
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Acute myocardial infarction induced by migration of iodine-125 seeds
Yijing Guo; Hong Shen; Zhifeng Dong; Juanjuan Zhang; Chengxing Shen; Xian Jin*
Department of Cardiology, Shanghai Jiao Tong University Affiliated Sixth People’s Hospital, No. 600, Yishan Road, Shanghai 200233, China.
*Corresponding Author : Xian Jin
Department of Cardiology, Shanghai Jiao Tong University Affiliated Sixth People’s Hospital, No. 600, Yishan Road, Shanghai 200233, China.
Tel: +86-18918169127 & +86-021-24056618;
Email: jinxianian@126.com
Received : Jul 12, 2023
Accepted : Aug 01, 2023
Published : Aug 08, 2023
Archived : www.jcimcr.org
Copyright : © Jin X (2023).
Abstract
Background: Iodine-125 seeds are used for brachytherapy of several tumors, which are considered to be relatively safe with rare complications.
Case summary: Here we report a case of acute myocardial infarction induced by Iodine-125 seeds migrating to right coronary artery. A 72-year-old male patient was diagnosed with colorectal cancer in 2019. After surgery, metastatic foci were found in liver and lung during the follow-up examinations. Thus, he was admitted to receiving iodine-125 seeds implantation for brachytherapy. However, he suffered chest pain and became unconscious 6 hours after seeds implantation in the lung. Electrocardiogram showed atrial fibrillation and signs of inferior myocardial infarction with II, III, aVF ST segment elevation. On the way to cardiac catheterization room, patient experienced Adams-Stoke syndrome caused by ventricular tachycardia. After cardiopulmonary resuscitation, electrical conversion, tracheal intubation and medication treatment, patient’s condition became relatively stable and percutaneous coronary intervention was performed subsequently. Related examinations detected other migrated seeds (3 in right arm and another one in the heart apart from 2 in the right coronary artery).
Discussion: To our knowledge, this is the first report of iodine-125 seeds migration leading to acute myocardial infarction which is explicitly caused by blockage of coronary artery within 6 hours after seeds implantation. Thus, optimizing seeds implantation procedure and standardizing monitoring procedure should be taken into consideration in the future.
Learning Points: Severe embolism could happen after iodine-125 seeds implantation, which emphasizes the significance of close monitor of patients after the procedure. Special intervention strategies should be taken for such special acute myocardial infarction caused by seed migration. Optimizing seeds implantation procedure, such as using CT-guided technology, should be taken into consideration for patients’ safety in the future work.
Keywords: Iodine-125, Brachytherapy; Seeds migration; Myocardial Infarction.
Abbreviations: ECG: Electrocardiogram; CT: Computed Tomography; ECT: Emission Computed Tomography; CPR: Cardiopulmonary Resuscitation; RCA: Right Coronary Artery; AMI: Acute Myocardial Infarction; LVEF: Left Ventricular Ejection Fraction; PCI: Percutaneous Coronary Intervention; STEMI: ST: Segment Elevation Myocardial Infarction.
Citation: Guo Y, Shen H, Dong Z, Zhang J, Jin X, et al. Acute myocardial infarction induced by migration of iodine-125 seeds. J Clin Images Med Case Rep. 2023; 4(8): 2534.
Introduction
Permanent radioactive seed implantation is one of the well-acknowledged treatments for solid tumor [1]. According to recent studies, it is effective and safe in treating primary or metastatic cancers including lung and hepatic cancer [2-4]. However, seed migration may cause severe clinical conditions because of its special physical characteristics. There are several case reports and clinical studies describing seed migrating to heart [5,6], in which only one report of Acute Myocardial Infarction (AMI) related to brachytherapy seed 22 months after implantation [7].
Here, we report a case in which Iodine-125 seeds migrated to Right Coronary Artery (RCA) and caused AMI within 6 hours after seeds implantation. To our knowledge, this is the first case explicitly elaborating the causal relationship between seeds migration and the mechanistically blockage of coronary artery rather than chronic radiation lesion.
