
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Prolonged hyponatremia due to syndrome of inappropriate secretion of antidiuretic hormone in a preterm infant
Vinay Kalvacherla, MD31,2; Imran N Mir, MD3; Jyothsna Gattineni, MD4; Luc P Brion, MD3*
1University of Texas Southwestern Medical School, Dallas, TX, USA.
2Department of Pediatrics, University of Utah Health, USA.
3Department of Pediatrics, Division of Neonatal-Perinatal Medicine, University of Texas Southwestern Medical Center, Dallas, TX, USA.
4Department of Pediatrics, Division of Pediatric Nephrology, University of Texas Southwestern Medical Center, USA.
*Corresponding Author : Luc P Brion, MD
Professor Emeritus, Department of Pediatrics,
University of Texas Southwestern Medical Center,
5323 Harry Hines Boulevard, Dallas, TX, 75390-9063, USA.
Phone: 214-548-3903, Fax: 214-648-2481;
Email: Luc.Brion@utsouthwestern.edu
Received : Jul 21, 2023
Accepted : Aug 07, 2023
Published : Aug 14, 2023
Archived : www.jcimcr.org
Copyright : © Brion LP (2023).
Abstract
Hyponatremia, defined as a serum sodium concentration < 135 mmol/L, is associated with significant morbidity and mortality. Hyponatremia occurs in one third of preterm infants in the first week of life. The patient was a preterm infant born to a G2P0A1 mother at 25 weeks of gestation. The pregnancy was complicated by chlamydia infection and E-coli bacteriuria (both treated), as well as severe pre-eclampsia, for which labor was induced. The infant was born via vaginal delivery, with Apgar scores of 5 and 8 at 1 and 5 minutes, respectively. He received continuous positive airway pressure in the delivery room and was admitted to the neonatal intensive care unit. By Day Of Life (DOL) 3, E.coli bacteremia was noted and treated by antibiotics for 15 days and was complicated by hypotension, which responded to dopamine. Head Ultrasound (HUS) on DOL 7 demonstrated a bilateral periventricular hemorrhagic infarction (Bassan score 2). Hyponatremia developed at DOL 25. Hyponatremia was attributed to syndrome of inappropriate Secretion of Antidiuretic Hormone (SIADH) and was treated by fluid restriction. On DOL 28 he presented with E. Coli meningitis, which was treated with a 21-day course of antibiotics. Hyponatremia persisted along with notable natriuresis (urine Na 176-213 mmol/L). Hypertonic saline was provided for 16 days. Hyponatremia and high natriuresis eventually resolved after progressive decrease in sodium intake and continued fluid restriction. In summary, this patient presented with an unusually prolonged SIADH associated with intraventricular hemorrhage and meningitis.
Keywords: SIADH; Hyponatremia; Preterm; Meningitis; Intraventricular hemorrhage.
Abbreviations: BUN: Blood Urea Nitrogen; CSW: Cerebral Salt Wasting Syndrome; DOL: Day of Life; FE: Fractional Excretion; GPA: Gravida _Para _Aborta; HUS: Head Ultrasonogram; PMA: Postmenstrual Age; SIADH: Syndrome of Inappropriate Secretion of Antidiuretic Hormone.
Citation: Kalvacherla V, Mir IN, Gattineni J, Brion LP. Prolonged hyponatremia due to syndrome of inappropriate secretion of antidiuretic hormone in a preterm infant. J Clin Images Med Case Rep. 2023; 4(8): 2541.
Introduction
Hyponatremia, defined as a serum sodium concentration <135 mmol/L, is associated with significant morbidity and mortality [1]. Hyponatremia occurs in one third of preterm infants in the first week of life [2,3].
Case presentation
The patient was a preterm appropriate for gestational age infant born to a G2P0A1 mother at 25 weeks of gestation with a birthweight of 780 grams. The pregnancy was complicated by chlamydia infection and E-coli bacteriuria (both treated), as well as severe pre-eclampsia, for which labor was induced. The infant was born via vaginal delivery, with Apgar scores of 5 and 8 at 1 and 5 minutes, respectively. He received continuous positive airway pressure in the delivery room and was admitted to the neonatal intensive care unit.
He received surfactant, caffeine, a sepsis workup, ampicillin and gentamicin, and parenteral nutrition. By Day Of Life (DOL) 3, E. coli bacteremia was noted and treated by antibiotics for 15 days (meropenem followed by cefepime) and a short course of dopamine for hypotension. Head Ultrasonogram (HUS) on DOL 7 demonstrated a bilateral periventricular hemorrhagic infarction (Bassan score 2) [4].
