
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A review of carotid endarterectomy in a patient with severe carotid artery stenosis and a review of related literature
Jianping Zhang1#; Xiangji Lu2#; Gang Yang3#; Xinwei Zhu1; Jingang Bao1; Yongfei Xin1; Xiaodong Wang2*; Ri Le Wu1*
1Inner Mongolia Autonomous Region People’s Hospital Emergency Cerebrovascular Department, Hohhot, China.
2Inner Mongolia Autonomous Region General Hospital,PAP, Hohhot, China.
3Department of Cardiothoracic Surgery, Central Theater Command General Hospital, WuHan, China.
#Equal Contribution.
*Corresponding Author : Wang X1; Wu RL2
1Inner Mongolia Autonomous Region People’s Hospital Emergency Cerebrovascular Department, Hohhot, China.
2Inner Mongolia Autonomous Region General Hospital, PAP, Hohhot, China.
Email: 302758945@qq.com;
wurile@hotmail.com
Received : Jul 12, 2023
Accepted : Jul 28, 2023
Published : Aug 04, 2023
Archived : www.jcimcr.org
Copyright : © Wang X & RL W (2023).
Abstract
At present, cerebral infarction has become a serious disease that endangers human health, and one of the important reasons for cerebral infarction is carotid artery stenosis. Carotid Endarterectomy (CEA)is a surgical procedure to treat carotid artery stenosis, Its principle is to remove carotid plaque and relieve carotid artery stenosis, thereby increasing the distal cerebral blood supply and preventing cerebral infarction. Carotid endarterectomy was first performed on patients in 1953 by Professor De Bakey of vascular surgery and has been used for more than 60 years. Due to its effectiveness in the treatment of carotid artery stenosis, it has become an important routine operation in neurosurgery and cerebrovascular department, greatly reducing the risk of stroke in patients. In particular, a large number of clinical trials were represented by the North American Endarterectomy Trial for Symptomatic Carotid Stenosis (NASCET) [1], the European Carotid Surgery Trial (ECST) [2], the Asymptomatic Carotid Stenosis versus Aspirin Trial (CASANOVA) [3], and the Asymptomatic Carotid Surgery Trial (ACST) [4]. After the results of the bed trial were published successively, the effective role of CEA in the treatment of carotid atherosclerotic stenosis became more clear, and the status of CEA was further consolidated. This paper reports a case of carotid endarterectomy and reviews the relevant literature.
Keywords: Cerebral infarction; Carotid artery stenosis; Carotid endarterectomy.
Abbreviations: CEA: Carotid Endarterectomy; NASCET: North American Endarterectomy Trial For Symptomatic Carotid Stenosis; ECST: European Carotid Surgery Trial; ACST: Asymptomatic Carotid Surgery Trial.
Citation: Zhang J, Lu X, Yang G, Wang X, Wu RL, et al. A review of carotid endarterectomy in a patient with severe carotid artery stenosis and a review of related literature. J Clin Images Med Case Rep. 2023; 4(8): 2530.
Introduction
The Emergency cerebrovascular Department of Inner Mongolia Autonomous Region Hospital is located in Hohhot, the capital city of Inner Mongolia Autonomous Region. The main business scope of the department involves the diagnosis and treatment of cerebrovascular diseases, including cerebrovascular intervention and carotid plaque stripping. In recent years, we have selected each patient strictly according to the indications, from admission examination evaluation to halfway treatment and discharge, the treatment level is thriving, and the postoperative effect is good. The case of carotid artery dissection reported below is a case of our dedicated treatment at the beginning of this year, the patient was followed up after discharge, the effect was good, and the patient was recognized.
