms | ||||||
| Headeache | 70 (63.64%) | 35 (50%) | 35 (50%) | - | 0.38 | |
| Constipation | 48 (43.64%) | 19 (39.58%) | 29 (60.42%) | - | 0.081 | |
| Cough | 52 (47.27%) | 24 (46.15%) | 28 (53.85%) | - | 0.416 | |
| Fever | 76 (69.09%) | 35 (46.05%) | 41 (53.95%) | - | 0.322 | |
| Diarrhea | 53 (48.18%) | 27 (50.94%) | 26 (49.06%) | - | 0.357 | |
| Digestive disorders | 55 (50%) | 26 (47.27%) | 29 (52.73%) | - | 0.5 | |
| Stomach pain | 75 (68.18%) | 33 (44%) | 42 (56%) | - | 0.14 | |
| Abdominal pain | 42 (38.18%) | 23 (54.76%) | 19 (45.24%) | - | 0.187 | |
| Anorexia | 88 (80%) | 43 (48.86%) | 45 (51.14%) | - | 0.482 | |
The corresponding p-value for 2x2 table was generated from Fisher’s Exact Test. On the same line, proportions of the S. Typhi positive group are significantly different to the S. Typhi negative group for p-values < 0.05.
Table 2: Liver biochemical parameters according to S. Typhi status.
| Liver biochemical markers | Normal values | Groups | p-value (Waller-Duncan’s test ) | |
|---|---|---|---|---|
| S. Typhi positive (n = 53) | S. Typhi negative (n = 57) | |||
| Alanine amino-transferase (ALT) | Women (< 31 IU/L) | 26.65 ± 1.74 | 18.92 ± 1.83 | 0.0021 |
| Men (< 41 IU/L) | 25.02 ± 2.33 | 21.79 ± 2.03 | 0.0742 | |
| Total | 26.06 ±1.70 | 20.30 ± 0.98 | 0.003 | |
| Alkaline phosphatase (ALP) | Children and adolescents (70 to 450 IU/L) | 198.79 ± 11.02 | 91.3± 4.17 | 0.0019 |
| Adults (30 to 125 IU/L) | 121.63 ± 13.42 | 68.6 ±7.54 | 0.0024 | |
| Total | 160.21 ± 14.78 | 80.12 ± 3.98 | 0.0046 | |
| Total bilirubin (TB) | (0.30 to 1 mg/dL) | 9.911 ± 1.42 | 1.59 ± 0.56 | 0.0001 |
On the same line, values of the S. Typhi positive group are significantly different to the S. Typhi negative group for p-values < 0.05 (Waller-Duncan’s test ).
Table 3: Distribution of biochemical abnormalities in the two groups of the study population.
| Liver biochemical markers | Variation | Groups | p-value (Fisher’s exact test) | |
|---|---|---|---|---|
| S. Typhi positive n = 53 | S. Typhi negative n = 57 | |||
| Alanine amino-transferase n (%) | Abnormal | 16 (30.18%) | 0 (0%) | 2.12.10-6 |
| Normal | 37 (69.81%) | 57 (100%) | ||
| Alkaline phosphatase n (%) | Abnormal | 37 (69.81%) | 3 (5.26%) | 1.29.10-13 |
| Normal | 16 (30.18%) | 54 (94.73%) | ||
| Total bilirubin n (%) | Abnormal | 45 (84.90%) | 10 (17.54%) | 4.03.10-13 |
| Normal | 8 (15.09%) | 47 (82.45%) |
* On the same line, values of the S. Typhi positive group are significantly different to the S. Typhi negative group.
