Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Atypical lipid keratopathy
Kammoun Sonda; Rekik Mona*; Gargouri Salma; Trigui Amira
Department of Ophthalmology, Habib Bourguiba Hospital, Sfax, Tunisia.
*Corresponding Author : Rekik Mona
Department of Ophthalmology, Habib Bourguiba Hospital, Sfax, Tunisia.
Tel: +00-216-24300099;
Email: rekikmona@yahoo.fr
Received : Jul 18, 2023
Accepted : Aug 08, 2023
Published : Aug 15, 2023
Archived : www.jcimcr.org
Copyright : © Mona R (2023).
Abstract
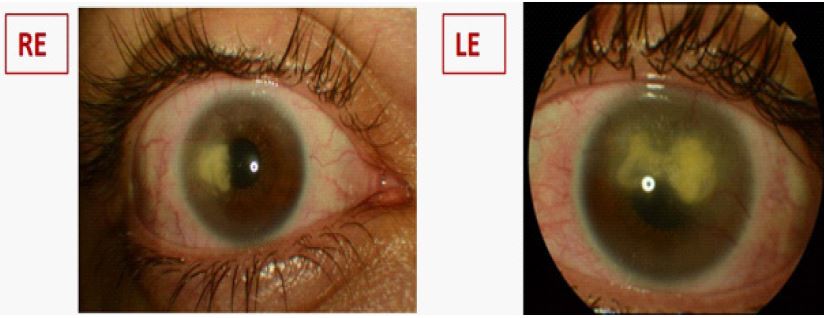
A 26-year-old patient, presented with a bilateral corneal clouding that had been slowly progressive over the last 2 years. He was a sports trainer having consumed protein for bodybuilding. Visual acuity was 6/10 in the Right Eye (RE) and 1/20 in the Left Eye (LE).
Citation: Sonda K, Mona R, Salma G, Amira T. Atypical lipid keratopathy. J Clin Images Med Case Rep. 2023; 4(8): 2543.
Clinical image description
Slit lamp examination showed deep yellow corneal deposits with stromal neovascularization (Figure 1). No other ocular abnormalities were found. The anterior segment optical coherence tomography revealed a hyper-reflective area in the deep stroma (Figure 2). Confocal microscopy showed hyper-reflective structures in deep stroma (Figure 3). Evidence of hyperlipidemia was not apparent. No evidence was found for a systemic or an infectious disease. The patient was diagnosed with lipid keratopathy secondary to anabolics. This case describes a very rare condition and represents the first case of lipid keratopathy secondary to anabolics in a sports trainer. To the best of our knowledge, this is the first report of corneal neovascularization in a patient using anabolics reported to date.
Lipid keratopathy is a rare disease. It has a primary and a secondary form, the secondary being the more common entity because of leakage from lipids out of newly formed corneal vessels after inflammation. Oxidative stress and physical exercise increase surface inflammation and limbitis and promote corneal neovascularization which leads lipid keratopathy.
Declarations of interest: None.