
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Fusarium fungemia in a term neonate with renal cysts
Adeyinka A Davies1,2*; Chioma S Osuagwu1,3; Rebecca Folake Peters1; Olajumoke Makinwa1; Rita O Oladele1,3
1Department of Medical Microbiology and Parasitology, Lagos University Teaching Hospital, Idi-Araba, Lagos-State, Nigeria.
2Department of Medical Microbiology and Parasitology, Olabisi Onabanjo University Teaching Hospital, Sagamu, Ogun-State, Nigeria.
3Department of Medical Microbiology and Parasitology, University of Lagos, Akoka, Lagos, Nigeria.
*Corresponding Author : Adeyinka A Davies
Department of Medical Microbiology and Parasitology, Lagos University Teaching Hospital, Idi-Araba, Lagos-State, Nigeria.
Email: dynkodunsi1@gmail.com
Received : Jul 20, 2023
Accepted : Aug 09, 2023
Published : Aug 16, 2023
Archived : www.jcimcr.org
Copyright : © Davies AA (2023).
Abstract
Fusarium species are emerging opportunistic pathogens responsible for life-threatening infection, especially in immunocompromised hosts. In this report, we present the case of invasive fusariosis in a term male neonate diagnosed with early-onset neonatal sepsis and post-renal Acute Kidney Injury (AKI). His fever was continuous and unresponsive to systemic antibiotics, in addition, the AKI was secondary to bilateral hydronephrosis with anuria that persisted despite kidney challenge. However patient demise occurred before a diagnosis of invasive fungal (Fusarium species) infection was made from his blood culture. This case further confirms that invasive Fungal Infection (IFI) should be entertained in persistent fever with accompanying neutropenia. And starting empirical antifungals in advance before the results of investigations are available is beneficial to patients. Thus, a heightened suspicion index is needed to reduce the mortality associated with IFI.
Keywords: Fusarium species; Invasive fusariosis; Invasive fungal infection; Acute kidney injury; Hydronephrosis.
Citation: Davies AA, Osuagwu CS, Rebecca FP, Makinwa O, Oladele RO. Fusarium fungemia in a term neonate with renal cysts. J Clin Images Med Case Rep. 2023; 4(8): 2546.
Introduction
Fusarium is an emerging pathogen endemic to tropical and subtropical countries [1]. It is an opportunistic pathogen that causes life-threatening infections in the immunocompromised [2-6]. It’s a filamentous mould whose spores exist in plant debris, soil, and water, and are reported to be associated with plant, human, and animal infections [1,2]. Human infections arise by inhalation, ingestion, direct inoculation, or through contaminated medical equipment with Fusarium spores in skin or mucous membrane [2,3]. Infection includes keratitis, endophthalmitis, onychomycosis, arthritis, fungemia, peritonitis, sino-pulmonary infections; and skin and soft tissue infection [2,3].
The literature search only revealed several case reports of invasive fusariosis in immunocompromised children with haematological malignancies [2-7]. More than 50 Fusarium species exist in nature, only 12 reportedly caused human infections, with F. solani (50%) being the most prevalent species. Fusarium species produce many virulence factors, such as trichothecenes that impair humoral and cellular immunity and cause tissue breakdown [2]. Aleuroconidia, collagenases, and proteases enzymes favour the invasion of the bloodstream resulting in thrombosis, tissue infarction and persistence of infection respectively [2].
We hereby present a case report of a full-term neonate with Fusarium species bloodstream infection from a Nigerian tertiary hospital. This may be the first case report from Nigeria as literature search did not reveal other cases of neonatal fusarium fungaemia in Nigeria.
Case presentation
A term male neonate was referred to Lagos University Teaching Hospital on 23rd April 2022 from a peripheral hospital on account of irritability, refusal of breast milk and inability to pass urine from birth. The accompanied full blood count results showed Packed Cell Volume (PCV) of 30%, White Blood Cell (WBC) of 28,500/mm3, Neutrophil (N) of 29%, Lymphocytes (L) of 53%, and an elevated C-reactive protein. He is a product of spontaneous vertex delivery, with a birth weight of 3.3 kilograms and an Apgar score of 8 at 1 minute. There was no history of fever, vomiting, or loss of consciousness, but the prenatal anomaly scan at 26 weeks gestation revealed a right renal cyst, with a normal-sized left kidney. Physical examination revealed an acutely ill-looking neonate on intranasal oxygen, via nasal prongs (from referral hospital). He was afebrile (temperature-37oC), pale, and in obvious respiratory distress.
