
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A case of familial mediterranean fever in an elderly patient experiencing recurrent fever and weigh loss
Seiji Yamashiro, MD, MS1,2; Keiichiro Kita, MD, PhD1; Hideki Niimi, MD, PhD3
1Department of General Medicine, Toyama University Hospital, Toyama, Japan.
2Department of General Medicine and Internal Medicine, Asahi General Hospital, Toyama, Japan.
3Department of Clinical Genetics, Toyama University Hospital, Toyama, Japan.
*Corresponding Author : Seiji Yamashiro
Department of General Medicine, Toyama University Hospital, Toyama, Japan.
Email: seiji-yamashiro@clock.ocn.ne.jp
ORCID: 0000-0002-5643-5762
Received : Jul 01, 2023
Accepted : Jul 20, 2023
Published : Jul 27, 2023
Archived : www.jcimcr.org
Copyright : © Yamashiro S (2023).
Abstract
Familial Mediterranean Fever (FMF) is a rare hereditary autoinflammatory disease. In particular, the onset is rare in the elderly, and the symptoms are atypical, making diagnosis difficult. A 61-year-old man was referred to our hospital due to recurrent fever and weight loss 3 months ago. Prior to his visit, he had a temporomandibular disorder and right hip arthritis, in addition to a fever, and had visited several medical departments. Infection- and rheumatism-related examinations were performed for fever and systemic malignant diseases were examined for weight loss; however, the causes were unknown. FMF was suspected based on a 3-month fever pattern chart at the time of consultation. It is important to suspect FMF in patient with fever of unknown cause, even in atypical cases of elderly -onset (over 60 years of age).
Keywords: Familiar Mediterranean fever; Elderly patients; Atypical symptoms; Important of suspicion.
Abbreviations: CT: Computed tomography; FEMV gene: Familiar Mediterranean fever gene; FMF: Familiar Mediterranean fever.
Citation: Yamashiro S, Kita K, Niimi H. A case of familial mediterranean fever in an elderly patient experiencing recurrent fever and weigh loss. J Clin Images Med Case Rep. 2023; 4(7): 2518.
Introduction
Familial Mediterranean Fever (FMF) is a hereditary autoinflammatory disease characterized by periodic fever and aseptic arthritis. Its incidence is high in the Mediterranean region and its surrounding areas. Although it is a rare disease in Japan, the number of reports has increased in recent years owing to the sharing of disease information and advances in genetic testing. FMF has a juvenile onset, with approximately 90% of patients diagnosed before the age of 20. In 10% of adult-onset cases, atypical presentations are common, and diagnosis is often delayed, especially in older patients [1].
We report the case of a 61-year-old male patient with FMF who was referred for recurrent fever and weight loss. We investigated the reasons for this delay in diagnosis in elderly patients and reported on them.
Case presentation
A-61-year-old Japanese man was referred to our department from a nearby general hospital with recurrent fever, hip arthritis, and weight loss. Approximately 3 months prior, he visited the internal medicine department at a nearby general hospital with a fever of unknown cause. Two and a half months ago, he visited the internal medicine department again because of a fever, and was unable to make a diagnosis based on whole-body computed tomography (CT), a negative anti-nuclear antibody, and two sets of blood cultures. Two months ago, he visited another hospital with right hip pain and was diagnosed with hip bursitis based on CT findings, CRP of 7 mg/dL, and WBC of 12,000/μL. At this time, he was suspected of having rheumatoid arthritis and visited the orthopedics department and the department of collagen disease at a nearby general hospital. At the time of presentation, his joint symptoms had disappeared and his inflammatory reaction was negative. He searched for malignancies during a weight-loss workup. Gastroscopy revealed esophageal Candida, a hiatal hernia, and fundic gland polyps. A colonoscopy revealed colonic polyps, and endoscopic mucosal resection was performed. Ga scintigraphy revealed uptake in the right hip joint but no abnormal uptake at other sites.
Since the cause of the recurrent fever and weight loss was unknown, he was referred to our department for examination 3 months after symptom onset. His weight loss was 9 kg over 3 months (range, 60–51 kg).
