
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
The role of ablation therapy and brachytherapy in the management of metastatic leiomyosarcoma: A case report
Daniel Gallie1; Hannah Riskin-Jones2; Daniel H Kim2*; Albert Chang3; Steven Raman2; Bartosz Chmielowski4; Robert Suh2
1Department of Biochemistry, University of California Riverside, Riverside, CA, USA.
2Department of Radiology, David Geffen School of Medicine at UCLA, Los Angeles, CA, USA.
3Department of Radiation Oncology, David Geffen School of Medicine at UCLA, Los Angeles, CA, USA.
4Division of Hematology-Oncology, Jonsson Comprehensive Cancer Center, Department of Medicine, David Geffen School of Medicine at UCLA, Los Angeles, CA, USA.
*Corresponding Author : Daniel HS Kim
Department of Radiology, David Geffen School of Medicine at UCLA, Los Angeles, CA, USA.
Email: DHKim@mednet.ucla.edu
Received : Jul 07, 2023
Accepted : Jul 27, 2023
Published : Aug 03, 2023
Archived : www.jcimcr.org
Copyright : © Kim DH (2023).
Abstract
Local therapies such as ablation therapy and brachytherapy may play a role in the management of patients with metastatic sarcomas. Here, we report a case of retroperitoneal leiomyosarcoma in a 62-year-old male, who developed local recurrence and pulmonary, hepatic, renal, peritoneal, intramuscular, and subcutaneous metastases over the course of four years following surgical resection of the primary tumor. In addition to first-line chemotherapy, disease progression is managed with microwave ablation, cryoablation, and brachytherapy of metastatic nodules. The use of ablation therapy and brachytherapy served to manage the spread of the disease by managing multiple lung metastases, thus contributing to the maintenance of the quality of life. Ablation therapy and brachytherapy can be important complements to traditional treatment modalities and may prove useful in managing a wide range of solid tumor cancers.
Keywords: Leiomyosarcoma; Microwave ablation; Cryoablation; Brachytherapy; Metastatic lung nodules.
Abbreviations: RFA: Radiofrequency Ablation; MWA: Microwave Ablation; CT: Computed Tomography; MRI; Magnetic Resonance Imaging; PET: Positron Emission Tomography; SUV: Standardized Uptake Values; FDA; Food And Drug Administration; STS: Soft Tissue Sarcoma; NCCN: National Comprehensive Cancer Network; SBRT: Stereotactic Body Radiation Therapy.
Citation: Gallie D, Riskin-Jones H, Kim DH, Chang A, Raman S, et al. The role of ablation therapy and brachytherapy in the management of metastatic leiomyosarcoma: A case report. J Clin Images Med Case Rep. 2023; 4(8): 2528.
Introduction
Leiomyosarcoma is an uncommon malignant neoplasm that occurs in less than two per million people annually [1]. It is of smooth muscle origin that typically arises in somatic soft tissues, the retroperitoneum, genitourinary tract, gastrointestinal tract, and large vessels, with some occurrence in bones, skin, and subcutis [2]. 20-67% of primary leiomyosarcomas occur in the retroperitoneum [3] with only liposarcomas being more common in this location [4]. Leiomyosarcoma usually metastasizes via hematogenous spread most often to the lung, liver, and kidney [1,2,5] but rare metastasis to other sites including skin, scalp, subcutis, skeletal muscles, pancreas, stomach, small bowel, cardiac chambers, and submandibular salivary gland have been reported [2,6,15-17,7-14]. These typically occur late in the course of the disease, indicating a poor prognosis [1,2]. In addition to metastasis, local recurrence occurs as frequently as 40-77% [4]. Compared to leiomyosarcomas at all sites, retroperitoneal leiomyosarcomas have the worst prognosis, and approximately 80-87% of these patients die within 5 years [4]. Because of its typically late presentation, location deep within tissue, and characteristic insensitivity to chemotherapy or radiotherapy, a complete cure following resection of the primary retroperitoneal leiomyosarcoma has been challenging [3,4]. Surgery and equivalent therapies remain the best means to control the disease. Ablation of primary or metastatic tumors offers a less invasive approach for resection. Various ablation modalities such as Radiofrequency Ablation (RFA), Microwave Ablation (MWA), and cryoablation have proven effective in providing local control in multiple cancer types [18-25] as brachytherapy [26,27]. Recent studies have supported the use of ablation therapy as a means of extending overall survival [21,28-31].
In this case report, we describe the case of a patient who underwent neoadjuvant chemotherapy/radiation, resection of the primary tumor, subsequent metastasis, and first-line chemotherapy. This standard of care was complemented by MWA, cryoablation, and brachytherapy for metastatic nodules. We report this case to highlight the use of these therapies to manage metastatic cancer, inform oncologists of these therapies as a complement to traditional treatment modalities, and increase the interest in these therapies to promote their consideration as an available management option for many types of cancer.
