
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A very rare case of light chain negative (non-producer) IgA plasma cell myeloma
Aliaa Mohamed Amer1*; Dina Sameh Abdelrahman Soliman1,2,3; Feryal Abbas Ibrahim Hilmi1; Samah Ahmed Samy Aly Kohla1,2,4; Ibrahim Almahdi A Ganwo1; Hesham Mahmoud A Elsabah5; Mouhammad Zuhair Sharaf Eldean1
1Department of Laboratory Medicine & Pathology, Hamad Medical Corporation, Hamad General Hospital, Doha 00974, Qatar.
2Weill Cornell Medicine, Doha, Qatar.
3National Cancer Center, Cairo University, Cairo, Egypt.
4Faculty of Medicine, Al-Azhar University, Cairo, Egypt.
*Corresponding Author : Aliaa Mohamed Amer
Department of Laboratory Medicine & Pathology, Hamad Medical Corporation, Hamad General Hospital, Doha 00974, Qatar.
Email: aamer1@hamad.qa
Received : Jul 05, 2023
Accepted : Jul 24, 2023
Published : Jul 31, 2023
Archived : www.jcimcr.org
Copyright : © Mohamed Amer A (2023).
Abstract
Multiple Myeloma (MM) is the 2nd most frequently diagnosed hematologic malignancy and accounts for 10-15% of all blood cancers and 1–1.8% of all cancers. Approximately 1% plasma cell myelomas are non-secretory (NSMM) and 15% of latter are non-producers (NSNPMM) where no cytoplasmic immunoglobulin (lg) synthesis is detected. We present a rare case presenting with multiple bone fractures and hypercalcemia and no monoclonal (M) protein in serum or urine. The diagnosis was challenging because the bone marrow (BM) sample provided was limited to a suboptimal core biopsy and touch imprint with no aspirate, therefore, flow cytometry and cytogenetics testing were not performed. We relied on immunohistochemistry and FISH analysis on paraffin embedded tissue to conclude a final diagnosis of NSNPMM. The challenge still exists in disease monitoring and a customized protocol is suggested. Non-Producing Multiple Myeloma (NPMM) though recognized three decades ago has only been described in a small number of case reports and further extensive research is still needed.
Keywords: Non-secretory; Non-producer; Myeloma.
Citation: Mohamed Amer A, Abdelrahman Soliman DS, Ibrahim Hilmi FA, Samy Aly Kohla SA, A Ganwo IA, et al. A very rare case of light chain negative (non-producer) IgA plasma cell myeloma. J Clin Images Med Case Rep. 2023; 4(7): 2522.
Introduction
Plasma Cell Myeloma (PCM) is a bone marrow-based multifocal neoplastic proliferation of plasma cells and accounting for 10-15% of hemopoietic neoplasms. It is usually associated with an M protein in serum and/or urine with evidence of organ damage related to plasma cell neoplasm [1]. Approximately 1% of plasma cell myelomas are NSMM, where there is absence of an M protein by serum and urine immunofixation electrophoresis. In about 15% of these NSMM cases, no cytoplasmic Ig synthesis is detected, fitting a term of Non-Secretory Non-Producer Myeloma (NSNPMM) [2] and although this rare entity was recognized three decades ago [3], it has only been described in a small number of case reports.
We present a challenging case, which to the best of our knowledge is the first described in the literature, where the myeloma is partly non secretory and partly non-producer where cytoplasmic immunoglobulin IgA could only be demonstrated by Immunohistochemistry (IHC) on Bone Marrow Biopsy (BMB), whereas light chains were not expressed, with absent M spike in serum and urine and negative Kappa (K) and Lambda (L) light chains both by IHC and In Situ Hybridization (ISH) for light chains mRNA.
