Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Stretching the potential of the lumbar ESP block: Case report of an effective perioperative analgesia for a major tibia endoprosthetic surgery
Jonathan ZM Lim*; Irene AL Lim
Department of Anaesthesia, National University Hospital, Singapore.
*Corresponding Author : Jonathan Lim
Department of Anaesthesia, National University Hospital, Singapore.
Email: [email protected]
Received : Jul 06, 2023
Accepted : Jul 25, 2023
Published : Aug 01, 2023
Archived : www.jcimcr.org
Copyright : © Jonathan ZML (2023).
Abstract
Background: The Erector Spinae Plane (ESP) block has been shown to provide good perioperative analgesia for thoracic, chest wall, abdominal, spinal and hip surgeries. A recent case report had demonstrated its efficacy in post-operative analgesia for an above-knee amputation surgery, but no reports have been published on ESP for surgeries below the level of the knee despite the theoretical possibility based on anatomical knowledge of the dermatomes and myotomes of the lumbar region. The authors would like to publish the first case report of effective use of lumbar ESP block with catheter for intra and post-operative analgesia for an extensive tibia endoprosthesis surgery.
Case presentation: Our patient, ESV is a 12-year-old male with non-metastatic osteosarcoma of the right proximal tibia. ESV and his mother were keen for a block for supplemental analgesia but not involving the central neuraxial axis, so a lumbar ESP block at L3 level was proposed. ESV was given a general anaesthetic and an ESP block with catheter was sited at the level of the right L3 transverse process. He underwent a 7-hour long resection of tumour and insertion of tibia endoprosthesis for which the ESP block initial bolus was effective in achieving good intraoperative analgesia. Post-operatively, the ESP block catheter was used to deliver Programmed Intermittent Boluses (PIB) of Local Anaesthetic (LA) for analgesia in the first 3 post-operative days, while facilitating ambulatory physiotherapy.
Conclusions: This case report demonstrates the efficacy of a lumbar ESP block in delivering good intraoperative analgesia for lower limb surgery. It also demonstrates that the continued use of a lumbar ESP catheter for PIB local anaesthetic boluses affords adequate analgesia without significant motor block and impediment to physiotherapy.
Keywords: Tibia; Knee; Lumbar Erector Spinae Plane (ESP) block; Catheter infusion; Programmed intermittent bolus; Perioperative analgesia.
Abbreviations: ESP: Erector Spinae Plane; CNB: Central Neuraxial Block; PACU: Post-Anaesthetic Care Unit; PIB: Program Intermittent Bolus; LA: Local Anaesthetic; POD: Post-Operative Day.
Citation: Jonathan ZML, Irene ALL. Stretching the potential of the lumbar ESP block: Case report of an effective perioperative analgesia for a major tibia endoprosthetic surgery. J Clin Images Med Case Rep. 2023; 4(8): 2523.
Introduction
Erector Spinae Plane (ESP) blocks are effective alternatives to Central Neuraxial Blocks (CNBs) for peri-operative analgesia for thoracic [1], abdominal [2], spine [3] and hip surgeries [4]. The use of ESP blocks for surgeries below the knee has not been reported.
ESP blocks were found to be equally efficacious to thoracic epidural analgesia for esophageal surgeries [5] and paravertebral blocks for thoracoscopic surgeries [6]. The lumbar ESP block has also been compared against the Fascia Iliaca Block (FIB) for total hip arthroplasty and shown to have better preservation of quadriceps strength [7].
Case presentation
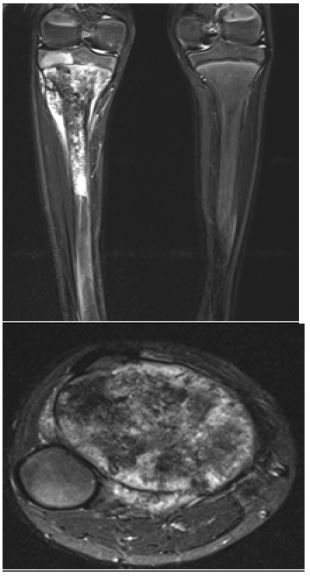
Our patient, ESV was a 12-year-old, 33 kg male with non-metastatic osteosarcoma of the right proximal tibia. ESV had chemotherapy prior to surgery and had no other significant medical history.
ESV was intubated under general anaesthesia and was turned left lateral for the lumbar ESP block. The ESP needle was sited with an in-plane technique under ultrasound guidance at the right L3 transverse process using a 100 mm echogenic needle. An initial bolus of 25 ml of 0.28% ropivacaine was administered with good Local Anaesthetic (LA) spread observed on ultrasound. The catheter was secured 2.5 cm in the myofascial plane.