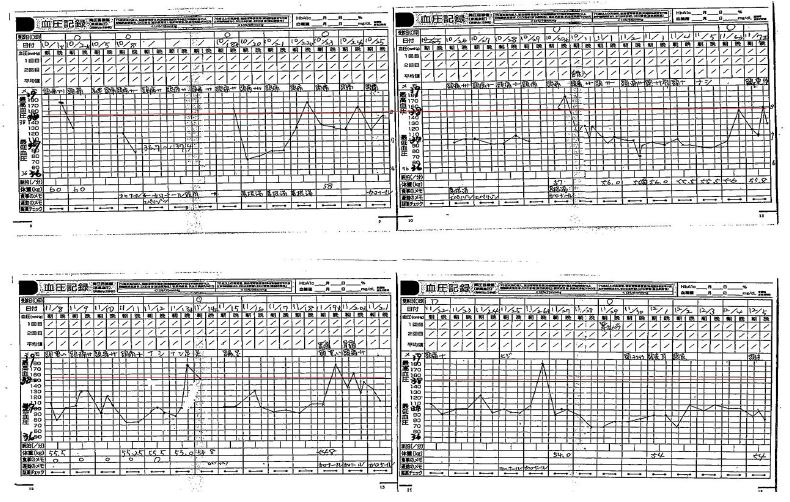
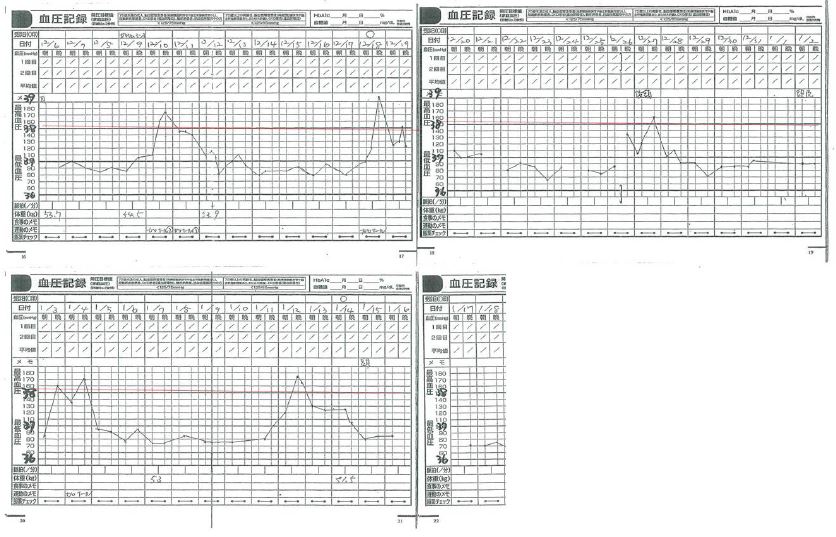
On the first day of the consultation, the patient had no fever or joint pain. The patient presented with a 3-month fever (Figures 1a, b). A fever of 38oC or higher lasted for 1-2 days, with an intermittent period of 6-7 days. He lost his appetite when he developed a fever, and he continued to feel malaise for 2-3 days after the fever subsided. Past medical history included appendicitis surgery at the age of 22 and no family history.
Vital signs: Blood pressure; 119/79 mmHg, pulse, 109 beats per minute; body temperature, 37.4°C; height, 165 cm; and weight, 51.7 kg. His chest, abdomen, and neurological findings were unremarkable. Blood tests showed no particular abnormality except for CRP at 0.25 mg/dL. Thyroid function was normal. Chest radiography showed no cardiomegaly, and electrocardiography showed sinus tachycardia (HR 101/min). Whole-body positron emission tomography/CT revealed no abnormalities. No malignancies that led to weight loss were observed.