Case presentation
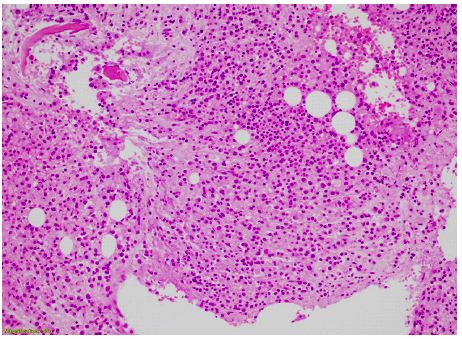
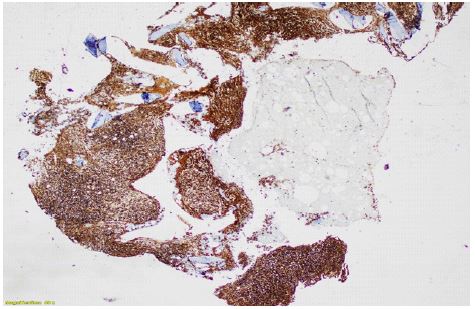
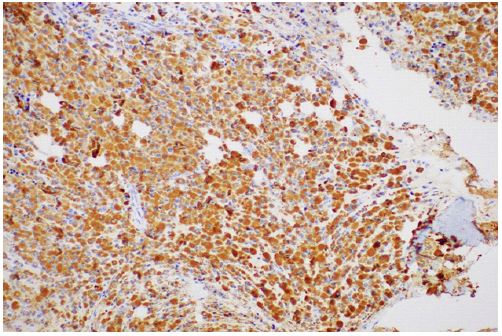
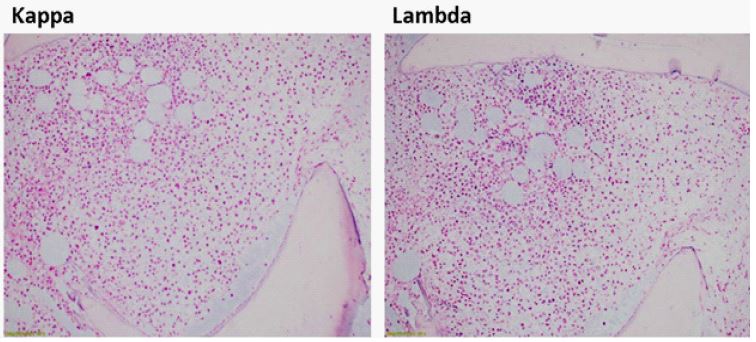
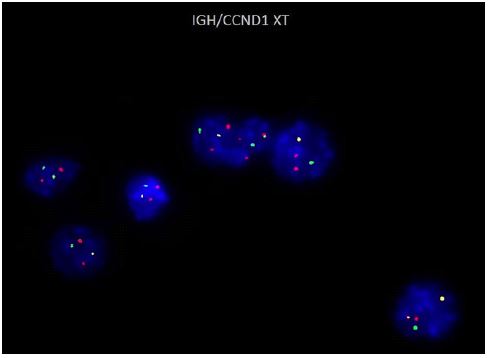
The patient is a 47-year-old female who presented with pathological fractures. PET CT demonstrated multiple destructive lytic lesions in both scapulae, sternum, right clavicle, multiple ribs, multiple vertebrae (most severe at T6), bilateral pelvic bones, and bilateral proximal femurs. The majority of these lytic lesions showed no significant FDG uptake; however, the left femoral neck destructive lesion showed surrounding soft tissue edema and increased FDG uptake due to recent fracture. Biochemical analysis revealed hypercalcemia (3.0 mg/dl), low serum Igs (hypogammaglobulinemia) and absence of an M protein by serum and urine protein electrophoresis and immunofixation using anti sera specific for IgG, IgM, IgD, IgA and IgE. Bence Jones protein was negative. Serum free light chains (FLC) were at their low levels (1.1 and 4.0 mg/dl for K and L FLC respectively) with a K/L ratio of 0.28. Peripheral blood showed moderate anemia with a Hb of 8.0 g/dl with no significant rouleaux in peripheral smear (a finding commonly seen in cases of myeloma). Bone curettage from the site of fracture (left femur head) demonstrated extensive infiltration by many plasma cells which by IHC were found positive for CD138, MUM1 and cyclin D1 but negative for both kappa and lambda light chains. BMB touch imprints showed sheets of plasma cells, majority large in size with distended pinkish cytoplasm with many flaming and some multinucleated forms (Figure 1). A small BM core biopsy was provided, showing few hypercellular intertrabecular spaces extensively infiltrated by plasma cells with streaming and increased fibrosis (MF 1-2). IHC showed the plasmacytic infiltrate positive for CD138, MUM-1, Cyclin D1 and cytoplasmic IgA (Figure 2) while negative for both K and L light chains, the latter finding was further confirmed by K and L mRNA by In Situ Hybridization (ISH). Fluorescence In Situ Hybridization (FISH) done on BMB revealed IGH/CCND1 rearrangement in 186/200 nuclei (Figure 3).