Table 4: Summary statistics of area under the curve for the ROC analysis of ALAT, ALP and TB against S. Typhi sero-prevalence.
| Parameters | Area under the curve | Std. error | p-value | 95% Confidence Interval | |
|---|---|---|---|---|---|
| Lower bound | Upper bound | ||||
| ALAT | 0.64 | 0.054 | 0.012 | 0.534 | 0.746 |
| ALP | 0.838 | 0.04 | 1.12.10-9 | 0.76 | 0.917 |
| Total bilirubin | 0.893 | 0.035 | 1.46.10-12 | 0.825 | 0.961 |
Table 5: Multidrug resistance patterns of Salmonella Typhi isolates at Dschang District Hospital.
| Number of drugs resistant | Number of isolates (n = 18) | Resistance (%) |
|---|---|---|
| ≥ 2 | 3 | 16.66 |
| ≥ 3 | 2 | 11.11 |
| ≥ 4 | 9 | 50.00 |
| ≥ 5 | 3 | 16.66 |
| ≥ 6 | 1 | 5.55 |
Antibiotic susceptibility of isolates from the study participants
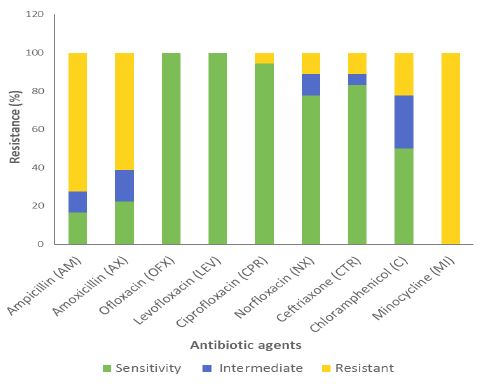
All the tested isolates of Salmonella Typhi were found sensitive to ofloxacin and levofloxacin (Figure 3). In contrast, 100%, 61.11%, 72.22%, 22.22%, 11.11%, 11.11% and 5.55% of the isolates were resistant to minocycline, amoxicillin, ampicillin, chloramphenicol, ceftriaxone, norfloxacin, and ciprofloxacin, respectively, while 27.77%, 16.66%, 11.11%, 11.11% and 5.55% of the isolates tested showed intermediate susceptibility to chloramphenicol, amoxicillin, ampicillin, norfloxacin and ceftriaxone, respectively. None of Salmonella Typhi isolates were sensitive to all antibiotics used in this study.
The presence of MDR Salmonella Typhi was observed in the study population (Table 5). Hence, 1 (5.55%), 2 (11.11%), 3 (16.66%), 3 (16.66%), and 9 (50%) of the isolates were resistant to two, three, four, five and six antibiotics tested, respectively.
Discussion
This study reports the effect of Salmonella Typhi infection on liver biochemical parameters and the in vitro antibiotic susceptibility pattern of isolates among patients visiting Dschang District Hospital in Cameroon, for medical care. The prevalence of Salmonella Typhi infection in the study population was evaluated at 48.18%. This result is higher than those obtained in other cities of Cameroon, particularly in Yaounde (34.5%), Douala (22.5%), Tiko (43%) and Bamenda (8.5%) [14,15]. Taking into account these data, it is obvious that Salmonella Typhi infection is a real public health problem in Cameroon. Nevertheless, the prevalence of S. Typhi infection obtained in the present study, is comparable to that recorded at the University hospitals of Tribhuvan (46.0%), Nepal and India [16]. These prevalences are in line with the World Health Organization [17], statement that the vast majority of typhoid fever cases occur in Asia, Africa and Latin America, where diseases transmission through results from inadequate public drinking water supply, added to poor environmental and personal hygiene. The findings of the present investigation also revealed an association between Salmonella Typhi positivity and inadequuete source of drinking water therefore consolidating the above mentioned WHO statement.