Case summary
A 72-year-old male patient had colorectal cancer and received sigmoid colon cancer radical resection, as well as transcatheter arterial chemoembolization and iodine-125 seeds implantation in the liver and lung metastatic foci under the guidance of Computed Tomography (CT) during past 2 years. Following CT and Emission Computed Tomography (ECT) scan showed no seeds migration in the upper body (Figure 1). In his recent admission to hospital, another 30 and 60 iodine-125 seeds were implanted by percutaneous puncture in left and right pulmonary metastatic loci respectively.
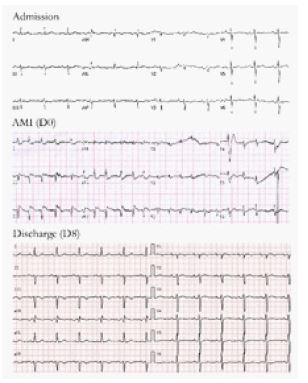
The patient developed mild dyspnea and chest discomfort one hour after iodine-125 seeds implantation in both lung metastatic sites. No special findings were made by consulting physician. Four hours later, patient felt severe chest pain and became unconscious. Electrocardiograph and blood pressure monitor were applied immediately, which revealed pulse of 160bpm, blood pressure of 103/83 mmHg and 100% oxygen saturation. Cardiologist arrived 5 minutes later and performed 12-lead electrocardiogram (ECG) examination that showed atrial fibrillation with II, III, aVF ST segment elevation (Figure 2). After all these examinations and venous access establishment, patient came awake and complained about chest pain and weakness. However, patient suffered ventricular tachycardia on the way to cardiac catheterization room with binocular gaze and hyperspasmia and became unconscious again. Electrocardiograph monitor showed ventricular tachycardia and electrical conversion was performed immediately. Physical examination found pupils dilatation, hyperpnea and negative Babinski sign. Oxygen saturation went down to 60-70%.
Doctors sent the patient back and performed Cardiopulmonary Resuscitation (CPR) immediately. Meanwhile, doctors performed tracheal intubation and provided oxygen with respiratory balloon. Due to repeated ventricular tachycardia and hypotension, electrical conversion along with medication including lidocaine and adrenaline were used. After one-hour resuscitation, patient’s condition became relatively stable. Then he was sent to cardiac catheterization room. Coronary Arteriography (CAG) showed three iodine-125 seeds in the Right Coronary Artery (RCA) and another one lodging in the left coronary system or endocardium. After aspiration through guiding catheter, there were still two seeds locating parallel in the ostium of RCA, mechanically blocked the blood flow entirely (Figure 3a). Subsequently, balloon angioplasty were performed, after which two seeds were moved to the mid part of RCA with partially revascularization. Considering great possible radioactive lesion in the future, we performed balloon angioplasty again and moved two seeds to the distal of artery, after which blood flow in RCA was restored, remaining a 70% stenosis in the proximal and mid portion on RCA (Figure 3b). Meanwhile, CAG showed showed 70-80% stenosis in the left anterior descending artery as well as 50% stenosis in the left circumflex coronary artery (Figure 3c, 4a). In this case, radioactive seeds were deemed the culprit for the inferior wall Acute Myocardial Infarction (AMI). No stent was deployed in the RCA or other coronary arteries.
Following blood tests showed peak troponin-I at 14.541 μg/L, which went down from the second day. Subsequent systematic X-ray fluoroscopy confirmed six migrated seeds including two in RCA, one in the left coronary system or endocardium and three in the right arm (Figure 4). Transthoracic echocardiography showed no left ventricular wall motion abnormality and Left Ventricular Ejection Fraction (LVEF) was 59%. Contrast echocardiography showed no microbubble in left heart at rest or with the Valsalva maneuver, which provided no evidence for foramen ovale, atrial septal defect, or pulmonary arteriovenous malformation. The patient was finally discharged from hospital 8 days after myocardial infarction.
The patient came back for follow-up tests 4 weeks later, in which blood test showed negative troponin-I. Transthoracic echocardiography showed no left ventricular wall motion abnormality and LVEF was in the normal range. Six months later, we performed PCI of his RCA with drug-coated balloon (Figure 5a). In the CAG, three iodine-125 seeds still lodged in the distal of coronary arteries. Besides, the patient received myocardial perfusion imaging (MPI) that showed normal cardiac function and no abnormal signals (Figure 5b). Thus, we believed that these seeds caused little cardiac lesion, which proved the accuracy of our treatment strategy.