Central nervous system examination showed a conscious neonate with a flat, normotensive anterior fontanelle. The neck was supple with global normotonia. Cardiovascular examination revealed a low-volume pulse, with a heart rate of 146 beats per minute. S1 and S11 heart sounds were heard. The chest examination revealed a respiratory rate of 66 cycles per minute, with a percentage oxygen saturation of 92-93%. The abdomen was full, with a liver size of 4 cm below the right costal margin, and the spleen and kidney were not palpably enlarged. Anus was patent with normal male external genitalia, both testicles were palpable. No cleft lip or palate, spinal dysraphism, or limb abnormalities.
A diagnosis of early-onset neonatal sepsis and post-renal acute kidney injury with Kidney Disease Improving Global Outcome (KDIGO) stage 3 was made. He was admitted to the neonatal intensive care unit (NICU). Commenced on intranasal oxygen via Continuous Positive Airway Pressure (CPAP) at 5 L/minute, nil per oral, with close monitoring of vital signs and urinary output, and intravenous Levofloxacin 34 mg (10 mg/ kg/ dose 12 hourly). The kidney was challenged with 20 ml/kg 0.9% normal saline (66 ml) over one hour, with maintenance Intravenous Fluid (IVF) of 50 ml/kg/day. The patient remains anuric and the Full Blood Count (FBC) Showed Anaemia (PCV 37.2%), leucocytosis with neutropenia (WBC, 35,000/mm3, N 22%) and thrombocytopenia (platelet count 70,000/mm3). Serum electrolytes revealed mild hyperkalemia with metabolic alkalosis (sodium 138 mmol/ l, potassium 5.5 mmol/ l, chloride 99 mmol/ l, bicarbonate 16 mmol/ l, blood urea nitrogen of 13.5 mmol/ l, Creatinine of 283.4 μmol/ l). The total protein was 52 g/ dl (67-82 g/l) with albumin 32 g/l (32-55 g/l). The deranged electrolyte was corrected, the blood level was optimized with packed cell and platelet transfusion in aliquot, and parenteral vitamin K was given daily.
On day 2, he became febrile and had intermittent episodes of hypoglycaemia (random plasma glucose ranged, from 45 to 59 mg/dl), which was corrected. Renal Ultrasound Scan (KUB USS) revealed Grade 2 bilateral hydronephrosis with a prominence of both pelvicalyceal systems and a poorly delineated ureter beyond the pelvi-uretero junction. Chest X-ray revealed cardiomegaly with multichambered Configuration (CTR was 62%) and clear lung field bilaterally. On day 3, he started bleeding from the mouth with associated hematemesis and haema haematochezia. Despite all measures to stabilise the patient he died at 11:30 PM.
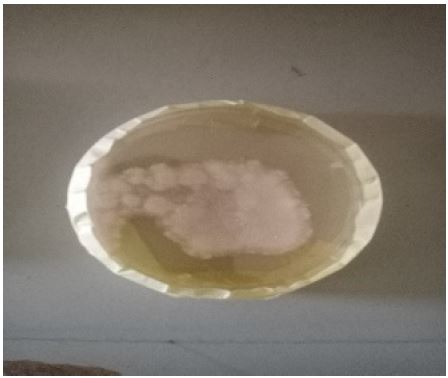
The blood culture collected on admission and incubated in the Bactec Blood culture system (BD diagnostics) flagged positively on the 3rd day of incubation. The Gram showed septate hyphae with acute angle branching. Sample was sub-cultured into Saboraud Dextrose Agar (SDA) which yielded white, cotton fluffy colonies. The microscopic examination with Lactophenol Cotton Blue (LPCB) revealed typical banana-shaped macroconidia that were identified as Fusarium species. Unfortunately, the patient had died at this time.

Discussion
Fusarium species is one of the most clinically significant moulds in the immunocompromised and is typically present in soil, water, and organic substrates [8]. Skin, mucous membranes, and airways serve as the primary entry points. In this case, we are not sure of the source of this infection, but access through the umbilical stump could be a possible entry site. In the first week of postnatal life, the innate immune cells are the sole source of immune defence responder, changes in this immune response promote early-onset sepsis [9]. Neutrophils and macrophages inhibit hyphal growth and spore germination, with neutrophils being the primary responder in infection [8,10]. In this case report, a clinical infection was evidenced by leucocytosis, fever and a positive blood culture. Empiric antibiotics are usually given to patients with clinical features of infection while awaiting the result of blood culture. Fungal infections do not respond to antibiotics, hence the treatment failure. Though there are serological markers of invasive fungal infections to aid in early diagnosis of fungal infections, they have their pitfalls and may have to be used in combination [11,12]. More so these tests are not routinely available in our facility and may not be affordable by the patient. The renal comorbidity in this patient could have contributed to the negative outcome of this case. This patient was anuric till death and the accumulation of waste may have hastened the demise.
