
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 4
Sheehan syndrome: Clues to underlying diagnosis
Saurav Shishir Agrawal1*; Shobhit Bhardwaj2
1Consultant Endocrinology, Yatharth Superspeciality Hospital, Noida (UP), India.
2Consultant Orthopedics, YatharthSuperspeciality Hospital, Noida (UP), India.
*Corresponding Author : Saurav Shishir Agrawal
Consultant Endocrinology, Yatharth Superspeciality Hospital, Noida (UP), India.
Email: docssagrawal@gmail.com
Received : Jun 05, 2023
Accepted : Jul 14, 2023
Published : Jul 21, 2023
Archived : www.jcimcr.org
Copyright : © Agrawal SS (2023).
Abstract
As Hypoglycemic disorders are rare in patients without Diabetes Mellitus, a thorough evaluation should be performed only in individuals presenting with Whipple’s Triad (Symptoms or signs consistent with hypoglycaemia, a low reliably measured plasma glucose concentration and resolution of these symptoms after plasma glucose is raised). In a seemingly Ill-looking individual, hormonal deficiencies including Cortisol and thyroid should be ruled out after excluding more common causes such as drugs and critical illnesses.
Keywords: Hypoglycemia; Hyponatremia; Cortisol.
Citation: Agrawal SS, Bhardwaj S. Sheehan syndrome: Clues to underlying diagnosis. J Clin Images Med Case Rep. 2023; 4(7): 2510.
Case details
A 46-year-old lady presented to the emergency department with sweating, palpitations, and tremors for the last fifteen minutes. Her plasma glucose was documented to be 46 mg/dl (reference range – 70-180 mg/dl) in emergency. Her Symptoms resolved after the administration of 25% dextrose solution. She had a recent history of low trauma fracture of the neck of the femur. There was no history of Anti-diabetic agents or insulin use in the past. There was a history of traumatic delivery twelve years back, which was followed by secondary amenorrhea and loss of secondary sexual characteristics. Physical examination revealed a pale-alabaster-looking skin, wrinkled face, loss of lateral eyebrows (Figure 1), and hoarse voice. Blood pressure was 92/60 mm Hg while pulse rate was 56/minute at presentation.
Laboratory studies showed Glycated hemoglobin of 5.3%, serum sodium - 128 mEq/L , low free T4 - 0.2 ng/dl with normal TSH of 2.2 mIu/ml and low serum cortisol - 1.5 mcg/dl. Other parameters of anterior pituitary function including, ACTH, Prolactin, IGF-1, were also low. LH and FSH were inappropriately normal for menopausal age.
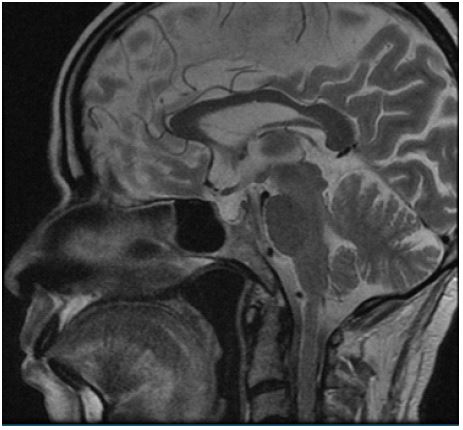
MRI of the pituitary revealed an Empty sella with thinned-out anterior pituitary (Figure 2). A diagnosis of Sheehan syndrome was made and she was started on intravenous dextrose containing fluids with hydrocortisone supplementation followed by thyroxine replacement. After 6 weeks of follow-up, her serum sodium had improved and there was no new episode of hypoglycaemia.

Discussion
Sheehan syndrome occurs due to ischemic pituitary necrosis induced by vasospasm and thrombosis of hypophyseal arteries [1]. In Sheehan syndrome, Hypoglycaemia can occur due to secondary adrenal insufficiency associated with loss of counter-regulatory hormones like Growth Hormone while hypothyroidism and cortisol deficiency decrease free water clearance and cause subsequent hyponatremia [2]. Low bone mineral density occurs due to long-standing estrogen deficiency.
Pale-alabaster-looking-skin occurs due to loss of ACTH and pro-opiomelanocortin related peptides and subsequent decreased stimulation of the skin MC1 receptor and is a clue to the underlying secondary adrenal insufficiency [3]. The loss of lateral one third of eyebrows known as “Hertoghe Sign” occurs in hypothyroidism due to increased apoptosis of hair follicles [4].
Central hypoadrenalism and hypothyroidism should always be suspected in patients presenting with unexplained hypoglycaemia and hyponatremia in emergency.
Acknowledgements: None.
References
- Kovacs K. Sheehan syndrome. Lancet. 2003; 361: 520–522.
- Adewiah S, Syukri M, Zufry H, Sucipto KW. Unusual Presentation of Sheehan’s Syndrome with Severe Hyponatremia and Recurrent Symptomatic Hypoglycemia: A Case Report. Journal of the ASEAN Federation of Endocrine Societies. 2016; 31: 166.
- Arlt W, Allolio B. Adrenal insufficiency. Lancet. 2003; 361: 1881-1893.
- Leonhardt JM, HeymannWR.Thyroid disease and the skin. (vii). Dermatol Clin. 2002; 20: 473–481.