
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A rare case of both primary and secondary intrathoracic goiters
Clément Dhainaut1*; François Montagne1; Guelareh Dezfoulian2; Lotfi Benhamed1
1Department of Thoracic Surgery, Valenciennes Hospital, Valenciennes, France.
2Department of Endocrine and Visceral Surgery, Valenciennes Hospital, Valenciennes, France.
*Corresponding Author : Clément Dhainaut
Department of Thoracic Surgery, Valenciennes
Hospital, Valenciennes, France.
Email: dhainaut-c@ch-valenciennes.fr
Received : Jun 01, 2023
Accepted : Jul 14, 2023
Published : Jul 21, 2023
Archived : www.jcimcr.org
Copyright : © Dhainaut C (2023).
Abstract
Primary intrathoracic goiter is a very rare entity representing only 1% of all intrathoracic goiters. It arises from mediastinal ectopic thyroid, without tissue connection with cervical thyroid and its blood supply is entirely derived from intrathoracic vessels. Secondary intrathoracic goiter is a much more common condition. It results from the intrathoracic extension of a cervical goiter which draws its vascularization from cervical vessels.
We report here the case of a 47-year-old women presenting both primary and secondary intrathoracic goiter compressing the trachea and the esophagus and causing compressive symptoms.
The complete surgical resection was performed by a sequential approach with a cervicotomy and a right lateral thoracotomy. This sequential approach allowed us to perform a safe resection with the control of the mediastinal vessels through the thoracotomy.
Keywords: Intrathoracic goiter; Primary intrathoracic goiter; Ectopic thyroid; Mediastinum.
Abbreviations: PIG: Primary intrathoracic goiter; SIG: Secondary intrathoracic goiter; ETT: Ectopic thyroid tissue.
François Montagne: https://orcid.org/0000-0001-8182-2695
Citation: Dhainaut C, Montagne F, Dezfoulian G, Benhamed L. A rare case of both primary and secondary intrathoracic goiters. J Clin Images Med Case Rep. 2023; 4(7): 2509.
Introduction
Primary Intrathoracic Goiter (PIG) is a very rare entity resulting from hypertrophy of a mediastinal ectopic thyroid affected by multinodular disease. Arising from an ectopic thyroid, PIG has no tissue connection with the cervical thyroid and its blood supply derives entirely from intrathoracic vessels. Surgical management is recommanded to prevent complications associated with the development of PIG including compression of adjacent structures and risk of carcinogenesis.A thoracic approach is often mandatory to ensure a complete resection with a safe control of the mediastinal vascularization [1].
On the opposite, Secondary Intrathoracic Goiter (SIG) is a much more frequent condition representing 99% of all intrathoracic goiters. It results from the intrathoracic extension of a goiter arising from an orthotopic cervical thyroid and occurs in 10-15% of all goiters. The blood supply derives from cervical vessels and the resection can be performed by cervicotomy in 99 % of cases [1,2].
PIG associated to SIG is a very rare condition and we report here the case of a 47-year-old woman presenting symptomatic PIG and SIG completely resected by a sequential cervicotomy and lateral thoracotomy approach.