Images showed implanted iodine-125 seeds in the liver and left pulmonary metastatic foci with no migrated seeds.
Discussion
Iodine-125 seeds currently used is molded into sticks of 0.5 mm in diameter and cut into carbon bars of 3 mm in length coated with Titanium tubes [8]. Iodine-125 seed shows half-life of 59.7 days, low energy with appropriate radiation range, which makes it widely used in varies of cancers [9]. Studies found that these seeds could inhibit tumor growth by suppressing epithelial-mesenchymal transition and regulating cell death pathways [10,11].
Though there are researchers claiming the safety of iodine-125 seeds implantation, severe complications can happen after such procedure [12]. One major concern is embolization caused by seeds migration. Calvert et al. reported pulmonary embolism due to migrated seeds within the pulmonary arteries in the right upper lobe 6 years after brachytherapy for prostate cancer [13]. Sachdeva et al. reported another severe embolization case in 2006, in which seeds migrated into RCA causing AMI 22 months after seeds implantation [7]. However, there was a 95% stenosis in the lodging position of the seed, which suggested chronic radioactive lesion or preexistent plaque as the pathological factor of this case.

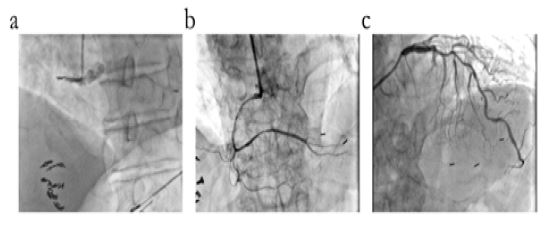
a: Two seeds locating parallel in the ostium of RCA. b: Seeds moved to the distal of RCA. c: Angiogram of left coronary artery.
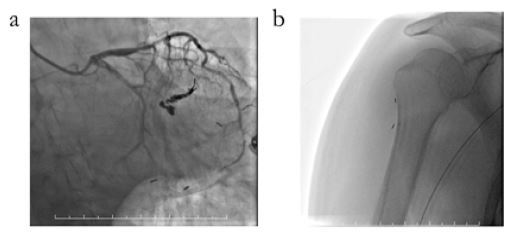
Migrated seeds were found in the left coronary system or endocardium and in the right arm.
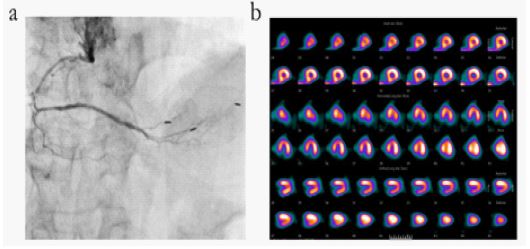
a: PCI of the RCA with drug-coated balloon. b: MPI showed normal cardiac function and no abnormal signal.
The mechanism of seeds migration is an interesting and important question we want to answer. Systematic X-ray fluoroscopy found seven migrated seeds, of which three located in right arm, and four in heart. Because they all come from left heart system, we performed contrast echocardiography which denied the right to left shunting route. Thus, misplacing seeds into pulmonary vein system is the most probable mechanism for this case. Thus, optimizing the protocol of iodine-125 seeds implantation would be the next step for this promising treatment. Wu et al. explored the assistant function of 3-D information for seeds implantation under the guidance of ultrasound [14]. Besides, three-dimensional printing was also used to help finding a safer puncture route [15]. However, whether these methods could help reducing seeds migration or embolism still needs to be further studied.
Fortunately, this patient was saved by in-time CPR and proper Percutaneous Coronary Intervention (PCI) strategy.
Conclusion
This report describes an AMI cause by mechanical blockade of migrated iodine-125 seeds in the RCA 6 hours after seeds implantation. To our knowledge, this is the first report explicitly represents mechanical blockage of coronary artery by radioactive seeds. Thus, close monitoring and standard first-aid treatments should always be strictly taken after seed implantation.
Declarations
Disclosures: There are no relevant disclosures for this work by any of the authors.