Case presentation
A 58-year-old male, who underwent orchiectomy for a 2 cm × 2 cm pure seminoma of the right testis and prophylactic para-aortic and right iliac radiation (25 Gy administered over 14 days) 25 years previously, presented with abdominal pain. Computed Tomography (CT), Magnetic Resonance Imaging (MRI), and Positron Emission Tomography (PET) (maximum SUV of 5.42) examinations revealed a 6.0 cm × 6.0 cm × 4.0 cm lobulated heterogeneous right pelvic retroperitoneal mass encasing the right external iliac artery and vein. Biopsy of the mass revealed histological features of a typical leiomyosarcoma with numerous mitoses (greater than 20/10 HPFs) and foci of necrosis, indicating a grade 3 (high-grade) tumor by the French grading system. The location of the tumor corresponded to the prior right iliac radiation area, suggesting a radiation-associated origin, although it did not appear as an undifferentiated radiation-associated sarcoma. The tumor appeared to arise from the vasculature, as it encased the right external iliac artery and vein. The patient underwent neoadjuvant chemotherapy (ifosfamide) and radiation prior to radical resection of the tumor, with en bloc resection of the right external iliac artery and vein. Reconstruction of the right external iliac artery with a 6 mm Dacron graft and the vein with a cryopreserved arterial homograft was performed. Moderate right renal hydroureteronephrosis with a dilated ureter extending down to the level of the tumor was observed after resection, consistent with compression of the right ureter by the tumor that had been observed intraoperatively.
Although bilateral lung nodules were first observed by CT examination three months after resection, they remained stable in size until 12 months post-surgery at which point further growth was observed. Numerous small nodules (~20), confirmed by biopsy as metastatic leiomyosarcoma, were present in all lobes, but were confined to the lungs. Prior to systemic treatment, four of the largest lung metastases were ablated using CT-guided MWA (Table 1). Six cycles of doxorubicin and olaratumab were initiated 18 months after resection, and olaratumab administration was maintained following the doxorubicin treatment for an additional three months. Most of the lung nodules remained stable during the systemic treatment. During treatment with olaratumab, the patient continued to undergo MWA of additional lung nodules. The growth of the nodules resumed within four months of completing the treatment with doxorubicin. As their location precluded safe treatment through ablation, CT-guided brachytherapy was used to treat two lung nodules in the left lower lung lobe that appeared 18 months apart (Figure 1). The patient continued to receive CT-guided cryoablation (Figure 2) and MWA (Figure 3) of the lung nodules, with 74 lung nodules treated with ablation or brachytherapy over a 38-month period (Table 1). Simultaneously, the patient was on systemic therapy with pazopanib. However, the impact of pazopanib on the course of the disease is uncertain, as the therapy is frequently interrupted because of scheduled ablation procedures. After pazopanib was discontinued, the patient was offered alternative systemic therapy, but declined.
Three years after resection, multiple nodules appeared in other locations outside the lung, including two nodules in the retroperitoneum, one in the left buttock, two in the liver, three in the kidney, and four in the subcutaneous chest. Over the next several months, all nodules were treated using image-guided ablations (Table 1). An additional nodule in the right upper quadrant omentum adjacent to the antrum of the stomach and medial border of the gallbladder was treated using CT-guided brachytherapy to minimize damage to the surrounding organs. The patient reported little to no discomfort during these procedures or during recovery, typically returning to normal activity by the day after the procedure. Four and a half years after resection, there was widespread disease progression in the lung, liver, kidney, bone, and soft tissue. Systemic therapy with liposomal doxorubicin was initiated and additional metastases were treated with ablation and brachytherapy (Table 1). At this point, it was determined that the patient’s disease progressed too rapidly to continue metastasis-directed local therapy, and he was continued on systemic therapy only with a total of five cycles of liposomal doxorubicin followed by trabectedin. He died three months later having survived five and half years (67 months) from the time of his original diagnosis.
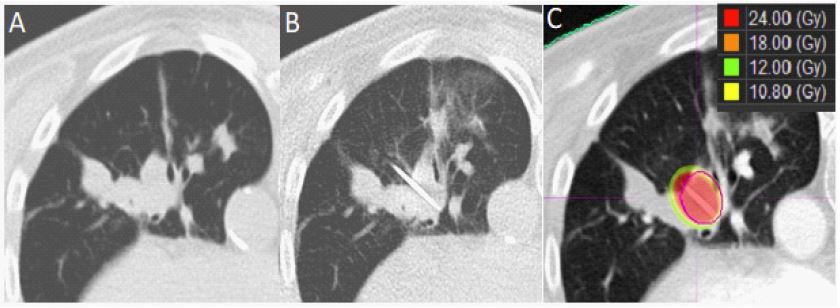
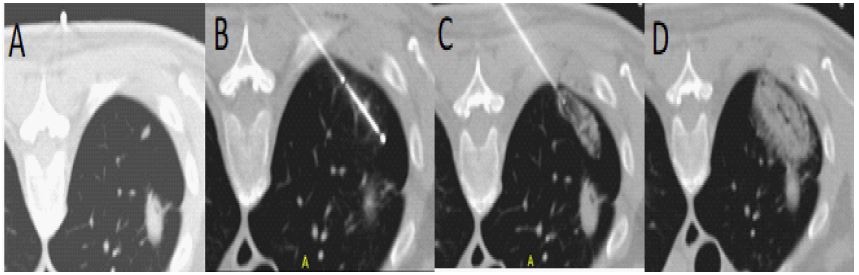
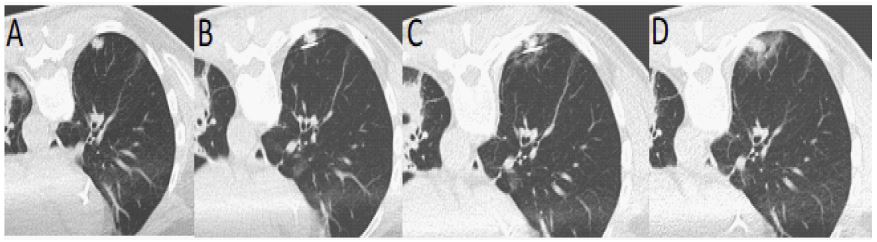
Table 1: Summary of treatment using ablation therapies and brachytherapy.