Case presentation
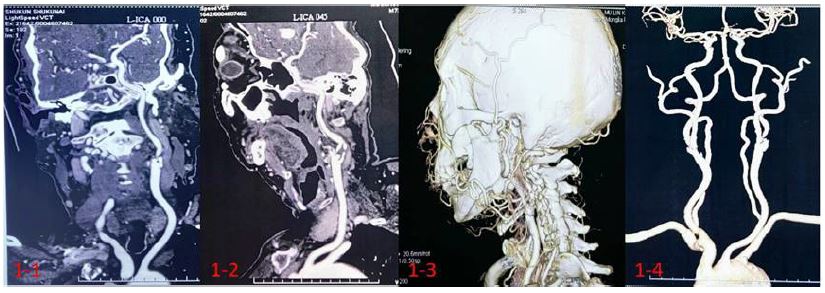
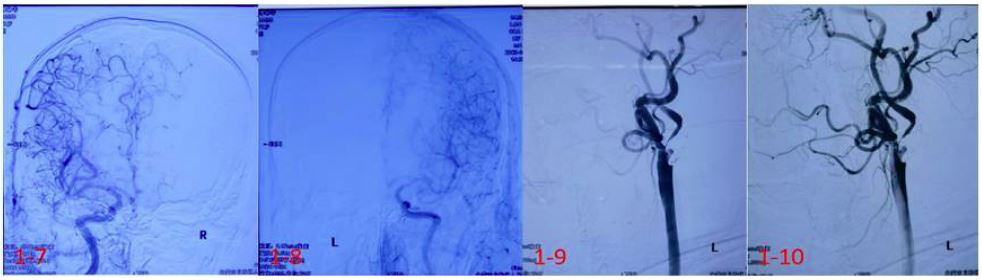
73-year-old male patient presented with “dizziness with transient right limb weakness for 1 month.” It was admitted to the department of cerebrohematology on January 5, 2023. According to the patient, dizziness, no spinning, and blurred vision occurred one month before admission without obvious causes. Transient right limb weakness occurred for 5 times, during which the right upper limb could not hold the object, and the right lower limb stiffness was relieved after a few minutes, without unsteady gait, nausea, and vomiting, so the patient was admitted to the local hospital. Cervical color ultrasound was performed: Severe stenosis of the initial segment of the left internal carotid artery (stenosis rate 70-99%). At that time, no treatment was performed, and she returned home for self-observation. He is now undergoing further treatment in the outpatient department of our hospital. The outpatient clinic was admitted to the ward as “left carotid artery stenosis”. The man suffered from hypertension for 7 years, and his blood pressure was stable with regular oral administration of amlodipine besy late tablets. Denied diabetes, coronary heart disease history. Smoking history of more than 40 years, an average of 20 cigarettes/day, occasionally drinking alcohol. Head and neck CTA after admission: Severe stenosis in the initial segment of the left internal carotid artery (A: Figure 1-1, Figure 1-2, Figure 1-3, Figure 1-4); Cranial DWI+ASL: Multiple lacunar infarction, left cerebral hemisphere hypoperfusion (B: Figures 1-5 and 1-6); DSA: Severe stenosis of the initial segment of the left internal carotid artery and significantly reduced blood flow in the left cerebral hemisphere (C: Figure 1-7, Figure 1-8, Figure 1-9, Figure 1-10). Considering that the patient had been diagnosed for more than one month and was in good condition with no obvious positive signs of nervous system after physical examination, we performed carotid artery dissection in strict accordance with Handbook of Neurosurgery, 8e [5] after completing the examination.



Anticoagulant drugs were routinely administered before surgery. For patients who normally take aspirin orally for a year, 100 mg, QD, more than 1 month, there is no need to change the drug, continue to take aspirin 100 mg until the day of surgery. If less than 1 month, start increasing to 300 mg 3 days before surgery. Thrombologram can be used to measure the anticoagulation effect more individually.