Case presentation
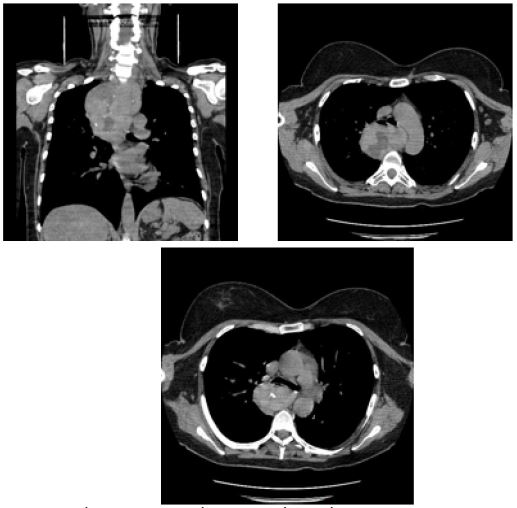
A 47-year-old woman was referred to an endocrine surgeon for management of a compressive multinodular goiter. She was followed by an endocrinologist for hyperthyroidism successfully treated by carbimazol. Over the last 3 months, she has progressively developped compressive symptoms and presented resting dyspnea associated with a permanent feeling of cervical compression. Clinical examination and ultrasonography showed an enlarged and multinodular thyroid extending beyond the manubrium. Chest CT-scan (Figure 1) revealed a multinodular cervical goiter associated with a large posterior mediastinal mass. The mediastinal mass occupied the upper two-thirds of the mediastinum and extended beyond the carena. It had closed relationships with the aortic arch and the brachiocephalic trunk. The esophagus and the trachea were compressed and deviated forward. From the upper pole of the thyroid to the lower edge of the mediastinal mass, the total height was 16 centimeters. Both lesions had the same pattern of heterogeneous content associated with calcifications. A detailed analysis of the CT-scan revealed no thyroid tissue between the cervical and thoracic lesions.
The surgical indication was retained because of the patient’s symptomatic condition. A sequential cervical and thoracic approach involving both endocrine and thoracic surgeons was planned. This sequential approach was indicated to perform a safe resection of the two distincts lesions. The thoracic approach allows the intrathoracic lesion to be resected while controlling its vascular supply, which is not possible with cervicotomy. The endocrine surgeon managed to resect a well-encapsulated cervical goiterby cervicotomy (Figure 2). The upper border of the mediastinal mass was palpable through the cervicotomy without any connection with the removed cervical goiter. The thoracic surgeon performed a right exploratory videothoracoscopy and attempted to resect the mediastinal mass. Given the hemorrhagic nature of this large lesion compromising safe dissection, a lateral thoracotomy was performed and allowed for complete resection of a well-encapsulated mass and ligation of the feeding vessel arising from an intercostal vessel (Figure 3). By this sequential approach a complete and safe resection was performed. Postoperative recovery was uneventful and the patient was discharged from hospital after 5 days.
The histopathological examination revealed the same diagnosis of well-encapsulated multinodular goiter without malignancy in the two specimens and therefore confirmed the diagnosis of both PIG and SIG.


Discussion
Ectopic Thyroid Tissue (ETT) is defined as thyroid tissue located in an other site than its pretracheal anatomical location between the third and the fifth tracheal ring. It is a rare entity occuring in 1/100 000 to 1/300 000 in general population.
Lingual ectopic thyroid is by far the most common condition representing 90% of all ETT but many other various sites are described. ETT can be found anywhere along the path of embryologic migration of the thyroid anlage from the foramen caecum at the base of the tongue to its final pretracheal position in the neck. These ectopic locations result from a prematured arrest of migration of the thyroid anlage. Distant ectopic sites include the mediastinum, heart, aorta, lungs, esophagus and even subdiaphragmatic organs such as the duodenum, gallbladder or adrenal glands [3].
Mediastinal ETT is extremely rare, accounting for only 1 % of all ETT and 1 % of all mediastinal masses [4,5]. It results from an excess of embryologic migration of a part of the thyroid anlage that is dragged into mediastinum by the caudal migration of the heart [1] or from aberrant differentiation of mediastinal pluripotent cells [6]. Mediastinal ETT can be affected by any thyroid disease. Several cases of PIG have been reported, mainly in the anterosuperior mediastinum [4,5,7] but rarely in the posterior mediastinum [8]. Exceptionnally, cases of malignancy [9] and Graves’ disease [10] have been described.
PIG are often diagnosed incidentally in euthyroid and asympomatic patients. Infrequently, patients develop symptoms related to the compression of the surrounding organs by the growing goiter as it was for our patient. Possible symptoms include dry cough, dyspnea, dysphagia, hoarseness or superior vena cava syndrome. Malignancy, tracheomalacia and acute respiratory obstruction due to spontaneous or traumatic bleeding are other serious complications leading many authors to recommend surgical resection for all PIG [1,4,7].