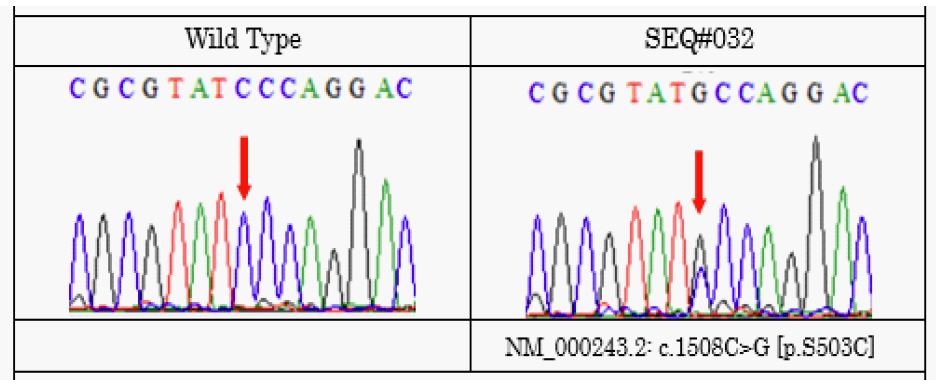
The FMF was suspected based on a history of recurrent fevers, arthritis (temporomandibular disorder and right hip arthritis), and regular periodic fever patterns. However, since we had never encountered a case of FMF, we decided to make the diagnosis based on an article by Kishida et al. [2]. There were two major criteria in the Livneh diagnostic criteria, and FMF was strongly suspected; therefore, we decided to observe the patient’s response to colchicine. For genetic testing, we consulted a doctor in the Department of Clinical Genetics and obtained patient consent for Mediterranean fever (MEFV) gene testing. Treatment with colchicine (1 mg/day) was initiated. As for the response to colchicine, the frequency of a fever of 38°C or higher was once every 2 weeks, the duration was one day, and the general condition improved, showing a favorable response. Approximately 2 months later, MEFV genetic testing revealed a heterozygous Ser503Cys (TCC→TGC) mutation in exon 5 (Figure 2). FMF was confirmed based on patient history, colchicine response, and MEFV gene mutation. Subsequently, colchicine was increased to 1.5 mg/day. The frequency of fever decreased to once per month, and 8 months later, fever above 38°C was not observed. One year later, a fever of 37°C or higher disappeared.
Discussion
FMF is a rare hereditary autoinflammatory disease that causes recurrent fever, peritonitis, synovitis, and pleurisy and responds well to colchicine. Overall, 90% of patients have an onset before the age of 20 years and 65% before the age of 10 years [1]. Adult-onset is in 10% of patients, and elderly-onset (over 60 years of age) is extremely rare. Elderly patients present with atypical presentations, mild fevers, and coexisting illnesses that delay diagnosis [3,4]. Tanosaki et al. reported a case in which diagnosis took more than 30 years due to patients with psychiatric disorders and physicians’ lack of knowledge of FMF, and other studies reported a delay from onset to diagnosis of 9.1–11.5 years [5-7]. Non-focal peritonitis is reported to be difficult to distinguish from pelvic inflammatory disease and Fitz-Hugh-Curtis syndrome in gynecology [7-9].
In this case, from onset to diagnosis, the patient initially visited an otolaryngologist and an oral surgeon for temporomandibular joint disorder and an orthopedic surgeon for hip joint pain. In addition, because of the weight loss, a full-body examination was performed; however, the cause was not investigated. The 3 month pattern of fever was a fever over 38 °C that lasted for 1-2 days about once a week, and the symptoms and inflammatory findings were relieved during the intermittent period, showing a typical periodic fever. Based on careful history-taking, we strongly suspected FMF.
As it is a rare disease, it was necessary to search the literature for its diagnosis. In addition, genetic testing requires advice from specialists. Applying the diagnostic criteria, colchicine was administered as a diagnostic treatment, and MEFV genetic testing was performed concurrently, leading to a diagnosis.