Brief course of operation: After the obvious effect of general anesthesia, supine position was taken. Tilt the head back slightly, pillow circle under the head, put a thin pillow under the left shoulder blade, raise 15°-20°. Turn your head to the right by 45°-60° (Figure 2-1). Three bony marks of mastoid process, mandibular Angle and suprasternal fossa were marked. Routine disinfection and placement of sterile surgical towels. Incision was made on the anterior edge of the left sternocleidomastoid muscle with a length of about 6 cm. The skin, subcutaneous, and platysma muscles were cut, and the carotid sheath was separated and exposed layer by layer along the anterior edge of the sternocleidomastoid muscle. The common carotid artery, internal carotid artery, external carotid artery, and superior thyroid artery were separated and exposed by opening the H-carotid sheath (Figure 2-2). 3000 units of heparin were injected intravenously, methylene blue lines were drawn, and vascular blocking forceps and two aneurysm clips successively blocked the superior thyroid artery, external carotid artery, common carotid artery, and internal carotid artery, raising blood pressure by 20 mmHg (Figure 2-3). A longitudinal incision of the carotid artery was made under the microscope, and the carotid plaque was removed. Ulcers, large lipid cores, and calcification were found on the surface of the plaque (Figure 2-4, A, B). Heparin saline irrigation was used to remove free intimal debris (Figure 2-5). After continuous 6-0 Proline suture, the carotid lumen was filled with heparin saline and then the superior thyroid artery, external carotid artery, common carotid artery, and internal carotid artery were released successively without active bleeding, and hemostatic gauze was attached to the incision (Figure 2-6). Suture the arterial sheath, place an indwelling drainage tube outside the carotid sheath. Suture platysma muscle, subcutaneous, skin. After operation, the patient was awake, the tracheal intubation was removed, and safely returned to the ward.
Key points of postoperative observation [6]: Changes in pupil size should be observed immediately after surgery to prevent cerebral infarction or cerebral hemorrhage. In particular, surgical stimulation of the sympathetic nerve in the neck may lead to abnormally large pupils after surgery, and the surgeon should know. After awakening from anesthesia, the consciousness and physical activity should be observed. Pay attention to the postoperative blood pressure control, maintain the basic blood pressure level or slightly lower, to prevent the occurrence of postoperative hyperperfusion syndrome. The patient was examined for hoarseness (recurrent laryngeal nerve), water choking cough (superior laryngeal nerve), and facial paralysis (mandibular and cervical branches of facial nerve). There is no neck weakness (accessory nerve). Pay special attention to the occurrence of several serious complications: 1. Cerebral infarction or cerebral hemorrhage; 2. Hyperperfusion, cerebral edema, cerebral hemorrhage; 3. Arterial rupture and bleeding.
Discussion
Choices about anesthesia. Most of the centers in China use general anesthesia surgery, general anesthesia is more suitable for patients, such as sensory experience, the stability of vital signs during the operation; Compared with general anesthesia, local anesthesia can observe the changes in the nervous system signs of patients after blood flow blockade in real time, so the utilization rate of bypass will be reduced. However, local anesthesia has higher technical requirements for surgeons and anesthesiologists, which will bring additional risks and pain to patients. Therefore, the choice of anesthesia lies in the habit of different centers, and general anesthesia is commonly used by individuals.About intraoperative monitoring. The purpose of intraoperative monitoring is to identify changes in cerebral blood flow during carotid artery occlusion and opening, thereby reducing surgical risk. At present, the main monitoring methods include Transcranial Doppler (TCD), cerebral oxygen saturation, stump pressure, Electroencephalography (EEG), evoked potential, jugular vein saturation and jugular vein lactic acid level, etc. It is not yet possible to determine which one has the best specificity and accuracy.About the choice of surgical approach. For CEA, the anatomical marks are clear and the level is simple, but due to various variations or other factors, there are still some problems to be discussed in terms of surgical approach [1]. Longitudinal incision or transverse incision: CEA generally selects the longitudinal incision of the front edge of the sternocleidomastoid muscle. The advantage is that it is easy to expose the mandibular Angle and sternal Angle, which can be applied to both high and low surgery, but the postoperative scar is very ugly; The transverse incision is made along the texture of the neck skin, which can be aesthetically preserved, but the exposure is limited when the lesion is extensive or the operation requires the use of bypass. The two incisions are generally selected individually according to the patient’s condition and the doctor’s experience [2]. Medial or lateral jugular vein approach: After platysma incision, generally choose to go through the internal jugular vein to expose the bifurcation of the carotid artery, ligation the transverse branches from the internal jugular vein and external jugular vein along the way, and expose the hypolingual nerve to prevent damage, expose the neck loop, if necessary, can also cut the neck loop, expose the sternocleidomastoid artery, vagus nerve, etc.