| Date | No. of ablations | Nodule size (cm) | Location | Treatment |
|---|---|---|---|---|
| 2-13-2017 | 1 | 1.2 x 1.6 | Lung- Left upper lobe | Microwave |
| 3-13-2017 | 1 | 1.1 x 0.8 | Lung- Right lower lobe | Microwave |
| 4-10-2017 | 2 | 1.5 x 0.7 0.5 x 0.6 |
Lung- Right upper lobe | Microwave |
| 8-28-2017 | 2 | 1.4 x 1.1 1.0 x 0.8 |
Lung- Right lower lobe | Microwave |
| 10-16-2017 | 2 | 1.1 x 0.9 0.7 x 0.7 |
Lung- Left lower lobe | Microwave |
| 10-23-2017 | 1 | 1.2 | Lung- Right lower lobe | Microwave |
| 12-11-2017 | 1 | 1.1 x 0.7 | Lung- Left lower lobe | Cryoablation |
| 1-8-2018 | 1 | 3.0 x 2.0 | Lung- Left lower lobe, Lingula lymph node | Brachytherapy |
| 1-16-2018 | 1 | 1.2 x 1.2 | Lung - Left lower, lingula | Cryoablation |
| 1-29-2018 | 1 | 0.8 x 0.6 | Lung- Right upper lobe | Cryoablation |
| 3-12-2018 | 3 | 1.4 x 0.8 1.3 x 1.0 1.3 x 0.5 |
Lung- Right lower lobe | Microwave |
| 3-26-2018 | 3 | 1.0 0.9 0.4 |
Lung- Right upper lobe | Microwave |
| 4-9-2018 | 1 | 0.8 | Lung- Right upper lobe | Microwave |
| 4-30-2018 | 2 | 0.7 x 0.6 0.5 x 0.3 |
Lung- Left upper lobe | Cryoablation |
| 5-14-2018 | 2 | 1.3 x 0.7 0.7 x 0.4 |
Lung- Right upper lobe | Cryoablation |
| 6-11-2018 | 3 | 2.0 x 1.0 0.5 x 0.4 0.5 x 0.4 |
Lung- Left upper lobe | Microwave |
| 7-2-2018 | 1 | 1.7 x 1.4 | Lung- Right lower lobe | Microwave |
| 7-23-2018 | 3 | 0.9 x 0.8 0.7 x 0.5 0.7 x 0.4 |
Lung- Left upper lobe | Microwave |
| 8-13-2018 | 1 | 0.9 x 0.9 | Lung- Left upper lobe | Microwave |
| 8-27-2018 | 5 | 1.0 x 0.5 0.7 x 0.4 0.8 x 0.2 0.3 x 0.3 0.2 x 0.2 |
Lung- Right middle lobe | Microwave |
| 9-24-2018 | 2 | 1.1 x 0.4 0.4 x 0.3 |
Lung- Left lower lobe | Microwave |
| 10-15-2018 | 3 | 0.4 x 0.4 0.3 x 0.3 0.3 x 0.3 |
Lung- Left upper lobe | Microwave |
| 11-5-2018 | 1 | 0.8 x 0.7 | Lung- Left upper lobe | Microwave |
| 11-26-2018 | 1 | 0.8 x 0.7 | Lung- Right upper lobe | Microwave |
| 12-10-2018 | 2 | 1.0 x 0.9 0.7 x 0.6 |
Lung- Left upper lobe | Microwave |
| 1-14-2019 | 1 | 0.9 x 0.7 | Lung- Right middle lobe | Microwave |
| 1-28-2019 | 1 | 0.8 x 0.7 | Lung- Left lower lobe | Microwave |
| 2-7-2019 | 2 | 1.1 x 0.9 0.9 x 0.8 |
Subcutaneous anterior abdominal wall right retroperitoneum | Cryoablation Cryoablation |
| 2-18-2019 | 1 | 2.2 x 1.4 | Lung- Left major fissural pleura | Microwave |
| 3-18-2019 | 1 | 0.8 x 0.7 | Lung- Right lower lobe | Microwave |
| 3-29-2019 | 2 | 1.6 0.7 |
Liver – Segment 3 Subcutaneous left chest wall |
Microwave Microwave |
| 4-29-2019 | 1 | 1.2 x 1.0 | Lung- Left upper lobe | Microwave |
| 5-22-2019 | 2 | 1.2 1.0 |
Liver – segment 6 Subcutaneous left anterior abdominal wall |
Microwave Cryoablation |
| 5-28-2019 | 1 | 1.3 x 0.9 | Lung- left upper lobe | Microwave |
| 6-12-2019 | 1 | 1.2 x 1.1 | Lung- right upper lobe | Microwave |
| 6-25-2019 | 1 | 2.8 x 2.5 | Lung- left lower lobe | Brachytherapy |
| 6-26-2019 | 1 | 1.5 x 1.0 | Left buttock | Cryoablation |
| 7-17-2019 | 1 | 0.8 x 0.7 | Left subcutaneous anterior abdominal wall | Cryoablation |
| 8-5-2019 | 1 | 2.4 x 1.8 | Right upper quadrant omentum | Brachytherapy |
| 8-26-2019 | 1 | 0.9 x 0.8 | Lung- Right upper lobe | Microwave |
| 9-9-2019 | 2 | 1.0 0.7 |
Lung- Left upper lobe | Microwave |