Many organs such as gastrointestinal tract, liver and heart may be involved in typhoid fever. Hepatic involvment is one of the earliest reported complications of typhoid fever [3,6,18,19]. In this study, the levels of alanine aminotransferase (26.06 IU/L), alkaline phosphatase (160.20 IU/L) and total bilirubin (9.91 mg/dL) were significantly higher in the group of S. Typhi positive patients compared to the control group. Similarly, higher prevalences of abnormal (hyper) alanine aminotransferase (30.18%), alkaline phosphatase (69.81%) and total bilirubin (84.90%) were found among S. Typhi positive individuals than their respective negatives (0%, 5.26% and 17.54%). However, the frequencies of elevated serum ALT in previous reports were 22% [20] and 100% [7,21]. Abnormal biochemical parameters (30 - 85%) suggestive of hepatic involvement have been reported in 23 - 60% cases [3,6]. It has been suggested that mild increase in liver biochemical parameters occurs in typhoid hepatitis and it could differentiate such cases from viral hepatitis where increase is marked [3,6]. However, we observed in this study, high levels of liver biochemical parameters as showed by Ayhan et al. [22]. Significant associations between S. Typhi infection and liver biochemical parameters were revealed by ROC curve analysis with AUC (95%CI) of 0.64 (0.534 - 0.746), 0.838 (0.76 - 0.917), and 0.893 (0.825 - 0.961) for Alanine Aminotransferase (ALT), Alkaline Phosphatase (ALP) and Total Bilirubin (TB), respectively. Indeed, there is an unique relationship between S. Typhi, macrophages of the liver, spleen, intestinal lymphoid follicles and mesenteric lymph nodes that could be responsible for the pathogenesis of typhoid fever. Functionally, active cytokines (TNF alpha, IL-1, alpha and beta interferons) are synthesized by macrophages and are an important source of arachidonic acid metabolites and reactive oxygen intermediate species. These products can lead to cell necrosis, recruitment of other inflammatory cells, stimulation of the immune system, vascular instability, initiation of the clotting mechanism and other abnormalities associated with typhoid fever [5]. Hepatic damage by Salmonella Typhi appears to be mediated by bacterial endotoxin [23]. Liver injury and myopathy are largely responsible for the release of the ALT enzyme. Simultaneous elevations of ALT, ALP, and TB suggest that hepatic lesions are hepatocellular and cholestatic. Further, hyper-bilirubinemia observed in patients infected with S. Typhi is due to the localization in the bile ducts of S. Typhi [24]; which causes an obstacle to the biliary flow or a malfunction of the liver which is unable to transform the free bilirubin in conjugated bilirubin so that it is excreted. The hepatocellular necrosis of the liver in typhoid fever may therefore be associated with an obstruction of the bile ducts.
Given the high frequencies of Salmonella isolates of bacterial cultures in the laboratory, and the increasing resistance of Salmonella enterica serotype Typhi to the conventional antibiotics [25], it necessary to evaluate their antibiotic susceptibility pattern. Thus, we observed various susceptibilities of 100% to ofloxacin and levofloxacin, 94.44% to ciprofloxacin; 77.77% to norfloxacin; 83.33% to ceftriaxone, 50% to chloramphenicol, 22.22% to amoxicillin, 16.66% to ampicillin, and 0% to minocycline. These results suggest that some Salmonella Typhi isolates with decreased ciprofloxacin susceptibility were still susceptible to norfloxacin, chloramphenicol and ceftriaxone. Further, the strains with decreased ciprofloxacin susceptibility were fully susceptible to broad-spectrum ofloxacin and levofloxacin which might suggest that these antibiotics could be appropriate therapy for urgent cases of typhoid fever. However, attention should be paid to the emergence of strains resistant to extended-spectrum minocycline in the near future. Previously, S. enterica serovar Typhi isolates with decreased antibiotic susceptibility have become the subject of worldwide attention [26-29]. The susceptibility of Salmonella Typhi isolates to second-generation fluoroquinolones is due to their high bactericidal activity. Indeed, after having penetrated the bacterium by diffusion, quinolones will inhibit bacterial replication by acting on the enzyme family namely topoisomerase and by exerting a rapid bactericidal effect [30,31]. The presence of fluorine in C6 position has broadened the antibacterial spectrum by significantly increasing the anti-DNA-gyrase activity and intracellular penetration of the antibiotic. Resistance of Salmonella against fluoroquinolones, minocycline, ceftriaxone, ampicillin, amoxicillin and chloramphenicol are thought to be related to misdiagnosis and misuse of common antibiotics that have led to the development and spread of multi-resistant strains of S. Typhi [32].