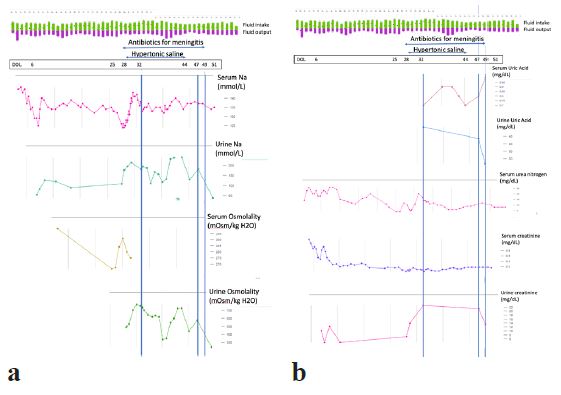
Hyponatremia (Na 126-133 mmol/L) developed at DOL 25 (Figure 1). Hyponatremia was attributed to syndrome of Inappropriate Secretion Of Antidiuretic Hormone (SIADH) due to high urine osmolality (490 mmol/kg H2O), low serum osmolality (266 mOsm/kg H2O) and normal urine output (3-4 ml/kg/hour) in the absence of high Blood Urea Nitrogen (BUN) or Acute Kidney Injury (AKI). Hyponatremia was treated by fluid restriction. High urine Na concentration (150 mmol/L) was attributed to hypervolemia secondary to SIADH. Laboratory data did not suggest adrenal insufficiency and ruled out hypothyroidism.
On DOL 28 he presented with hypotension, mottling and clinical seizures, due to E. Coli meningitis, which was treated with a 21-day course of antibiotics (meropenem followed by cefepime), fluid boluses and a short course of dopamine. Hypertonic saline was started on DOL 29 with a total Na intake of 15 mmol/kg/day while limiting fluid intake for SIADH. The differential diagnosis included SIADH treated with high Na intake from hypertonic saline versus Cerebral Salt Wasting Syndrome (CSW); both are associated with concentrated urine, high urinary Na concentration and high Fractional Excretion (FE) of urate (FEUrate) [5-8]. On DOL 32 [Postmenstrual Age (PMA), i.e., gestational age plus postnatal age, 30 weeks] urine osmolality was 735 mOsm/kg H2O) and FEU rate was 80% (normal up to 75% at 29-32 weeks PMA [9,10]. The presumed diagnosis was SIADH and the plan was to maintain fluid restriction and to reduce Na intake progressively. On DOL 44 serum Na concentration normalized. On DOL 45 hypertonic saline was stopped and Na intake reduced to 10 mmol/kg/day. On DOL 47 (PMA 32 weeks) urine osmolality remained high at 590 mOsm/kg H2O, FEU rate was normal at 72% with a Na intake of 8.7 mmol/kg/day. On DOL 49 FEUrate remained at 72% with a Na intake of 6.7 mmol/kg/day. On DOL 51 urine osmolality decreased to 242 mOsm/kg H2O) and serum Na concentration remained normal with a Na intake of 5 mmol/kg/day.
The patient developed food protein-induced enterocolitis treated with elemental diet. He later developed retinopathy of prematurity requiring laser surgery, and posthemorrhagic hydrocephalus, for which he received a ventricular reservoir and later a ventriculoperitoneal shunt. He was discharged home at 4 months of age.
Discussion
Hyponatremia in preterm infants most often results from either fluid overload, negative sodium balance due to insufficient intake to compensate sodium loss via immature kidneys or both [3]. SIADH, a dysregulation of ADH secretion by the posterior pituitary gland, is characterized by hyponatremia resulting from water retention due to increased water permeability in the renal collecting ducts. Increased natriuresis often occurs in SIADH because of volume expansion (typically with low BUN: Creatinine ratio) and contributes to hyponatremia. SIADH often occurs as a complication of cerebral injury via meningitis, neoplasia, or surgical/traumatic causes [5]. The main treatment for SIADH is fluid restriction. High natriuresis with SIADH is initially caused by SIADH-mediated hypervolemia and is treated with fluid restriction. Hypertonic saline is reserved for patients with severe symptomatic hyponatremia.
CSW or renal salt wasting syndrome is a much rarer process in children and infants [5-8]. CSW, a dysregulation of natriuresis, is characterized by volume depletion, hyponatremia, hypouricemia, inappropriately concentrated urine, high urine Na concentration and high FEUrate. Most common causes of CSW include cerebral injury and craniofacial surgery [5-8). The pathophysiologic mechanism for CSW is incompletely elucidated. Treatment for CSW is generally fluid and Na supplementation.