| 9-23-2019 | 1 | 0.5 x 0.5 | Lung- Right lower lobe | Microwave |
| 10-21-2019 | 2 | 0.6 x 0.5 0.7 x 0.6 |
Lung- Left upper lobe | Microwave |
| 11-4-2019 | 1 | 1.7 x 1.6 | Lung – Posterior right upper lobe | Microwave |
| 11-19-2019 | 2 | 1.5 1.6 |
Kidney – Left lower pole | Microwave |
| 11-19-2019 | 1 | 1.7 | Right retroperitoneum | Microwave |
| 12-23-2019 | 2 | 0.8 x.0.7 0.2 x 0.2 |
Lung – Right middle lobe | Microwave |
| 1-22-2020 | 1 | 1.3 | Right paraspinal musculature | Cryoablation |
| 1-22-2020 | 1 | 1.2 | Kidney | Microwave |
| 2-10-2020 | 1 | 1.6 x 1.5 | Lung – Left lower lobe | Microwave |
| 2-19-2020 | 4 | 2.2 1.3 1.0 0.8 |
Liver – Segments 5/6, 7 and 8 | Microwave |
| 2-24-2020 | 2 | 0.7 x 0.7 0.5 x 0.5 |
Lung – Right upper lobe | Microwave |
| 3-9-2020 | 2 | 0.5 x 0.5 0.5 x 0.5 |
Lung – Left lower lobe | Microwave |
| 3-16-2020 | 1 | 4.1 x 3.0 | Lung – Right middle lobe | Brachytherapy |
| 3-23-2020 | 1 | 3.6 x 2.2 | Lung – Left upper lobe | Cryoablation |
| 3-26-2020 | 3 | 1.5 1.3 2.4 |
Liver – Segments 4, 5 and 6 | Microwave |
| 3-31-2020 | 2 | 1.6 x 1.5 0.5 x 0.5 |
Lung – Left upper lobe | Cryoablation |
| 4-6-2020 | 1 | 2.6 x 2.5 | Lung – Lingula | Cryoablation |
| 4-9-2020 | 4 | 3.4 1.0 1.6 4.5 |
Liver – Segments 2, 3 and 4a | Microwave |
| 4-15-2020 | 2 | Ill-defined | Liver – Segments 2 and 3 | Microwave |
| 4-23-2020 | 1 | 2.2 | Left gluteus | Cryoablation |
| 5-11-2020 | 1 | 0.9 x 0.8 | Lung – Right upper lobe | Cryoablation |
| 5-28-2020 | 1 | 2.8 x 2.2 | Left Iliopsoas | Brachytherapy |
Discussion
Successful treatment of leiomyosarcoma is challenging. Although surgical resection of the primary tumor is the treatment of choice, recurrence can be as high as 40-77% [4]. Treatment for metastatic leiomyosarcomas includes surgical or adjuvant chemotherapy; however, advances in systemic treatment have not been forthcoming for several decades. Promising results from a phase Ib/II study suggested that the combination of olaratumab, a humanized monoclonal Antiplatelet-Derived Growth Factor Receptor alpha antibody (PDGFRα), in combination with doxorubicin, improved overall survival [32] leading to accelerated approval of olaratumab by the FDA in October 2016 and addition to the NCCN Guidelines as part of standard treatment for Soft Tissue Sarcoma (STS). However, the efficacy of these phase II results was not supported in a subsequent phase III trial, leading to changes in the NCCN Guidelines to remove the recommendation for olaratumab in combination with doxorubicin [33-35] and a return to the use of doxorubicin alone as the recommended single agent for first-line therapy. Other systemic treatments, such as ifosfamide, gemcitabine and docetaxel, pazopanib, trabectedin, and dacarbazine, were used in the subsequent lines of therapy. Overall survival in a population of patients diagnosed with STS and synchronous metastases from 1989 to 2014 revealed only minimal and not significant improvement [36], suggesting only modest advancements in the treatment of STS over this 25 year period. Until the limitations of the existing treatment modalities can be overcome, other approaches are needed to maintain the quality of life and extend the survival of patients with metastatic leiomyosarcoma.