Differences in the susceptibility between S. Typhi isolates, and which would be related to certain particularities in their genetic constitutions, show not only that some of the test antibiotics have limited spectra of action, but also that Salmonella Typhi infections should be well diagnosed; given that two isolates of S. Typhi may have different susceptibilities to the same antibiotic. Hence, ongoing surveillance for antibiotic susceptibility remains essential, and will enhance efforts to identify resistance and attempt to limit its spread. This is all the more important because, very often, drug misuse and inappropriate treatments as well as intrinsic plasmid-mediated factors are responsible of certain forms of resistance in microorganisms [32]. The increased virulence of MDR strains may be due to the presence of other virulence genes on its R-plasmid. However, resistance may develop again if MDR strains are able to transfer their R-plasmids, which encode resistance determinants, to the strains sensitive to these drugs [28]. These findings may be of immense importance to health authorities in order to rationalise the policy of empirical treatment of typhoid fever.
The result of the present study indicates that ofloxacin (which is no longer commonly used for the treatment of typhoid fever in the study area) was found to be 100% active against the Salmonella isolates. This observation is consistent with the hypothesis that a microorganism which was previously resistant to a particular antibiotic may become sensitive if treatment with that antibiotic is suspended for a long time [33].
The findings of this study also showed that 100%, 61.11%, 72.22%, 22.22%, 11.11%, 11.11% and 5.55% of S. Typhi isolates were resistant to minocycline, amoxicillin, ampicillin, chloramphenicol, ceftriaxone, norfloxacin, and ciprofloxacin, respectively. High prevalences of resistance to aminopenicillins, phenicols, tetracyclines, and penicillins have been reported from many areas of the world [29,34]. Also, resistance of Salmonella to newer antibiotics (quinolones and extended spectrum cephalosporins) has been documented both in developing and developed countries with increasing frequency [26,28,29,35]. The mechanisms of S. Typhi resistance against antibiotics are generally mediated through plasmid and chromosomal mediations [36]. Plasmids that transfer antibiotic resistance in S. Typhi are the plasmids of incompatibility group (Inc) HI1. The mechanism of resistance of S. Typhi by chromosome mediation against fluoroquinolones is the result of the selective selection in a bacterial population following antibiotic use. The point mutation in the Quinolone Resistance Determining Region (QRDR) of the gyrA topoisomerase gene that codes for DNA gyrase is the resistance gene against fluoroquinolones [37].
Conclusion
This study provided data that further support liver disfunction through increase of biochemical parameters as a result of S. Typhi infection. Data also demonstrated the imperative need to maintain continuous monitoring of antibacterial resistance and follow a rational prescription of antibiotics based on the local antibacterial pattern. These findings advocate update on algorithm and protocol for diagnosis, monitoring and management of Salmonella enterica serovar Typhi positive patients.
Declarations
Data Availability: The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Approval: The study protocol was approved by the National Committee for Ethics in Human Health (CNERSH), Yaounde, Cameroon (ref: 2020/11/73/CE/CNERSH/SP). The research was carried out in accordance with the principles of the Helsinki Declaration.
Consent: All participants willingly provided informed consent either by signing or placing their thumbprint on the consent form.
Conflicts of Interest: The authors declare no conflicts of interest.
Authors’ contributions: TANE, JCLS and BPWT contributed to the data collection and analysis, did the biological assays and helped in manuscript writing. NNM, PGD and EDK oversed data analysis and manuscript editing. JDT designed the study, supervised and critically revised the manuscript. All authors read and approved the final version of the manuscript.
Acknowledgments : authors gratefully acknowledge all the study participants in Dschang District Hospital. We are very grateful to the Director of Dschang District Hospital, and all the nurses and laboratory personnel who took part in the study.
