
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 4
Restricted diffusion in the corpus callosum: Marchiafava-Bignami disease
*Corresponding Author : El Amrani Soukaina
Radiology Department, National Institute of
Oncology, Ibn Sina Hospital, Mohammed V
University, Rabat, Morocco.
Email: drsoukainael@gmail.com
Received : Jul 06, 2023
Accepted : Jul 21, 2023
Published : Jul 28, 2023
Archived : www.jcimcr.org
Copyright : © Soukaina ElA (2023).
Abstract
Marchiafava-Bignami disease (MBD) is a very rare demyelinating/necrotic disorder of the corpus callosum and nearby subcortical white matter, seen mostly in chronic alcoholics. We present here the magnetic resonance imaging findings of Machiafava-Bignami disease in a 75-year-old man with a history of untreated diabetes mellitus who presented with a sudden onset of alteration in speech and multiple falls in a few days.
Keywords: Marchiafava-Bignami disease; Diabetes mellitus; Corpus callosum; Magnetic resonance imaging.
Citation: Soukaina EA. Restricted diffusion in the corpus callosum: Marchiafava-Bignami disease. J Clin Images Med Case Rep. 2023; 4(7): 2520.
Introduction
Marchiafava-Bignami disease (MBD) is a rare disorder of unknown etiology [1] that is particularly prevalent in alcoholics suffering from malnutrition but can also occur in patients with metabolic disorders [2]. The symptomatology is non-specific [3] and includes a variety of psychiatric symptoms, including dementia, aphasia, seizures, heightened muscle tone, tremor, paralysis, stupor, and coma.
The diagnosis is based on Magnetic Resonance Imaging (MRI) imaging that shows hyperintense lesions without significant mass effect within the corpus callosum that may extend to adjacent white matter on T2WI, FLAIR, and DWI [4].
Case presentation
A 75-year-old man was admitted to the neurology department for dysarthria, apraxia, and gait disorders. A neurological examination showed dysarthria, ataxy, and left central facial palsy. With no history of previous alcoholism or malnutrition and no comorbidities, the patient was newly diagnosed with diabetes during hospital admission.
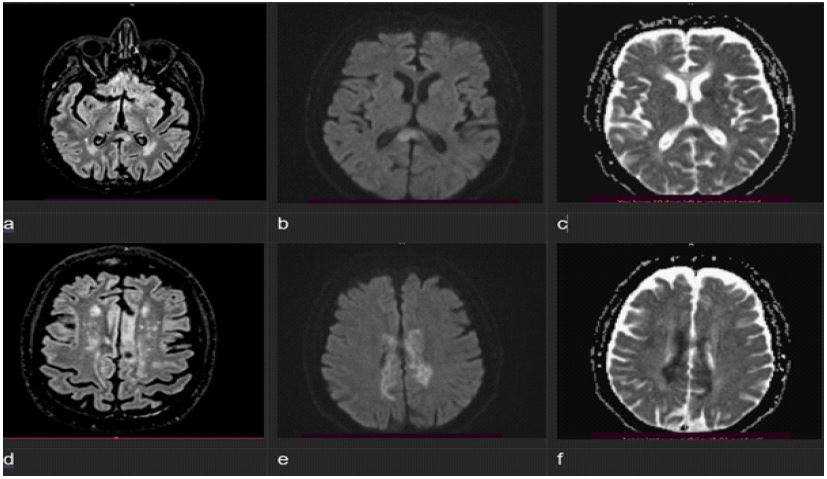
Blood analysis revealed a glycemic level of 455mg/dL and glycated hemoglobin of 10%. Cerebral magnetic resonance imaging (MRI) showed anomalies in the corpus callosum, more pronounced in its central region and appearing as hyperintensities in T2-weighted, FLAIR (Figure 1), and diffusion sequences.
Discussion
MBD is still recognized as a rare disorder with no typical symptoms, seen typically in alcoholic or malnourished patients [5]. Only a few isolated cases of MBD in non-alcoholic diabetics have been reported.