In this case report, we provide an example of a patient who underwent surgical resection of a primary tumor. Following the appearance of metastatic disease, the patient underwent complementary standard first-line chemotherapy with a combination of ablation therapy and brachytherapy to manage the spread of the disease. Ablation therapy of the pulmonary nodules was initiated just prior to systemic treatment with doxorubicin and olaratumab. As the systemic treatment delayed growth only briefly, ablation therapy of pulmonary nodules resumed shortly following the completion of the systemic treatment and continued for another three years with approximately 74 such nodules treated. Local recurrence and the appearance of pulmonary, hepatic, renal, peritoneal, intramuscular, and subcutaneous metastases have been reported late in the course of leiomyosarcoma, indicating poor prognosis [1,2]. In the present case, MWA and cryoablation were used to treat metastases to the liver, kidney, retroperitoneum, subcutis, and gluteus.
The safety and efficacy of ablation techniques including RFA, MWA, and cryoablation have been well documented in the treatment and palliation of metastatic disease, particularly for lung [37-39] and liver lesions [40,41]. Ablation techniques allow multiple rounds of treatment with minimal morbidity owing to the relative sparing of the surrounding tissue [42]. Depending on the lesion location, ablation procedures can be performed in an outpatient setting with short post-procedure observation periods, maintaining a high quality of life in patients requiring frequent treatment. In this case, the patient continued full-time employment, returning to work within 1-2 days following each procedure and recreational hiking at elevation until late in the disease course.
Both cryoablation and MWA were used in this case, with the decision between the methods based primarily on the location of the lesion. Cryoablation is better tolerated during the procedure and recovery, particularly for lesions proximal to or involving the somatically innervated parietal pleura or chest wall, including the intercostal nerve, as the cold temperatures cause analgesia. Additionally, cryoablation was chosen for lesions near sensitive structures such as the mediastinum, as the zone of necrosis can be visualized on CT as the ice is formed during ablation [43]. MWA allows for a shorter procedure with less radiation exposure; hence, if the lesion location does not indicate cryoablation, shared decision-making between the patient and provider is advised.
For metastatic sarcomas, the treatment of metastatic lesions is an important prognostic factor for survival [44,45]. The use of ablation for local control in patients who are not surgical candidates has been reported to extend chemotherapy-free intervals [46,47] and achieve comparable rates of overall survival to surgical metastectomy [48,49]. Despite their success, ablative techniques can be limited to central lesions in close proximity to sensitive structures.
In this case, brachytherapy was used to treat three lung nodules that could not be treated with ablation therapy because of their proximity to vessels and airways. In addition, brachytherapy was used to treat a nodule that was present on the omentum adjacent to the antrum of the stomach and the medial border of the gallbladder to minimize damage to the liver, stomach, colon, and gallbladder. Another nodule was treated with brachytherapy, which was located on the iliopsoas muscle, for which cryoablation was initially attempted but aborted due to proximity to the femoral nerve. High-dose-rate CT-guided interstitial brachytherapy for metastatic lung nodules requires collaboration between the radiation oncologist and thoracic interventionalist. A 17-gauge introducer coaxial needle with a 4 french flexiguide sheath was placed in the lesion under CT guidance. Using this device, simulation radiography, three-dimensional computerized dosimetry, and single-fraction high-dose-rate brachytherapy with iridium-192 were performed. Previous studies have reported high local control rates for both primary and metastatic lung tumors reaching 100% and 96.88% for six and 12-months, respectively, for low-dose-rate brachytherapy [50], as well as single- and multifraction high-dose-rate brachytherapy reaching 96.2% for two-years [51-54]. While there is growing interest in brachytherapy for pulmonary metastasis, its clinical use is rare due to limited data and the highly specialized expertise required. This case highlights the potential utility of interstitial brachytherapy as part of the multimodal treatment of metastatic leiomyosarcoma, particularly for lesions too close to sensitive structures to be treated with ablative techniques.
It is well known that several forms of local control, such as surgical resection and Stereotactic Body Radiation Therapy (SBRT), are associated with worsening of pulmonary function leading to a decrease in quality of life. For instance, cumulative decline of FEV1 can occur up to 5% postoperatively for thoracoscopic wedge resections, 3-11% for segmentectomy, and 9-16% after lobectomy [55-57]. For SBRT, although the degree of pulmonary function decline is generally less than surgical resection, it is also reported to have decline of FVC of 5.7%, FEV1 of 4.1%, DLCO of 5.2%, and TLC of 3.6% after one year from Stone et al [58]. For the purposes of mitigating pulmonary function decline and preservation of quality of life, ablative therapy is the treatment of choice. The RAPTURE and ACOSOG Z4033 trials both have shown no significant worsening of pulmonary function post-RFA of the lung, leading to optimal preservation of quality of life [59,60]. In addition, ECLIPSE trial also proved that cryoablation in the setting of oligometastatic disease of the lung show preservation of quality of life [61]. Although presented as an atypical use of local therapies in the setting of limited options for widespread disease control, the ability of ablative therapies to provide the most optimal preservation of quality of life cannot be understated.
