
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Acute interstitial pneumonia post-COVID infection complicated by secondary bacterial pnuemonia
Etienne Ceci Bonello1*; Caroline Gouder2
1Higher Specialist Trainee Respiratory and General Medicine in Mater Dei Hospital, Malta.
2Consultant Respiratory and General Medicine in Mater Dei Hospital, Malta.
*Corresponding Author : Etienne Ceci Bonello
Higher Specialist Trainee Respiratory and General Medicine in Mater Dei Hospital, Malta.
Email: etienne.ceci@gov.mt
Received : May 02, 2023
Accepted : Jul 31, 2023
Published : Aug 07, 2023
Archived : www.jcimcr.org
Copyright : © Bonello EC (2023).
Citation: Bonello EC, Gouder C. Acute interstitial pneumonia post-COVID infection complicated by secondary bacterial pneumonia. J Clin Images Med Case Rep. 2023; 4(8): 2532.
Case description
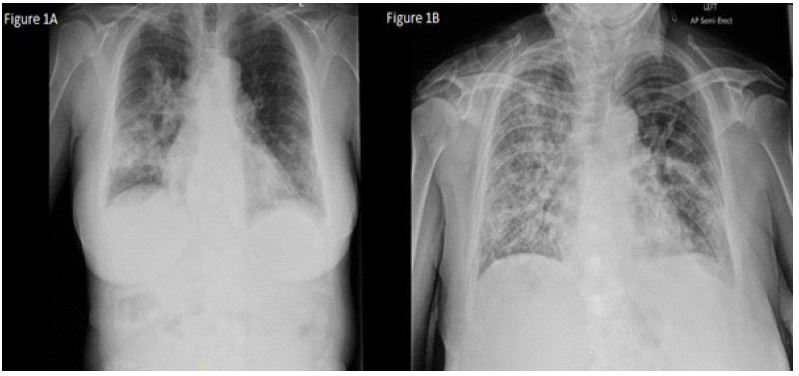
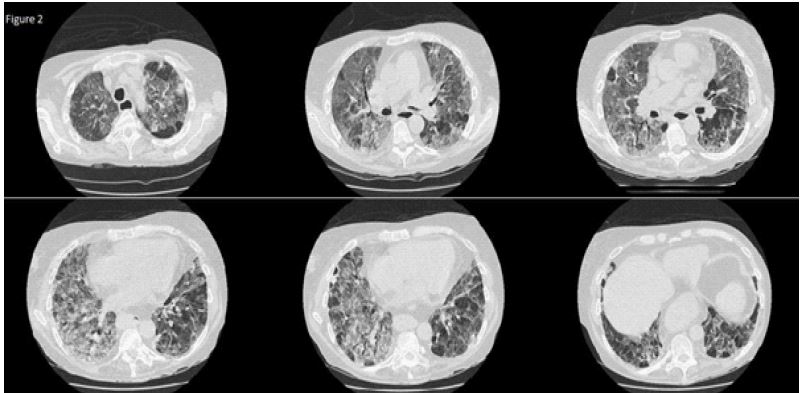
64-year-old lady presented to emergency with dyspnoea, fever, cough and green sputum production for the previous week. She had tested positive for SARS-cov-2 two weeks prior to the onset of these symptoms. Investigations including a Chest X-Ray (CXR) (Figure 1a) confirmed a lower respiratory tract infection, likely a secondary complication to COVID-19 infection. The patient was started on Intravenous (IV) antibiotics with oxygen and cardiovascular support. Two days into her admission, the patient developed severe type 1 respiratory failure needing transfer to a high-dependency unit for Non-Invasive Ventilation (NIV). A repeat CXR indicated Acute Respiratory Distress Syndrome (ARDS) (Figure 1b), most likely post-COVID ARDS complicated with a secondary bacterial infection. A Computed Tomography (CT) scan of the chest (Figure 2) showed widespread Ground Glass (GG) changes, septal thickening and traction bronchiectasis, in keeping with severe acute interstitial pneumonia pattern. The patient was pulsed with IV methylprednisolone 500 mg IV for 3 consecutive days and started on oral prednisolone thereafter at 1 mg/kg/daily (60 mg). Antibiotics were upgraded to meropenem and teicoplanin in view of this deterioration. A steroid-sparing agent was considered, however the patient’s condition improved rapidly and was eventually weaned off NIV within a few days. She is currently receiving oral corticosteroids with a tail down regimen, receiving supplemental oxygen as necessary and is awaiting transfer to a rehabilitation hospital.
Discussion
SARS-cov-2 infection can cause a spectrum of disease from asymptomatic infection to fatal ards. Post-COVID Interstitial Lung Disease (ILD) is a well-known phenomenon described in literature. AIP is a rare form of diffuse lung injury with a fulminant onset characterised by rapidly progressive hypoxemic respiratory failure refractory to standard treatment. The aetiology is uncertain. HRCT typically shows bilateral, patchy, symmetricareas of GG attenuation, often accompanied by consolidation, septal thickening, and traction bronchiectasis. Early treatment is vital. Pulsed methylprednisolone 500 mg - 1 g for three consecutive days is first-line therapy. Thereafter, maintenance therapy (0.5 – 1 mg/kg/day prednisolone orequivalent) is given. It is usual to assess the response to corticosteroid therapy after initial treatment before considering second-line agents such as cyclophosphamide. Lung transplantation may be a final resort if the patient remains dependent on oxygen and established ILD [1-3].
References
- Myall KJ, Martinovic JL, West A. How COVID-19 interacts with interstitial lung disease. Breathe. 2022; 18: 210158.
- Wells AU, Hirani N. Interstitial lung disease guideline. Thorax. 2008; 63: v1-v58.
- Avnon LS, Pikovsky O, Sion-Vardy N, Almog Y. Acute interstitial pneumonia-Hamman-Rich syndrome: Clinical characteristics and diagnostic and therapeutic considerations. Anesthanalg. 2009; 108: 232-237.