On CT-scan PIG is often described as an heterogeneous mediastinal mass with calcifications with the same tone as the orthotopic thyroid. In case of incidental finding, some authors recommend a thyroid scintigraphy or even a tissue biopsy guided by CT-scan or by endobronchial or endoesophagial echoendoscopy to confirm the thyroidal nature of the lesion [1,4,7]. In our patient’s case, no further investigation was necessary and surgical resection was indicated for both diagnosis and treatment of disabling compressive symptoms.
Historically sternotomy was preferred for PIG located in the anterosuperior mediastinum [4,5,7] and thoracotomy for PIG in the posterior mediastinum [8]. Nowadays, minimally invasive approaches as videothoracoscopy and robotic-assisted surgery have been reported with better short-term outcomes compared to open approaches [6]. In our patient’s case, the sequential approach was indicated because the pre-operative CT-scan suggested the presence of 2 distincts lesions with the thoracic mass vascularized by mediastinal vessels. No one of the single approach could therefore allow to perform a safe and complete resection. Minimally invasive approach by videothoracoscopy was preferred but unfortunately, continuous bleeding during the dissection required conversion to thoracotomy to perform a complete and safe resection of the large hemorrhagic mediastinal mass. Nevertheless, conversion to thoracotomy did not compromise post-operative outcomes of our patient.
Conclusion
Intrathoracic goiters are often SIG. Although very rare, PIG should be kept in mind because the control of their intrathoracic vascularization requires a planned multidisciplinary and sequential approach involving both endocrine and thoracic surgeons.
References
- Foroulis CN, Rammos KS, Sileli MN, Papakonstantinou C. Primary intrathoracicgoiter: A rare and potentially serious entity. Thyroid. 2009; 19: 213-218.
- Polistena A, Sanguinetti A, Lucchini R, Galasse S, Monacelli M, et al. Surgicalapproach to mediastinalgoiter: An update based on a retrospectivecohortstudy. Int J Surg. 2016; 28: S42-S46.
- Noussios G, Anagnostis P, Goulis DG, Lappas D, Natsis K, et al. Ectopicthyroid tissue: Anatomical, clinical, and surgical implications of a rare entity. Eur J Endocrinol. 2011; 165: 375-382.
- Regal M, Kamel MM, Alyami H, Al-Osail EM. Media stinalectopic thyroid mass with normal thyroidfunction and location: Case report. Int J Surg Case Rep. 2018; 52: 5-7.
- Raji Y, Gupta S, Pucar D, Keshavamurthy JH. Ectopicthyroid: The greatmimicker. Lung India. 2018; 35: 248-250.
- Haddad R, Bussade I, Henrique Ferreira C, Mingarini Terra R, Braga F, et al. Symptomatic Ectopic Middle Mediastinal Thyroid Resected by Robotic Thoracic Surgery - Case Report. World J Surg Surgical Res. 2020; 3: 1194.
- El Oueriachi F, El Hammoumi MM, Arsalane A, Slaoui O, Diouri H, Kabiri EH, et al. Primary mediastinalgoiters. Springer Plus. 2014; 3: 503.
- Chaudhry IU, Cheema AI, AlShamasi Z, Mutairi H. Hoarseness of voice, respiratory distress and dysphagia due to giant primary posterior mediastinal ectopicgoitre: A rare clinicalentity. BMJ Case Rep. 2016; 2016: bcr2016215132.
- Shah BC, Ravichand CS, Juluri S, Agarwal A, Pramesh CS, Mistry RC, et al. Ectopic Thyroid Cancer. Ann Thorac Cardiovasc Surg. 2007; 13: 122-124.
- Gorur GD, Isgoren S, Tan YZ, Utkan Z, Demir H, et al. Graves’ disease in a patient with ectopicmediastinal thyroid. Clin Nucl Med. 2011; 36:1039-1040.