Conclusion
The median survival time of patients with metastatic soft tissue sarcomas is only 12-15 months [62]. The treatment options for sarcomas remain limited, and surgical removal or its equivalent remains the best means of control. In the case of leiomyosarcoma presented here, the initial chemotherapy provided only temporary control of the disease once metastasis was detected, following surgical resection of the primary tumor. The development of ablation and brachytherapy techniques for many of the locations in which tumors can arise offers a complementary approach for the local control of this disease. 74 metastases in the lung and 28 others that appeared in other locations, including the liver, kidney, subcutis, musculature, and retroperitoneum, were treated by either ablation or brachytherapy over the course of three years. Given that metastases arose in every lobe of the lung during this period, surgery may not have been an effective means of control. In addition, subsequent metastasis to multiple other locations would have precluded a surgical approach. Our case report highlights the contribution of ablation and brachytherapy to the management of the metastatic spread of the disease. Ablation offers advantages over surgical resection, given its greater flexibility, ease of procedure, shorter recovery time, and greater conservation of tissue and organ function. Despite the large number of ablations, the patient maintained a good quality of life and remained fully employed late in the course of metastatic spread of the disease. Thus, ablation therapy and brachytherapy can serve as important complementary modalities to existing treatment options.
References
- Vandergriff T, Krathen R, Orengo I. Cutaneous metastasis of leiomyosarcoma. Dermatol Surg. 2007; 33: 634.
- Barbetakis N, et al. Cutaneous skull metastasis from uterine leiomyosarcoma: A case report. World J. Surg. Oncol. 2009; 7: 45.
- O’Sullivan PJ, Harris AC, Munk PL. Radiological imaging features of non-uterine leiomyosarcoma. British Journal of Radiology. 2008; 81: 73-81.
- Hartman DS, Hayes WS, Choyke PL, Tibbetts GP. From the archives of the AFIP. Leiomyosarcoma of the retroperitoneum and inferior vena cava: radiologic-pathologic correlation. Radiographics: A review publication of the Radiological Society of North America, Inc. 1992; 12: 1203-1220.
- Prieto Muñoz I, Pardo Masferrer J. Scalp Metastasis from Leiomyosarcoma of the Inferior Vena Cava Sign as the First Clinical Sign: A Case Report. Case Rep. Oncol. Med. 2012; 2012: 1-3.
- Burgos Sánchez AJ, Papi M, Talavera J, Trigueros M. Metástasis a glándula submaxilar de leiomiosarcoma uterino. Acta Otorrinolaringol. Esp. 2002; 53: 67-70.
- O’Brien JM. et al. Skeletal muscle metastasis from uterine leiomyosarcoma. Skeletal Radiol. 2004; 33: 655-659.
- Koh YS, Kim JC, Cho CK, Kim HJ. Pancreatic metastasis of leiomyosarcoma in the right thigh: A case report. World J. Gastroenterol. 2007; 13: 1135-1137.
- Subramanian S, Kumar M. Bowel metastases from primary leiomyosarcoma of the gluteal region. Singapore Medf. 2008; 49.
- Burgos Sánchez AJ, Papi M, Talavera J, Trigueros M. Metástasis a glándula submaxilar de leiomiosarcoma uterino. Acta Otorrinolaringol. Esp. 2002; 53: 67-70.
- Burke JP, Maguire D, Dillon J, Moriarty M, O’Toole GC. Whipple’s procedure for an oligometastasis to the pancreas from a leiomyosarcoma of the thigh. Ir. J. Med. Sci. 2012; 181: 361-363.
- Calleja AM, Wellnitz CV, Alharthi MS, Khandheria BK, Chaliki HP. Extensive Cardiac Metastases Secondary to Uterine Leiomyosarcoma. J. Am. Soc. Echocardiogr.2009; 22: 1419.e5-1419.e7.
- Courtney MW, Levine EA. Uterine leiomyosarcoma metastatic to soft tissue of the flank following a ten-year disease-free interval. South. Med. J. 2009; 102: 325-326.
- Ishigure K. et al. Pancreatic metastasis from leiomyosarcoma in the back. Hepatogastroenterology. 2003; 50: 1675-1677.
- Mizuno T, Imai A, Hirose Y. Skeletal muscle metastatic and pelvic leiomyosarcomas following hysterectomy. Int. J. Gynecol. Obstet. 2007; 96: 49-50.
- Sultana N, Pikaart D, Ahmad S, DeNardis S, Finkler N. Paraovarian leiomyosarcoma with scalp metastasis: A case report. Eur J Gynaecol Oncol. 2009; 30: 566-567.