Based on the clinical presentation, hypercalcemia, the extensive plasmacytic infiltrate in the BMB with the single expression of one Ig isotype (IgA heavy chain) in the cytoplasm of the plasma cells and absence of K and L light chains both in serum and urine as well as in the plasma cells, in addition to Cyclin-D1 expression, the diagnosis of a non-secretory IgA multiple myeloma was made. Unfortunately, BM aspiration failed and hence no flow cytometry or cytogenetics (karyotype) testing was performed. According to multidisciplinary team (MDT) decision, the patient was started on Zoledronic and D-VTD (daratumumab in combination with bortezomib, thalidomide and dexamethasone), to be later scheduled for Autologous Stem Cell Transplantation (ASCT).



Discussion
The diagnosis of plasma cell neoplasms including myeloma is based on the detection of clonal plasma cells and M protein. Generally, when 10% of the BM volume is composed of plasma cells, a diagnosis of myeloma is likely, although rare cases of reactive plasmacytosis can reach that level or even higher [4]. However, in the case presented here, reactive plasmacytosis was excluded based on the presence of lytic bone lesions, hypercalcemia, the extent of bone/BM infiltration with abnormal looking plasma cells and most importantly, neither kappa nor lambda light chains expression could be demonstrated by IHC, ISH or immunofixation techniques while all the plasma cells were exclusively expressing IgA heavy chain by IHC.
Our case does not actually fit into any of the myeloma variants defined either by WHO or IMWG; as NSMM is defined by absence of an M protein in serum and urine by immunofixation electrophoresis. however, with the presence of cytoplasmic M protein in the neoplastic plasma cells in about 85% of cases when evaluated by IHC, consistent with production but impaired secretion of lg [5]. This contrasts with non-producer myeloma (which constitutes about 15% of NSMM, where no cytoplasmic lg synthesis is detected.
Our case seems to have an unusual defect in immunoglobulin production/secretion, where the plasma cells expressed the heavy chain (IgA) but failed to express/secrete any light chain.
Possible mechanisms of this rare finding may include an acquired mutation of the Ig light chain variable genes and/or alteration in the light chain constant region which have led to failure of production of light chain thus interfered with immunoglobulin molecule assembly and secretion. Similar mechanisms have also been proposed in the pathogenesis of NSMM [6] However, this is a proposed possible mechanism as we could not find similar cases reported with discrepancy between light and heavy chain expression within PCM. Also, the increased expression of cyclin D1 in this very rare non producer MM entity suggests that the t(11;14) plays a role in its pathophysiology [7].
Heavy Chain Diseases (HCDs) on the other hand are rare B-cell neoplasms characterized by the production of monoclonal immunoglobulin heavy chains (lgG, lgA HCD, or lgM) and typically no light chains [8,9]. The heavy chain is usually truncated, preventing normal assembly with light chains. However, this diagnosis was excluded in our case as there was no B-cell differentiation noted and the whole neoplastic cells were plasma cells.
Currently, treatments for NSMM are the same as those for secretory MM however the current data on overall survival are yet inconclusive. Given the higher incidence of t(11,14), customized treatment protocols may probably erupt. The prognostic significance of t(11;14) MM remains debatable, as studies continue to show varying outcomes for patients harboring t(11;14) and may further evolve into changing treatment landscape [10-12].
Monitoring efficacy of treatment in true cases of NSMM typically lack easy parameters for evaluating response to treatment and monitoring and evaluation of treatment efficacy will probably be a real challenge to both oncologist and hematopathologist. Simultaneous BM examination with multiparametric flow cytometry and sensitive imaging (e.g., magnetic resonance imaging (MRI) or PET/CT) are currently the best way to assess the effectiveness of treatment in patients with NSMM [13]. Non-producer MM however, still constitutes a further dilemma due to inability to use serum and urine Ig studies as reliable surrogates for tumor burden and in our case, PET CT was only useful in detecting the multiple lytic bone lesions at diagnosis but no significant FDG avidity was demonstrated and thus questioning its value in disease monitoring. It looks like IHC staining for IgA heavy chain and Cyclin D1 positivity in addition to FISH analysis for t(11;14) will represent the only tools available for follow up and disease monitoring in our case.
