
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Self-limiting pernio-like ‘Covid-Toe’ reaction following oxford-astrazeneca vaccination in a renal transplant patient
Sebastian Spencer1,2,3*; Sunil Bhandari2,3
1University of Hull, England.
2Hull York Medical School, England.
3Hull University Teaching Hospitals NHS Trust, England.
*Corresponding Author : Sebastian Spencer
Hull University Teaching Hospitals NHS Trust, England.
Email: sebastian.spencer2@nhs.net
Received : Jul 21, 2023
Accepted : Aug 07, 2023
Published : Aug 14, 2023
Archived : www.jcimcr.org
Copyright : © Spencer S (2023).
Abstract
We present a case of self-limiting pernio-like ‘Covid-Toe’ reaction in a 40-year-old female with a history of kidney/pancreas transplant who received the Oxford-AstraZeneca Covid-19 mRNA vaccine. The patient experienced bilateral digital skin inflammation, erythematous papules, blistering, and ulceration in the proximal interphalangeal joints, which spontaneously resolved. Extensive investigations ruled out other causes, and subsequent doses of the vaccine and an episode of SARS-Cov-2 infection did not trigger a similar reaction. The underlying mechanism of Covid-Toe remains uncertain, but it may involve immune activation by the virus or vaccine.
Citation: Spencer S, Bhandari S. Self-limiting pernio-like ‘Covid-Toe’ reaction following oxford-astrazeneca vaccination in a renal transplant patient. J Clin Images Med Case Rep. 2023; 4(8): 2542.
Description
A 40-year-old female kidney-pancreas transplant patient presented with painful swelling of PIP joints and circular ulcerated skin lesions (Figures 1 and 2) in March 2021. The patient demonstrated reduced grip strength, and range of movement of the right shoulder.
She has a past medical history of hypothyroidism, type-1 diabetes and diabetic nephropathy with simultaneous kidney-pancreas transplant on Christmas Day 2020. She was maintained on Mycophenolate Mofetil and Tacrolimus and received her first Coronavirus vaccination, with AZD1222, five weeks prior.
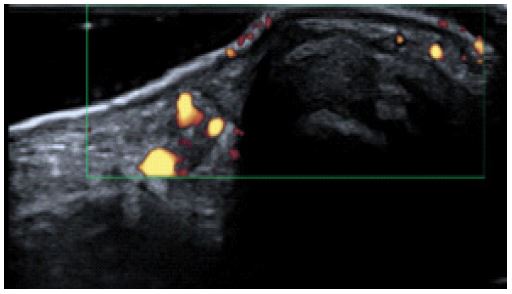
X-ray and ultrasound imaging demonstrated swelling of radial aspects of the wrists, but no evidence of inflammatory arthritis, joint effusions, or bone abnormalities (Figure 3 and 4). Swabs and skin scrapings detected no bacterial, viral or fungal infections. Blood tests, including anti-CCP, ANCA, complement, immunoglobulins, rheumatoid factor, autoantibodies and HLA-B27, were negative. CRP was less than 2 mg/L.
No autoimmune, infective or vascular cause for the observed pernio-like reaction was identified and so we hypothesize that the reaction is a consequence of exposure to AZD1222. The lesions gradually improved and spontaneously resolved in 4 months without any specific intervention. Interestingly, our patient did not experience a recurrence of the reaction with a subsequent booster dose of AZD1222, nor with the Moderna mRNA-1273 booster.
She also experienced an episode of acute symptomatic SARS-Cov-2 infection in January 2022 which did not produce any dermatological manifestations.
A diagnosis of self-limiting pernio-like ‘Covid Toe’ reaction was made with spontaneous resolution four months later. The underlying mechanism of this reaction remains uncertain and requires further investigation to better understand its pathophysiology.


Acknowledgements
The authors would like to thank Dr Maneesha Weerasooriya for her contribution and collaboration in producing this case report.
References
- Cavazos A, Deb A, Sharma U, Nugent K. COVID toes following vaccination. Proc (Bayl Univ Med Cent). 2022; 35(4): 476-479. doi: 10.1080/08998280.2022.2043732
- Freeman EE, McMahon DE, Lipoff JB, Rosenbach M, Kovarik C, Desai SR, Harp J, Takeshita J, French LE, Lim HW, Thiers BH, Hruza GJ, Fox LP. The spectrum of COVID-19-associated dermatologic manifestations: An international registry of 716 patients from 31 countries. J Am Acad Dermatol. 2020; 83(4): 1118-1129. doi: 10.1016/j.jaad.2020.06.1016
- Marzano AV, Cassano N, Genovese G, Moltrasio C, Vena GA. Cutaneous manifestations in patients with COVID-19: a preliminary review of an emerging issue. Br J Dermatol. 2020; 183: 431-442.
- Magro CM, Mulvey JJ, Laurence J, et al. The differing pathophysiologies that underlie COVID-19-associated perniosis and thrombotic retiform purpura: a case series. Br J Dermatol. 2021; 184(1): 141-150. doi:10.1111/bjd.19415
- Magro C, Crowson AN, Franks L, Schaffer PR, Whelan P, Nuovo G. The histologic and molecular correlates of COVID-19 vaccine-induced changes in the skin. Clin Dermatol. 2021; 39(6): 966-984. doi:10.1016/j.clindermatol.2021.07.011
- Aschoff R, Zimmermann N, Beissert S, Günther C. Type I Interferon Signature in Chilblain-Like Lesions Associated with the COVID-19 Pandemic. Dermatopathology (Basel). 2020; 7(3): 57-63. doi: 10.3390/dermatopathology7030010
- Souaid K, Oulès B, Sohier P, Deschamps L, Aractingi S, Dupin N. Type I Interferon Signature in Chilblains Following SARS-CoV-2 mRNA Vaccine: A Case Report. Acta Derm Venereol. 2021; 101(11): adv00589. doi: 10.2340/00015555-3888