- Arslan E, Kuzeyl K, Çakir E, Res A. Temporalis Muscle Metastasis of the Uterine Leiomyosarcoma: A Case Report . Turk. Neurosurg. 2008; 18: 215-218.
- McWilliams JP, et al. Percutaneous ablation of hepatocellular carcinoma: Current status. Journal of Vascular and Interventional Radiology. 2010; 21.
- Abtin F, et al. Percutaneous Cryoablation for the Treatment of Recurrent Malignant Pleural Mesothelioma: Safety, Early-Term Efficacy, and Predictors of Local Recurrence. J. Vasc. Interv. Radiol. 2017; 28: 213-221.
- Tafti BA, Genshaft S, Suh R, Abtin F. Lung Ablation: Indications and Techniques. Semin. Intervent. Radiol.2019; 36: 163-175.
- Abtin F, et al. Updates on Current Role and Practice of Lung Ablation. J. Thorac. Imaging 2019; 34: 266-277.
- Chen T, et al. Intraoperative test stimulation versus stereotactic accuracy as a surgical end point: A comparison of essential tremor outcomes after ventral intermediate nucleus deep brain stimulation. J. Neurosurg. 2018; 129: 290-298.
- Suh R, Reckamp K, Zeidler M, Cameron R. Radiofrequency ablation in lung cancer: Promising results in safety and efficacy. Oncol. willist. Park. 2005; 19: 12-21.
- Shakeri S, Raman SS. Trends in Percutaneous Thermal Ablation Therapies in the Treatment of T1a Renal Cell Carcinomas Rather than Partial Nephrectomy/Radical Nephrectomy. Semin. Intervent. Radiol. 2019; 36: 183-193.
- Shakeri S, et al. The effect of tumor size and location on efficacy and safety of US- and CT- guided percutaneous microwave ablation in renal cell carcinomas. Abdom. Radiol. 2019; 44: 2308-2315.
- Xu MJ, et al. Single-fraction brachytherapy as monotherapy for early-stage prostate cancer: The UCSF experience. Brachytherapy. 2019; 18: 470-476.
- Chen CP, et al. Salvage HDR brachytherapy for recurrent prostate cancer after previous definitive radiation therapy: 5-year outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2013; 86: 324-329.
- Iyengar P, Lau S, Donington JS, Suh RD. Local Therapy for Limited Metastatic Non-Small Cell Lung Cancer: What Are the Options and Is There a Benefit? Am. Soc. Clin. Oncol. Educ. B. 2016; 35: e460-e467.
- McClure TD, et al. Intermediate outcomes and predictors of efficacy in the radiofrequency ablation of 100 pathologically proven renal cell carcinomas. J. Vasc. Interv. Radiol. 2014; 25: 1682-1688.
- Tong MJ, Rosinski AA, Huynh CT, Raman SS, Lu DSK. Long-term survival after surveillance and treatment in patients with chronic viral hepatitis and hepatocellular carcinoma. Hepatol. Commun. 2017; 1: 595-608.
- Lee MW, et al. Radiofrequency ablation of hepatocellular carcinoma as bridge therapy to liver transplantation: A 10-year intention-to-treat analysis. Hepatology. 2017; 65: 1979-1990.
- Tap WD, et al. Olaratumab and doxorubicin versus doxorubicin alone for treatment of soft-tissue sarcoma: an open-label phase 1b and randomised phase 2 trial. Lancet. 2016; 388: 488-497.
- Seeber A, et al. Olaratumab plus anthracyline in advanced/metastatic soft tissue sarcoma: Data of real-world utilization in Austria. Wien. Klin. Wochenschr. 2019.
- Herold R, et al. Revocation of the conditional marketing authorisation of a cancer medicine: The olaratumab experience. European Journal of Cancer. 2019; 123: 25-27.
- US Food & Drug Administration. Olaratumab (LARTRUVO). FDA statement. 2019.
- Vos M, Ho VKY, Oosten AW, Verhoef C, Sleijfer S. Minimal Increase in Survival Throughout the Years in Patients with Soft Tissue Sarcoma with Synchronous Metastases: Results of a Population-Based Study. Oncologist 2019; 24.
- De Baere T, et al. Evaluating cryoablation of metastatic lung tumors in patients-safety and efficacy the ECLIPSE trial-interim analysis at 1 year. J. Thorac. Oncol. 2015; 10: 1468-1474.
- Callstrom MR, et al. Multicenter Study of Metastatic Lung Tumors Targeted by Interventional Cryoablation Evaluation (SOLSTICE). in Journal of Thoracic Oncology. 2020; 15: 1200-1209.
- Lencioni R, et al. Response to radiofrequency ablation of pulmonary tumours: A prospective, intention-to-treat, multicentre clinical trial (the RAPTURE study). Lancet Oncol. 2008; 9: 621-628.
- De Baere T, et al. Radiofrequency ablation of 100 metastases with a mean follow-up of more than 1 year. Am. J. Roentgenol. 2000; 175: 1619-1625.