Autoinflammatory diseases are said to be the fourth most common fever of unknown origin after the three major fevers of unknown origin (infectious diseases, malignant diseases, and collagen diseases). Migita et al. reported a high frequency of FMF as a cause of unexplained fever and nonspecific rheumatic symptoms [10]. FMF is the most common autoinflammatory disease, and knowledge of its characteristics facilitates its diagnosis. MEFV genetic testing shows that the complete type has many mutations in exon 10, whereas the incomplete type has few mutations in exon 10 and is often associated with mutations in exons 1, 2, 3, and 5 [2]. Endo et al. reported that the late-onset group aged 40 years in Japan had fewer exson10 mutations and more arthritis and myalgia than those aged < 40 years [11]. Our 61-year-old patient had an exon 5 mutation that was associated with a temporomandibular disorder and hip arthritis.
In Japan, MEFV genetic testing has been covered by insurance since 2020 and can be outsourced, making it easier to genetically diagnose FMF as a rare disease. Therefore, suspicion should be based on the patient’s medical history. In addition, early administration of colchicine is important to prevent amyloidosis, which can cause organ damage.
Conclusion
FMF is a rare hereditary autoinflammatory disease. Diagnosis is more difficult in older patients; however, knowledge of their typical history and findings is the first step in managing atypical cases. As the genetic diagnosis of MEFV has become easier, early diagnosis and treatment have become increasingly important.
Declarations
Authors contributions: SY reviewed the literature and drafted the manuscript. KK critically reviewed the manuscript. HN consulted for MEFV analysis and critically reviewed the manuscript.
Acknowledgements: We would like to thank Editage (www.editage.com) for English language editing.
Patient consent: Consent was taken from the patient.
Funding source: Not applicable.
Conflicts of interest: No competing interests.
References
- Lancieri M, Bustaffa M, Palmeri S, Prigione I, Penco F, Para R, et al. An Update on Familial Mediterranean Fever. Int J Med Sci. 2023; 24: 9584.
- Kishida D, Yazaki M, Nakamura A. Diagnosis and Treatment of Familial Mediterranean Fever. Shinshu Med J. 2019; 67(4): 229-240.
- Takahashi S, Ito S, Mizoguchi A, Nishii S, Wada A, Furuhashi H, et al. A typical clinical presentation of familial Mediterranean fever resembling colonic diverticulitis in an elderly patient: a case report. J of JSGE. 2020; 117(11): 978-984.
- Yamashita K, Mizugishi K, Takaori-Kondo A. Familial Mediterranean Fever Mutations in a Patient with Periodic episodes of Systemic Pain Deriving from Cancer Bone Metastases. Intern Med. 2018; 57: 2901-2904.
- Tonosaki K, Yonenaga K, Itai S, Mizuno T, Oyama S. Familial Mediterranean Fever with Psychiatric Disorder which Have not Been Diagnosed over 30 Years: A Case report. Tokai J Exp Clin Med. 2021; 46(4): 180-183.
- Migita K, Agematsu K. Clinical aspects of Familial Mediterranean fever. Jpn J Clin Immunol. 2011; 34(5): 355-360.
- Kunimatsu J, Maeda J, Watanabe R, Kato O, Kishida D, Mazaki M, et al. Fever of unknown origin in the outpatient setting: A retrospective analysis of 30 cases of familial Mediterranean fever. Jpn J Clin Immunol. 2016; 39(2): 130-139.
- Adair R, Colon J, McGovern PG. Familial Mediterranean fever presenting as recurrent acute pelvic inflammatory disease. Obstet Gynecol. 2003; 101(5): 1098-1100.
- Romero-Gomez M, Corpas R, Sanchez-Munoz D, Grande L. Familial Mediterranean Fever Mimicking Fitz-Hugh-Curtis Syndrome. Am J Gastroenterol. 2003; 98: 701.
- Migita K, Izumi Y, Jiuchi Y, Iwanaga N, Kawahara C, Agematsu K, et al. Familial Mediterranean fever is no longer a rare disease in Japan. Arthritis Res Ther. 2016; 18: 175.
- Endo Y, Koga T, Ishida M, Fujita Y, Tsuji S, Takatani A, et al. Musculoskeletal manifestations occur predominantly in patients with later-onset familial Mediterranean fever: Date from a multicenter, prospective national cohort study in Japan. Arthritis Res Ther. 2018; 20: 257.