A Target-Controlled Infusion (TCI) of remifentanil was used and ESV only needed an effect site concentration of 0.2-0.4 ng/ml for the 1st 4.5 hours of surgery. After the block wore off, he was administered 7 ml of 0.2% ropivacaine hourly through the catheter. Prior to extubation, ESV was also given 500 mg of intravenous paracetamol, 3mg of oxycodone and 20mg of ketamine. He required 2 mg of oxycodone and 10 mg of ketamine in the Post-Anaesthetic Care Unit (PACU) due to mild knee discomfort. A Program Intermittent Bolus (PIB) pump initiated to administer 7 ml of 0.2% ropivacaine every hour for the patient through the ESP catheter.
When the Acute Pain Service (APS) team reviewed ESV on Post-Operative Day (POD) 1, he reported numbness at the L2 dermatome but no weakness. He had moderate pain at rest and on movement, so he started on mist morphine 5mg every 4 hours, paracetamol 500 mg every 6 hours and ibuprofen 300mg every 8 hours.
On POD 2, his PIB settings was changed to 15 ml of 0.2% ropivacaine every 4 hours, which resulted in mild pain at rest and tolerable pain when ambulating with crutches.
On POD 3, the ESP catheter was removed and ESV had severe pain over the right tibia 6 hours later. He was given 10 mg of mist morphine rescue with his mist morphine dosing increased to 7.5 mg every 4 hours, and started on 70 mg of gabapentin every 8 hours. Wound inspection on POD 4 revealed healthy healing of tissues and he was continued on ambulatory physiotherapy before he was discharged well on POD 9.
Discussion
ESP blocks have several advantages against their CNB counterparts by avoiding the subarachnoid and epidural space. Patients who are on anti-platelets or anticoagulants are contraindicated for CNBs [8] but may get ESPs without the risk of spinal or epidural hematomas. Patients who are septic risk seeding bacteria into the CNS with CNBs, with an incidence of 0.007% to 0.6% [9] but this is negligible for ESP blocks. Post-Dural Puncture Headaches (PDPH) from breaching the subarachnoid space with CNBs are also avoided with ESP blocks.
ESPs also offer unilateral blockade for one-sided surgeries. Although the ESP has been reported to block sympathetic nerve fibres to generate visceral abdominal analgesia in bariatric surgeries [10-12], incidences of severe hypotension from blocking the thoracolumbar sympathetic chain are rare compared to CNBs.
Furthermore, lumbar ESPs are associated with a low incidence of motor block and often imperceptible sensory block despite provision of analgesia [13]. Though there are reports of ESP blocks causing motor deficits [11] and hypotension [12] postulated from epidural spread through the costotransverse foramen, incidences are estimated to be 0.2% [13]. CNBs, femoral or sciatic nerve blocks for lower limb surgeries may result in significant motor and possibly prolonged sensory block, which would be counterproductive for early rehabilitation after surgery. In ESV’s case, the ESP block and catheter infusion did not result in motor or sensory blockade so he was cooperative with physiotherapy, yet with adequate pain control for mobilisation.
The authors would like to recommend the use of PIB administration of LA as opposed to a continuous infusion for the lumbar ESP block. Epidural studies have demonstrated the superiority of PIB to continuous infusion of LA for labour analgesia [14] and the authors postulate that PIBs would afford better cephalo-caudal spread of the ESP block in the same fashion. Patient ESV was initially started on a PIB of 7ml of 0.2% ropivacaine every hour. Since the paravertebral spread of ESP blocks are known to be volume-dependent [15], a larger PIB bolus with a lower frequency was proven superior to a lower PIB bolus at a higher frequency in our patient.
Conclusion
The ESP block is a reliable regional anaesthetic technique for truncal, hip and proximal femur surgeries. Our patient has demonstrated the successful use of a lumbar ESP block for proximal tibia surgery both in terms of perioperative analgesia and facilitation of early rehabilitation. With increasing familiarity of the lumbar ESP block, it can potentially replace many CNBs for unilateral limb surgeries below the knee, as it comes without the risks of CNBs, but with the added benefit of lateralisation of block side, decreased hemodynamic instability and reduced motor block which would allow for early rehabilitation.
Declarations
Ethics approval and consent to participate: Ethics approval was not required for the case report. Our patient and his mum were agreeable for the authors to write up on his case to apprise the medical community, and the patient’s mum signed our institutional consent form for the use of his medical records including photographs and images for the publication.
Consent for publication: As the patient is a minor, the consent for publication including the use of photographs and images was given by his mother using our institutional consent form.
Availability of data and materials: Our patient’s medical records are available upon request to the authors.