Funding : No funding was used in this study.
References
- F X Weill. Typhoid fever is no longer as simple to treat. Medical Sciences. 2010; 26: 969-975.
- WHO. Typhoid fever question-and-answer. http://www.who.int//features/qa/typhoid ferver / en. Accessed January 14, 2019, 2018.
- SN Khosla, R Singh, GP Singh. The spectrum of hepatic injury in enteric fever. American Journal of Gastroenterology. 1988; 83: 413-416.
- R Rajput, D Jain, A Kumar, A Mittal. ‘‘Typhoid fever presenting with acute renal failure and hepatitis simultaneously at rare presentation,’’ ARS Medica Tomitana. 2016; 2: 80-82.
- A Murinello, A Morbey, CJ Figueira, P Mendonça, AC Pires, et al. ‘‘Typhoid fever clinical and endoscopic aspects,’’ GE-Portuguese Journal of Gastroenterology. 2008; 15: 76-82.
- S Ramachandran, JJ Godfrey, MV Perera. ‘‘Typhoid hepatitis,’’ Journal of the American Medical Association. 1974; 230: 236-240.
- GM Mody, V Gathiram, EA Abdulla. ‘‘Severe reversible myopathy due to typhoid,’’ Journal of tropical medicine and hygiene. 1989; 92: 102-103.
- T Butt, RN Ahmad, A Mahmood, S Zaidi. ‘‘Ciprofloxacin treatment failure in typhoid fever case, Pakistan,’’ Emerging Infectious Diseases. 2003; 9: 1621-1622.
- AS Dajani. ‘‘Beta-lactam resistance: Minimizing the risk of therapy failure,’’ Journal of International Medical Research. 2002; 30: 1A-33A.
- C Chande, S Shrikhande, S Kapale, S Agrawal, RP Fule. ‘‘Change in antimicrobial resistance pattern of Salmonella Typhi in central India,’’ Indian Journal of Medical Research. 2002; 115: 248-250.
- JG Collee, RS Miles, B Watt. ‘‘Tests for the identification of bacteria,’’ In: J. G. Collee, A. G. Fraser, B. P. Marmion and A. Simmons, editors. Mackie and McCartney Practical medical microbiology. 14th ed. London: Livingstone. 1996; 131-149.
- Clinical and Laboratory Standards Institute (CLSI), ‘‘Performance Standards for Antimicrobial Disk Susceptibility Tests,’’ CLSI, Wayne, PA, USA. 2012.
- Clinical and Laboratory Standards Institute (CLSI), ‘‘Performance Standards for Antimicrobial Susceptibility Testing: Twenty Fifth Informational Supplement M100-S23,’’ CLSI, Wayne, PA, USA. 2015.
- EF Nsutebu, P Martins, D Adiago. ‘‘Prevalence of typhoid fever in patients with compatible symptoms in Cameroon,’’ Tropical Medicine & International Health. 2003; 8: 575-578.
- A Nkeza, M Kengne, NM Julius, TD Goon, PA Njukeng. ‘‘The susceptibility pattern of Salmonella species to commonly used antibiotics in the Bamenda district health area, Cameroon,’’ African Journal of Pathology and Microbiology. 2016; 5: 14-17.
- CP Bhatta, KC Bhuyan, A Maharjan. ‘‘The study, antibiotic sensitivity pattern of Salmonella species isolated from blood culture,’’ Journal of the Nepal Health Research Council. 2005; 3.
- World Health Organization, ‘‘Typhoid Vaccine (Initiative for Vaccine Research),’’ WHO, Geneva, Switzerland. 2010.
- S Amen, S Ayesha, H Bilal. ‘‘Study of biochemical changes and elevated levels of enzymes in Salmonella typhi infected patients in Pakistani population,’’ International Journal Bioautomation. 2012; 16: 33-42.
- MM Ibrahim, A Salihu, FI Dugje. ‘‘Typhoid fever and liver enzyme activity,’’ International Journal of Research. 2015; 2: 656-662.