Acknowledgments: All authors have acknowledged and approved authorship. ECGs were performed before AMI (2021-6-22), immediately after AMI (2021-6-30) and before discharge from hospital (2021-7-7).
Lead author biography
Jin Xian, Ph.D., is an Associate Chief Physician of Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine. He is an associate director of the Structural Cardiology Group of Shanghai Cardiovascular Association. He specializes in the diagnosis and treatment of heart diseases, especially in intervention of CAD, transcatheter treatment of VHD. He participated in the compiling and writing of “The Progress of Cardiology”, “Panvascular Medicine - Concepts and Clinical Practice” and other literature. He has hosted 1 general projects of the National Natural Science Foundation of China, and published over 10 SCI articles.

References
- de la Puente P, Azab AK. Delivery systems for brachytherapy. J Control Release 2014; 192: 19-28.
- Zhang F, Wang J, Guo J, Huang X, Guan Z, Lei G, et al. Chinese expert consensus workshop report: Guideline for permanent iodine-125 seeds implantation of primary and metastatic lung tumors (2020 edition). J Cancer Res Ther. 2020; 16: 1549-1554.
- Liu Q, Dai X, Zhou X, Ye F, Zhou Y. Comparison of TACE combined with and without iodine-125 seeds implantation therapy for advanced stage hepatocellular carcinoma: a systematic review and meta-analysis. J BUON. 2019; 24: 642-649.
- Yan L, Chen L, Qian K, Kan X, Zhang H, Liang B, et al. Caudate Lobe Hepatocellular Carcinoma Treated with Sequential Transarterial Chemoembolization and Iodine 125 Seeds Implantation: A Single-Center Retrospective Study. Cancer Manag Res 2021; 13: 3901-3912.
- Lin J, Yang W, Jiang N, Zheng Q, Huang J, Huang N, et al. Incidence and prediction of seed migration to the chest after iodine-125 brachytherapy for hepatocellular carcinoma. Brachytherapy 2017; 16: 1252-1256.
- Sachdeva S, Udechukwu NS, Elbelasi H, Landwehr KP, Clair WH, Winkler MA. Prostate brachytherapy seed migration to the heart seen on cardiovascular computed tomographic angiography. Radiol Case Rep. 2017; 12: 31-33.
- Zhu AX, Wallner KE, Frivold GP, Ferry D, Jutzy KR, Foster GP. Prostate brachytherapy seed migration to the right coronary artery associated with an acute myocardial infarction. Brachytherapy. 2006; 5: 262-265.
- Li ZY, Gao HB, Zhang WH, Zhang XF, Han LG, Cui HP. Preparation of (125)I brachytherapy seeds by iodinating carbon bars with a silver coating. Appl Radiat Isot. 2021; 167: 109426.
- Mayer C, Kumar A. Brachytherapy. In. StatPearls. Treasure Island (FL); 2021.
- Li D, Jia YM, Cao PK, Wang W, Liu B, Li YL. Combined effect of (125)I and gemcitabine on PANC-1 cells: Cellular apoptosis and cell cycle arrest. J Cancer Res Ther. 2018; 14: 1476-1481.
- He Y, Li L, Liu J, Zhang X. Iodine-125 seed brachytherapy inhibits non-small cell lung cancer by suppressing epithelial-mesenchymal transition. Brachytherapy. 2018; 17: 696-701.
- Jia SN, Wen FX, Gong TT, Li X, Wang HJ, Sun YM, et al. A review on the efficacy and safety of iodine-125 seed implantation in unresectable pancreatic cancers. Int J Radiat Biol. 2020; 96:383-389.
- Calvert AD, Dyer AW, Montgomery VA. Embolization of prostatic brachytherapy seeds to pulmonary arteries: a case study. Radiol Case Rep. 2017; 12: 34-38.
- Wu W, Xue J, Liang P, Cheng Z, Zhang M, Mu m, et al. The assistant function of three-dimensional information for I125 particle implantation. IEEE J Biomed Health Inform. 2014; 18: 77-82.
- Chen E, Zhang Y, Zhang H, Jia C, Liang Y, Wang J. Dosimetry study of three-dimensional print template for 125I implantation therapy. Radiat Oncol. 2021; 16: 115.