Fusarium fungaemia usually responds to antifungal therapy. The case of Fusarium mycetoma in a preterm infant with posterior urethral valve abnormalities was reported from Israel, and the neonate fully recovered with surgical drainage and medical therapy [13]. Likewise, Ramos et al reported a case from Brazil involving an 11-year-old boy with Acute Lymphocytic Leukaemia (ALL) who made a full recovery with the timely institution of antifungal treatment [6]. Several case series involving those with haematological and non-haematological malignancies have been reported [5,7,14]. In this case, death occurred before diagnosis, so antifungal treatment was not initiated.
Conclusion
This case further confirms that Invasive Fungal Infection (IFI) should be entertained in persistent fever with accompanying neutropenia. And starting empirical antifungals in advance before the results of investigations are available is beneficial to patients. Thus, a heightened suspicion index is needed to reduce the mortality associated with IFI.
Declarations
Author contributions: R.F.P: did the laboratory work and wrote the introduction. A.A.D: was involved in the conceptualisation of the case report, literature review and wrote the draft manuscript. O.M: was involved in the laboratory work. C.S.O and R.O.O: were involved in the literature review and manuscript writing. All the authors reviewed and accepted the final version of the manuscript.
Funding: None.
Conflicts of interest: The authors declare no conflict of interest.
Acknowledgements: All staff of Medical Microbiology and Parasitology and the paediatricians in LUTH.
References
- Ruiz-Beguerie J, Barbini C, Busso C, Anaya J. Invasive Fusariosis: Case Series and Review of the Fusarium Infection. Indian J Dermatol Res. 2019; 1: 102.
- Nucci M, Barreiros G, Akiti T, Anaissie E, Nouér SA. Invasive Fusariosis in Patients with Hematologic Diseases. J. Fungi. 2021; 7, 815.
- Velasco E, Martins CA, Nucci M. Successful treatment of catheter-related Fusarial infection in immunocompromised children. Eur. J. Clin. Microbiol. Infect. Dis. 1995; 14.
- Nadia Litvinov, Mariama Tomaz N da Silva, Inneke M van der Heijden, Mariana G Graça, Larissa Marques de Oliveira, et al. An outbreak of invasive fusariosis in a children’s cancer hospital. Clin Microbiol Infect 2015; 21: 268.e1-268.e7
- Benish M, Elitzur S, Arad-Cohen N, Barg AA, Ben-Harosh M, et al. Invasive Fusariosis in Pediatric Hematology/Oncology and Stem Cell Transplant Patients: A Report from the Israeli Society of Pediatric Hematology-Oncology. J. Fungi. 2022; 8: 387
- Regina Teixeira Barbieri Ramos, Luciana da Silva Ruiz, Diniz Pereira Leite Júnior, Mariana Volpe Arnoni, Marcelo Otsuka, et al. Invasive infection by Fusarium verticillioides in a pediatric leukaemia patient and literature review on a series of fusariosis. Europ. Acad. Res. 2022; 9: 12
- Carlesse F, Amaral AC, Goncalves SS, Xafranski H, Lee MM, et al. Outbreak of Fusarium oxysporum infections in children with cancer: An experience with 7 episodes of catheter-related fungemia. Antimicrob Resist Infect Control. 2017; 6: 93.
- Alireza Rajabzadeh, Dariush Shokri, Shima Aboutalebian, Hamid Morovati, Abdolrasoul Mohammadi, et al. A Fatal Case of Bloodstream Infection by Fusarium Solani in a Patient with Adrenocortical Carcinoma From Isfahan, Iran. Int J Cancer Manag. 2020; 13: e98610.
- Francesca Cortese, Pietro Scicchitano, Michele Gesualdo, Antonella Filaninno, Elsa De Giorgi, et al. Early and Late Infections in Newborns: Where Do We Stand? A Review, Pediatrics & Neonatology, 2016; 57: 265-73.
- Kernien JF, Snarr BD, Sheppard DC, Nett JE. The Interface between Fungal Biofilms and Innate Immunity. Front Immunol. 2018; 8: 1968.
- Lass-Florl C, Alastruey-Izquierdo A, Gupta R, Chakroborti A. Interpretation, pitfalls of biomarkers in diagnosis of invasive fungal diseases. Indian Journal of Medical Microbiology. 2022; 40: 480-484.
- Ostrosky-Zeichner L, Vitale RG, Nucci M. New serological markers in medical mycology: (1,3)-(-D-glucan and Aspergillus galactomannan. Infection. 2012; 16, 59-63.
- Nakar C, Livny G, Levy I, Samra Z, Linder N, et al. Mycetoma of the renal pelvis caused by Fusarium species. Pediatr Infect Dis J. 2001; 20: 1182-3.
- Ji-Yeon Kim, Cheol-In Kang, Ji Hye Lee, Woo Joo Lee, Kyungmin Huh, Sun Young Cho. Clinical Features and Outcomes of Invasive Fusariosis: A Case Series in a Single Center with Literature Review. Infect Chemother. 2021; 53: e4.