The lateral jugular vein approach is selected. The internal jugular vein needs to be pulled medial during the operation, and 1-2 small branch blood vessels from the sternocleidomastoid muscle may be imported laterally from the internal jugular vein. Some nerve fibers emanating from the neck loop need to be severed by this approach, and the vagus nerve must be separated from the posterior wall of the internal carotid artery. To prevent damage to the vagus nerve during traction, resulting in postoperative hoarseness.
Compared with the two approaches, the lateral approach of the internal jugular vein has better exposure to the front and distal end of the internal carotid artery. At the same time, because there is no need to deal with the transverse branch of the jugular vein, the operation is simple and rapid, generally there is no need to expose the hypoglossal nerve, thus reducing the chance of damage, but it may increase the possibility of hoarseness due to pulling the vagus nerve [3]. Posterior cervical triangle approach: Mainly for the exposure of high CEA, it can expose the internal carotid artery to the level of the first cervical vertebra. A straight incision was made at the posterior margin of sternocleidomastoid muscle, and the superficial auricular nerve and minor occipital nerve were not damaged during the operation. During the operation, the accessory nerve should be separated carefully, and the internal jugular vein and sternocleidomastoid muscle should be pulled forward together to expose the bifurcation of the carotid artery. In order to prevent damage to the vagus nerve, it can be retained behind the carotid artery, and if necessary, it can be free to move forward and medial to prevent damage to the superior laryngeal nerve.
Looking at all surgical methods, different technical methods and improvements are to better solve the problem, so there will be individual differences based on doctor habits and patient conditions, although some methods show better advantages, but in terms of surgical technology itself, there is no advanced and backward points, at present, there is no surgical method can completely replace other methods.
Declarations
Acknowledgement: The authors thank Yang Gang for assistance in the preparation of this paper.
Funding: This work was supported by Natural Science Foundation of Inner Mongolia Autonomous Region [Grants number: 2021MS08108]; Science and Technology Project of Inner Mongolia Autonomous Region [Grants number: 2021GG0114].
References
- Ferguson GG, Eliasziw M, Barr HW, Clagett GP, Barnes RW, et al. The North American Symptomatic Carotid Endarterectomy Trial: Surgical results in 1415 patients. Stroke. 1999; 30: 1751-8.
- Warlow CP. Symptomatic patients: The European Carotid Surgery Trial (ECST). J Mal Vasc. 1993; 18: 198-201.
- Carotid surgery versus medical therapy in asymptomatic carotid stenosis. The CASANOVA Study Group. Stroke. 1991; 22: 1229-35.
- Rudarakanchana N, Dialynas M, Halliday A. Asymptomatic Carotid Surgery Trial-2 (ACST-2): rationale for a randomised clinical trial comparing carotid endarterectomy with carotid artery stenting in patients with asymptomatic carotid artery stenosis. Eur J Vasc Endovasc Surg. 2009; 38: 239-42.
- De Backer A. Handbook of neurosurgery, 8th edition. Acta Chir Belg. 2016; 116: 269.
- Qian Hai. Practical Techniques of Carotid Endarterectomy. Beijing: Science and Technology Press of China.2020; 9.