- Meijerink MR, et al. Radiofrequency and Microwave Ablation Compared to Systemic Chemotherapy and to Partial Hepatectomy in the Treatment of Colorectal Liver Metastases: A Systematic Review and Meta-Analysis. CardioVascular and Interventional Radiology. 2018; 41: 1189-1204.
- Quirk MT, Pomykala KL, Suh RD. Current Readings: Percutaneous Ablation for Pulmonary Metastatic Disease. Semin. Thorac. Cardiovasc. Surg. 2014; 26: 239-248.
- Eiken PW, Welch BT. Cryoablation of Lung Metastases: Review of Recent Literature and Ablation Technique. Seminars in Interventional Radiology. 2019; 36: 319-325.
- Weiser MR, Downey RJ, Leung DHY, Brennan MF. Repeat resection of pulmonary metastases in patients with soft-tissue sarcoma. J. Am. Coll. Surg. 2000; 191: 184-190.
- Chudgar NP, et al. Is Repeat Pulmonary Metastasectomy Indicated for Soft Tissue Sarcoma? in Annals of Thoracic Surgery. 2017; 104: 1837-1845.
- Sutton C, et al. Analysis of the Chemotherapy-Free Interval following Image-Guided Ablation in Sarcoma Patients. Sarcoma. 2020; 2020.
- Gravel G, et al. Percutaneous thermal ablation: A new treatment line in the multidisciplinary management of metastatic leiomyosarcoma? Eur. J. Surg. Oncol. 2017; 43: 181-187.
- Falk AT, et al. Effect on survival of local ablative treatment of metastases from sarcomas: A study of the french sarcoma group. Clin. Oncol. 2015; 27: 48-55.
- Tetta C, et al. Non-surgical Treatments for Lung Metastases in Patients with soft Tissue Sarcoma: Stereotactic Body Radiation Therapy (SBRT) and Radiofrequency Ablation (RFA). Curr. Med. Imaging Former. Curr. Med. Imaging Rev. 2020; 16: 1-14.
- Liu B, et al. Salvage treatment of NSCLC recurrence after first-line chemotherapy failure: Iodine-125 seed brachytherapy or microwave ablation? Thorac. Cancer. 2020; 11: 697-703.
- Ricke J, et al. CT-guided interstitial single-fraction brachytherapy of lung tumors: Phase I results of a novel technique. Chest. 2005; 127: 2237-2242.
- Peters N, et al. CT-guided interstitial brachytherapy of primary and secondary lung malignancies: Results of a prospective phase II trial. Strahlentherapie und Onkol. 2008; 184: 296-301.
- Tselis N, et al. Computed tomography-guided interstitial high-dose-rate brachytherapy in the local treatment of primary and secondary intrathoracic malignancies. J. Thorac. Oncol. 2011; 6: 545-552.
- Yoon SM, Suh R, Abtin F, et al. Outcomes with multi-disciplinary management of central lung tumors with CT-guided percutaneous high dose rate brachyablation. Radiat Oncol. 2021; 16: 99.
- Welter S, Cheufou D, Sommerwerck U, Maletzki F, Stamatis G. Changes in lung function parameters after wedge resections: a prospective evaluation of patients undergoing metastasectomy. Chest. 2012; 141: 1482-1489.
- Harada H, Okada M, Sakamoto T, Matsuoka H, Tsubota N. Functional advantage after radical segmentectomy versus lobectomy for lung cancer. Ann Thorac Surg. 2005; 80: 2041-2045.
- Nomori H, Mori T, Ikeda K, Yoshimoto K, Iyama K, et al. Segmentectomy for selected cT1N0M0 non-small cell lung cancer: a prospective study at a single institute. J Thorac Cardiovasc Surg. 2012; 144: 87-93.
- Stone B, Mangona VS, Johnson MD, Ye H, Grills IS. Changes in Pulmonary Function Following Image-Guided Stereotactic Lung Radiotherapy: Neither Lower Baseline Nor Post-SBRT Pulmonary Function Are Associated with Worse Overall Survival. J Thorac Oncol. 2015; 10: 1762-1769.
- Lencioni R, Crocetti L, Cioni R, et al. Response to radiofrequency ablation of pulmonary tumours: A prospective, intention-to-treat, multicentre clinical trial (the RAPTURE study). Lancet Oncol. 2008; 9: 621-628.
- Alexander ES, Xiong L, Baird GL, Fernando H, Dupuy DE. CT Densitometry and Morphology of Radiofrequency-Ablated Stage IA Non-Small Cell Lung Cancer: Results from the American College of Surgeons Oncology Group Z4033 (Alliance) Trial. J Vasc Interv Radiol. 2020; 31: 286-293.
- de Baère T, Woodrum D, Tselikas L, et al. The ECLIPSE Study: Efficacy of Cryoablation on Metastatic Lung Tumors With a 5-Year Follow-Up. J Thorac Oncol. 2021; 16: 1840-1849.
- Demetri GD, et al. Efficacy and safety of trabectedin or dacarbazine for metastatic liposarcoma or leiomyosarcoma after failure of conventional chemotherapy: Results of a phase III randomized multicenter clinical trial. J. Clin. Oncol. 2016; 34: 786-793.