Differentiating criteria between SIADH and CSW in children and infants include volume status, which often is inaccurate and unreliable, and serial measurements of FEUrate [5-8,11-14]. Because SIADH and CSW have similar presentations, the existence of CSW has been questioned [13-14]. Diagnosis of CSW can only be made based on stringent criteria including lack of volume expansion and persistence of a high FEUrate for age after correcting hyponatremia and progressively stopping Na supple mentation. Measuring FEUrate has limited usefulness in very preterm infants until reaching term corrected age because of lack of normal values at < 28 weeks gestational age and high [50 ± 21% (mean ± standard deviation)] values up to 36 weeks PMA in preterm infants born at 28-34 weeks’ gestation [9,10]. Mean values of FE Urate decrease progressively from 70% at 29-32 weeks to 39 ± 14% at 38-40 weeks PMA [9].
Duration of SIADH-related hyponatremia (19 days) and high urine osmolality (22 days) in this patient was much longer than SIADH in published case series of children with acute non-tuberculous bacterial (n=28) or enteroviral (n=9) meningitis, which resolves, respectively, within 10 days or 1.7 ± 1.9 days [15,16].
Declarations
In summary, this patient presented with an unusually prolonged case of SIADH associated with intraventricular hemorrhage and meningitis. Hyponatremia resulted from two mechanisms associated with SIADH: Dilution and hypernatriuresis. The persistence of high natriuresis was likely due to high Na intake, which was reduced progressively. Eventually fluid and electrolyte disturbances resolved with fluid restriction and progressive reduction of Na intake.
Funding source: None
Conflict of interest: None
Financial disclosure: None
References
- Bernal A, Zafra MA, Simón MJ and, Mahía J. Sodium Homeostasis, a Balance Necessary for Life. Nutrients. 2023; 15: 395.
- Yee AH, Burns JD and, Wijdicks EF. Cerebral salt wasting:: pPathophysiology, diagnosis, and treatment. Neurosurg Clin N Am. 2010; 21: 339-352.
- Van der Lee D, de Bruin C, Steggerda SJ and , Vlaardingerbroek H. Idiopathic SIADH in the premature newborn, a case report. J Neonatal Perinatal Med. 2020; 13: 283-285.
- Bassan H, Benson CB, Limperopoulos C, Feldman HA, Ringer SA, Veracruz E, et al. Ultrasonographic features and severity scoring of periventricular hemorrhagic infarction in relation to risk factors and outcome. Pediatrics. 2006; 117: 2111-2118.
- Oh JY and, Shin JI. Syndrome of inappropriate antidiuretic hormone secretion and cerebral/renal salt wasting syndrome:: similarities and differences. Front Pediatr. 2015; 2: 146.
- Assadi F and, Mazaheri M. Differentiating syndrome of inappropriate ADH, reset osmostat, cerebral/renal salt wasting using fractional urate excretion. J Pediatr Endocrinol Metab. 2020; 34: 137-140.
- Bardanzellu F, Marcialis MA, Frassetto R, Melis A and, Fanos V. Differential diagnosis between syndrome of inappropriate antidiuretic hormone secretion and cerebral/renal salt wasting syndrome in children over 1 year: proposal for a simple algorithm. Pediatr Nephrol. 2022; 37: 1469-1478.
- Bettinelli A, Longoni L, Tammaro F, Faré PB and, Garzoni L, Bianchetti MGet al. Renal salt-wasting syndrome in children with intracranial disorders. Pediatr Nephrol. 2012; 27: 733-739.
- Stapleton FB. Renal uric acid clearance in human neonates. J Pediatr. 1983; 103: 290-294.
- Giapros V, Papadimitriou P, Challa A and, Andronikou S. The effect of intrauterine growth retardation on renal function in the first two months of life. Nephrol Dial Transplant. 2007; 22: 96-103.
- Chung HM, Kluge R, Schrier RW and , Anderson RJ. Clinical assessment of extracellular fluid volume in hyponatremia. Am J Med. 1987; 83: 905-908.
- Palmer BF and, Clegg DJ. Cerebral Salt Wasting Is a Real Cause of Hyponatremia:: COMMENTARY. Kidney Intern. 2023; 4: e445-e447.
- Sterns RH and, Rondon-Berrios H. Cerebral Salt Wasting Is a Real Cause of Hyponatremia:: CON. Kidney Intern. 2023; 4: e441-e444.
- Maesaka JK and, Imbriano LJ. Cerebral Salt Wasting Is a Real Cause of Hyponatremia:: PRO. Kidney Intern. 2023; 4: e437-e440.
- Patwari AK, Singh BS and , Manorama DE. Inappropriate secretion of antidiuretic hormone in acute bacterial meningitis. Ann Trop Paediatr. 1995; 15: 179-183.
- Chemtob S, Reece ER and, Mills EL. Syndrome of inappropriate secretion of antidiuretic hormone in enteroviral meningitis. Am J Dis Child. 1985; 139: 292-194.