Conclusion
Non-Producing Multiple Myeloma (NPMM) though recognized three decades ago has only been described in a small number of case reports. Herein, we report an exceptional case of IgA PCM, where only heavy chain could be detected in the cytoplasm of the myeloma cells by IHC with no evidence of production or secretion of light chains in serum or tissue. No myeloma cases with similar biology could be found in the literature. Monitoring and evaluation of treatment efficacy in our patient will probably be a real challenge to both oncologist and hematopathologist. Currently, treatments for NSMM are the same as those for secretory MM however the current data on overall survival are yet inconclusive. Given the higher incidence of t(11,14) customized treatment protocols may probably erupt. More research on this unique entity still needs to be made. Multicenter based studies for myeloma cases with similar biology, is probably needed to study the actual incidence of such cases and explore more regarding the precise disease pathogenesis and its effect on myeloma course, outcome and overall survival.
Acknowledgement: The authors would to acknowledge the role of Dr Francis Lam for pursuing extensive multistep protein electrophoresis and immunofixation and Dr Zafar Nawaz and Ms Farzana Murad for performing and interpreting the FISH analysis.
References
- Palumbo A, Bringhen S, Ludwig H, Dimopoulos MA, Bladé J, et al, Personalized therapy in multiple myeloma according to patient age and vulnerability: A report of the European Myeloma Network (EMN). Blood. 2011; 118: 4519-4529.
- Coriu D, Weaver K, Schell M, Eulitz M, Murphy CL, et al. A molecular basis for non-secretory myeloma. Blood 2004; 104: 829-31.
- Barlogie B, Alexanian R, Pershouse M, Smallwood L, Smith L. Cytoplasmic immunoglobulin content in multiple myeloma. J Clin Invest. 1985; 76: 765-769.
- Jego G, Avet-Loiseau H, Robillard N, Moreau P, Amiot M, et al. Reactive plasmacytoses in multiple myeloma during hematopoietic recovery with G- or GM- CSF. Leuk Res, 2000; 24: 627-630.
- International Myeloma Working Group. Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: a report of the International Myeloma Working Group. Br J Haematol. 2003; 121: 749-57.
- Dul JL, Argon Y. A single amino acid substitution in the variable region of the light chain specifically blocks immunoglobulin secretion. Proc Natl Acad Sci USA. 1990; 87: 8135-9.
- Papanikolaou X, Zhang Q, Heuck C, Waheed S, Atrash S, et al. Non-Producing Multiple Myeloma (MM) Is a Distinct Subset Of Non-Secretory MM Characterized By High Cyclin D1 Expression and Decreased Progression Free Survival. Blood 2013; 122: 1911.
- Bianchi G, Anderson KC, Harris NL, Sohani AR. The heavy chain diseases: Clinical and pathologic features. Oncology (Williston Park). 2014; 28: 45-53.
- Wahner-Roedler DL, Kyle RA. Heavy chain diseases. Best Pract Res Clin Haematol. 2005; 18: 729-46.
- Bal S, Giri S, Godby KN, Costa LJ. Impact of t(11;14) as a sole and concomitant abnormality on outcomes in multiple myeloma. Br J Haematol. 2021; 195: e113-e116.
- Grzegorz Charliński, Artur Jurczyszyn. Non-secretory multiple myeloma: Diagnosis and management. Adv Clin Exp Med. 2022; 31: 95-100
- Bal S, Kumar S, Fonseca R, Gay F, Hungria V, et al. Multiple myeloma with t(11; 14): Unique biology and evolving landscape. Am J Cancer Res. 2022; 12: 2950- 2965.
- Durie BG, Harousseau JL, Miguel JS, Bladé J, Barlogie B, et al. International uniform response criteria for multiple myeloma. Leukemia. 2006; 20: 1467-1473.