Competing interests: The authors have no financial or non-financial competing interests to declare.
Funding: No funding was required nor solicited for the case report.
Acknowledgements: We are grateful to our patient, his family as well as all the physicians and allied health members involved in the care of this patient.
Supplementary file (Photographs): Preoperative and intraoperative images of right proximal tibia osteosarcoma; Postoperative images of patient’s wound and lumbar ESP catheter.
References
- Naghmeh Pirsaharkhiz, Kelly Comolli, Wakana Fujiwara, Susan Stasiewicz, Jeanne M Boyer, et al. Utility of erector spinae plane block in thoracic surgery. J Cardiothorac Surg. 2020; 15: 91.
- Serkan Tulgar, Onur Selvi, Mahmut Sertan Kapakli. Erector Spinae Plane Block for Different Laparoscopic Abdominal Surgeries: Case Series, Case Rep Anesthesiol. 2018; 2018: 3947281.
- Hironobu Ueshima, Mayumi Inagaki, Tomoaki Toyone, Hiroshi Otake. Efficacy of the Erector Spinae Plane Block for Lumbar Spinal Surgery: A Retrospective Study. Asian Spine J. 2019; 13: 254-257.
- Ali Ahiskalioglu, Serkan Tulgar, Mine Celik, Zeliha Ozer, Haci Ahmet Alici, et al. Lumbar Erector Spinae Plane Block as a Main Anesthetic Method for Hip Surgery in High Risk Elderly Patients: Initial Experience with a Magnetic Resonance Imaging, Eurasian J Med. 2020; 52: 16-20.
- Hoda Shokri, Amr A Kasem. Analgesic efficacy of erector spinae block in comparison to thoracic epidural anesthesia in patients undergoing transthoracic esophageal surgical procedure. Research and Opinion in Anesthesia and Intensive Care. 2020; 7: 124-130.
- Y Taketa, Y Irisawa, T Fujitani. Comparison of ultrasound-guided erector spinae plane block and thoracic paravertebral block for postoperative analgesia after video-assisted thoracic surgery: A randomized controlled non-inferiority clinical trial Regional Anesthesia & Pain Medicine.
- E Flaviano, S Bettinelli, M Assandri, H Muhammad, A Benigni, et al. Erector spinae plane block versus fascia iliaca block after total hip arthroplasty: a randomized clinical trial comparing analgesic effectiveness and motor block. Korean J Anesthesiol. 2023.
- Samer Narouze, Honorio T Benzon, David Provenzano, Asokumar Buvanendran, José De Andres, et al. Huntoon, Interventional Spine and Pain Procedures in Patients on Antiplatelet and Anticoagulant Medications (Second Edition) Guidelines From the American Society of Regional Anesthesia and Pain Medicine, the European Society of Regional Anaesthesia and Pain Therapy, the American Academy of Pain Medicine, the International Neuromodulation Society, the North American Neuromodulation Society, and the World Institute of Pain, Chronic And Interventional Pain (Special Article).
- Ana María Gimeno, Carlos Luis Errando. Neuraxial Regional Anaesthesia in Patients with Active Infection and Sepsis: A Clinical Narrative Review. Turk J Anaesthesiol Reanim. 2018; 46: 8-14.
- Ki Jinn Chin, Laith Malhas, Anahi Perlas. The Erector Spinae Plane Block Provides Visceral Abdominal Analgesia in Bariatric Surgery: A Report of 3 Cases, Reg Anesth Pain Med. 2017; 42: 372-376.
- O Selvi, S Tulgar. Ultrasound guided erector spinae plane block as a cause of unintended motor block. Rev Esp Anestesiol Reanim. 2018; 65: 589-92.
- Kumar, Kamal, Woods, Megan, Ludwig, et al. Motor block and hypotension following a high thoracic erector spinae plane block. Journal of Anaesthesiology Clinical Pharmacology. 2022; 38: 678-679.
- Tulgar S, Senturk O, Serifsoy TE, Thomas DT. Ultrasound-guided erector spinae plane block: Indications, complications, and effects on acute and chronic pain based on a single-center experience. Cureus. 2019; 11: e3815.
- Cynthia A Wong, John T Ratliff, John T Sullivan, Barbara M Scavone, Paloma Toledo, et al. A randomized comparison of programmed intermittent epidural bolus with continuous epidural infusion for labor analgesia. Anesth Analg. 2006; 102: 904-9.
- You-Jin Choi, Hyun-Jin Kwon, Jehoon O, Tae-Hyeon Cho, Ji Yeon Won, et al. Influence of injectate volume on paravertebral spread in erector spinae plane block: An endoscopic and anatomical evaluation. PLoS One. 2019; 14: e0224487.