- M Mirsadraee, A Shirdel, F Roknee. ‘‘Typhoid myopathy or typhoid hepatitis: A matter of debate,’’ Indian Journal of Medical Microbiology. 2007; 25: 351-353.
- R Morgenstern, PC Hayes. ‘‘The liver in typhoid fever: Always affected, not just a complication,’’ American Journal of Gastroenterology. 1991; 86: 1235-1239.
- A Ayhan, A Gokoz, S Karacadag. ‘‘The liver in typhoid fever,’’ American Journal of Gastroenterology. 1973; 59: 141-146.
- C Pramoolsinasp, V Viranuvatti. ‘‘Salmonella hepatitis,’’ Journal of Gastroenterology and Hepatology. 1998; 13: 745-751.
- B Marchou, JJ Meurisse. ‘‘Salmonellosis: therapeutic aspects,’’ Med Infect Dis. 1992; 22: 340-347.
- VC Chauvin. ‘‘Antibiotic use and bacterial resistance in poultry farming,’’ PhD Thesis, University Rennes. 2009; 1: 25.
- K Hirose, K Tamura, H Sagara, H Watanabe. ‘‘Antibiotic susceptibilities of Salmonella enterica serovar Typhi and S. enterica erovar Paratyphi isolated from patients in Japan, Antimicrobial Agents and Chemotherapy. 2001; 45: 956-958.
- U Madhulika, BN Harish, SC Parija, ‘‘Current pattern in antimicrobial susceptibility of Salmonella Typhi isolates in Pondicherry,’’ Indian Journal of Medical Research. 2004; 120: 111-114.
- Y Kumar, A Sharma, KR Mani. ‘‘Antibiogram profile of Salmonella enterica serovar Typhi in India-A two year study,’’ Tropical Life Sciences Research. 2013; 24: 45-54.
- MA Rahman. ‘‘Antimicrobial resistance patterns of Salmonella Typhi isolated from stool culture,’’ Chattagram Maa-O-Shishu Hospital Medical College journal. 2015; 14: 26-30.
- PC Appelbaum, PA Hunter. ‘‘The fluoroquinolone antibacterial: past, present and future perspectives,’’ International Journal of Antimicrobial Agents. 2000; 16: 5-15.
- PMJ Hawkey. ‘‘Mechanisms of quinolone action and microbial response,’’ Antimicrobial Chemotherapy. 2003; 51: 29-35.
- NU Adabara, BU Ezugwu, A Momojimoh, A Madzu, Z Hashiimu, et al. ‘‘The prevalence and antibiotic susceptibility pattern of Salmonella Typhi among patients attending a military hospital in Minna, Nigeria,’’ Advances in Preventive Medicine. 2012; 10: 1-4.
- EJ Threlfall, LR Ward. ‘‘Decreased susceptibility to ciprofloxacin in Salmonella enterica serotype Typhi, United Kingdom,’’ Emerging Infectious Diseases. 2001; 7: 448-440.
- LH Su, CH Chiu, C Chu, JT Ou. ‘‘Antimicrobial resistance in nontyphoid Salmonella serovars: A global challenge,’’ Clin Infect Dis. 2004; 39: 546-551.
- G Mijovic, B Andric, D Terzic, M Lopicic, B Dupanovic. Antibiotic susceptibility of Salmonella spp: A comparison of two surveys with a 5 years interval. Journal of IMAB Annual Proceeding. 2012; 18: 216-219.
- SA Zaki, S Karande. ‘‘Multidrug-resistant typhoid fever: A review, J Infect Dev Countr. 2011; 5: 324-337.
- KE Holt, NR Thomson, J Wain, MD Phan, S Nair, et al. ‘‘Multidrug-resistant Salmonella enterica serovar Paratyphi A harbors IncHI1 plasmids similar to those found in serovar Typhi,’’ Journal of Bacteriology. 2007; 189: 4257-4264.