The pathological mechanism of MBD has not been fully elucidated but can be attributed to the neurotoxicity of ethanol on the brain and to vitamin B complex deficiency [6] or the indirect effect of electrolytic and osmotic changes, as in central pontine myelinolysis [7].
In our case, the patient presented with extrapyramidal tract symptoms and difficulty walking and had only partial callosal lesions on MRI, which are compatible with the B type of MBD and usually associated with a favorable prognosis [7]. Type A MBD is often fatal and presents with coma, seizures, and T2-hyperintense swelling of the entire corpus callosum on MRI [8].
Three clinicoradiologic forms are distinguished: Acute (2 weeks); subacute (>2 weeks); and chronic (>3 months). MRI plays a pivotal role in supporting the diagnosis of MBD in non-alcoholic patients. In Acute MBD, the corpus callosum appears hyperintense in T2 and hypointense in T1. In subacute MBD, the patient may develop cystic lesions and small foci in T2, commonly due to hemosiderin deposits. In chronic MBD, residual atrophy is seen [9-12].
Treatment with corticosteroids and stabilization of plasma glucose have been described in several patients with favorable outcomes [11].
The severity of disease is variable and may produce a fatal outcome or partial clinical recovery [7].
Conclusion
We conclude that, in addition to Alcoholism and malnutrition, osmotic changes associated with glycaemic fluctuations, can cause this disease. MRI offers many advantages as pathophysiological mechanism of MBD at an early stage, diagnostic and prognostic.
References
- Perea, Jhon, Luis, María Belén, Luciana Grimanesa, et al. Marchiafava-Bignami Disease Associated with Spinal Involvement. Case reports in neurological medicine. 2020; 202.
- Celik, Yahya, Temizoz, Osman, Hakan, et al. A non-alcoholic patient with acute Marchiafava-Bignami disease associated with gynecologic malignancy: paraneoplastic Marchiafava-Bignami disease?. Clinical neurology and neurosurgery. 2007; 109: 505-508.
- Dong, Xiaoyu, Bai, Chaobo, Nao, et al. Clinical and radiological features of Marchiafava-Bignami disease. Medicine. 2018; 97: 5.
- Khan, Ateeque Ahmed, Sasui, Shaikh, Rehana, et al. Marchiafava-Bignami Disease: A Rare Disease with MRI Findings and Literature Review. Journal of Islamabad Medical & Dental College. 2017; 6: 275-277.
- Yadala, Sisira, Luo, Jin Jun. Marchiafava-bignami disease in a nonalcoholic diabetic patient. Case reports in neurological medicine. 2013; 2013.
- Tian, Terrence Y, Ruschel, Pescador, Park, et al. Marchiafava Bignami Disease. 2018.
- Álvarez, AI Pérez, Carbajo, C Ramón, De La Tassa, et al. Marchiafava-Bignami disease triggered by poorly controlled diabetes mellitus. Neurologia (Barcelona, Spain). 2016; 31; 498-500.
- Pinheiro BG, Melo AS, Fernandes LMP, et al. Alcoholic Neurological Syndromes. In: Addictive Substances and Neurological Disease. Academic Press, 2017. p. 127-137
- Miranda-Nava, Gabriel, García-Toribio, Martha Guadalupe. Marchiafava-Bignami: case report. Revista Mexicana de Neurociencia. 2017; 18: 98-103.
- Namekawa, Michito, Nakamura, Yuko, Nakano, Imaharu. Cortical involvement in Marchiafava-Bignami disease can be a predictor of a poor prognosis: A case report and review of the literature. Internal medicine. 2013; 52: 811-813.
- Suzuki Y, Oishi M, Ogawa K, Kamei S. A patient with Marchiafava-Bignami disease as a complication of diabetes mellitus treated effectively with corticosteroid. J Clin Neurosci. 2012; 19: 761-2.
- Sisira Yadala, Jin Jun Luo. Marchiafava-Bignami Disease in a Nonalcoholic Diabetic Patient. Case Reports in Neurological Medicine. 2013; 2013: 4.