
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Fertility-preserving radical trachelectomy for early-stage cervical cancer in a young woman at Bugando Medical Centre in Mwanza, Tanzania: A case report
Fatma Mohd1; Gonzaga Ngonyani1; James Mboyerwa1; Oscar Ottoman2; Richard Kiritta1; Feredina John1;
Albert Kihunrwa1; Dismas Matovelo1; Edgar Ndaboine1*
1Department of Obstetrics and Gynecology, Bugando Medical Centre, Catholic University of Health and Allied Sciences, Mwanza, P.O. Box 1464, Mwanza, Tanzania.
2Department of Pathology, Bugando Medical Centre, Catholic University of Health and Allied Sciences, P.O. Box 1464, Mwanza, Tanzania.
*Corresponding Author : Edgar Ndaboine
Department of Obstetrics and Gynecology, Bugando Medical Centre, Catholic University of Health and Allied Sciences, Mwanza, P.O. Box 1464, Mwanza, Tanzania.
Email: ndaboine2@yahoo.com
Received : Jul 17, 2023
Accepted : Aug 11, 2023
Published : Aug 18, 2023
Archived : www.jcimcr.org
Copyright : © Ndaboine E (2023).
Abstract
Background: For women with early cervical cancer who wish to preserve their fertility, radical trachelectomy is the recommended procedure. More than 40% of all instances of cervical cancer occur in women of reproductive age, resulting in a major increase in the frequency of this surgery. Even though cervical cancer is common in places with few resources, this procedure is rarely mentioned.
Case presentation: Para 4 Living 1, a 36-year-old female, was examined and cared for at our facility for one year. Her major concerns were six years of infertility and repeated fetal loss due to recurrent preeclampsia. During her reproductive examination, she was also screened for cervical cancer, which found the disease’s early stages (IB1). Her biopsy confirmed grade 1 squamous cell carcinoma. To preserve her fertility, she had radical trachelectomy, bilateral pelvic lymph node dissection, and transabdominal placement of cervical cerclage. This is among rare reports of a radical trachelectomy as a fertility-preserving treatment for early cervical cancer in low-resource settings.
Conclusion: Radical trachelectomy with pelvic lymphadenectomy is an oncologically safe option for preserving fertility that may be considered in resource-limited areas, particularly for women with a strong desire to have babies.
Keywords: Radical trachelectomy; Cervical cancer; Fertility-sparing surgery; Resource-limited setup.
Citation: Mohd F, Ngonyani G, Mboyerwa J, Ottoman O, Ndaboine E, et al. Fertility-preserving radical trachelectomy for early-stage cervical cancer in a young woman at Bugando Medical Centre in Mwanza, Tanzania: A case report. J Clin Images Med Case Rep. 2023; 4(8): 2549.
Introduction
Cervical cancer is the second most commonly diagnosed cancer and the third cause of cancer death among women in less developed countries (sub-Saharan Africa, Latin America and the Caribbean, and Melanesia) with more than 40% of patients with early cervical cancer affected during reproductive age where there is a desire for future fertility [1]. In Tanzania, the burden of cervical cancer is higher where approximately every year 10,241 women are diagnosed and 6,525 die from the disease [2].
Case presentation
A 36-year-old para 4 living 1 lady was cared for at our facility for one year with the main complaints of infertility for the previous six years and recurrent fetal loss related to preeclampsia. She was evaluated for infertility in February 2022, and she was also examined for cervical cancer with a Pap smear test, pelvic ultrasound, and hormone tests. Despite having irregular menstrual cycles with skipping patterns, her hormonal workups were normal, as were her uterus and ovaries sonography findings. The Pap smear, on the other hand, indicated a high-grade squamous intraepithelial lesion (HSIL) associated with acute cervicitis. She was subsequently given antibiotics for cervicitis as well as LEEP for HSIL. Later her LEEP biopsy indicated invasive squamous cell carcinoma keratinizing grade 1 with micro invasion, yet she was missing for several months. She came in December 2022, complaining of postcoital bleeding and irregular vaginal discharge. A 2 cm hyperemic, enlarged cervical lesion was detected during a cervical reexamination.
Her obstetric history revealed that she became pregnant for the first time at the age of 18. Tragically, due to eclampsia, she lost the baby at 32 weeks. She became pregnant again at the age of 22, and due to severe preeclampsia, she had to give delivery at 29 weeks. Her baby died on the fourth day of life owing to preterm issues. Her third pregnancy occurred in 2013, at the age of 26, and her baby died intrauterine from severe preeclampsia at 27 weeks of gestation. She gave birth vaginally to a healthy live fetus in 2016 at the age of 29, and is still living today. Her medical history is unremarkable, she is HIV-negative and has no history of diabetes or chronic hypertension. She has not been able to conceive again after her last delivery, despite not taking contraception and remaining married to the same spouse.
Apart from the cervical lesion, her other examination findings, including laboratory and radiographic findings, as well as vital signs, were normal, her BIM was normal at 24 kg/m2. Because the patient desired conception, she underwent radical transabdominal trachelectomy, which included dissection of bilateral pelvic lymph nodes and insertion of a cerclage at the level of the cervical internal os (Figure 1 shows pictures of the removed cervix). An intra-cavitary Foley catheter was placed for 14 days to prevent stenosis. Her uterus, ovaries, and fallopian tubes appeared normal during surgery, and there were no pelvic adhesions. She had an uneventful recovery from surgery and is currently undergoing follow-up, during which she has remained cancer-free and resumed regular menstruation.
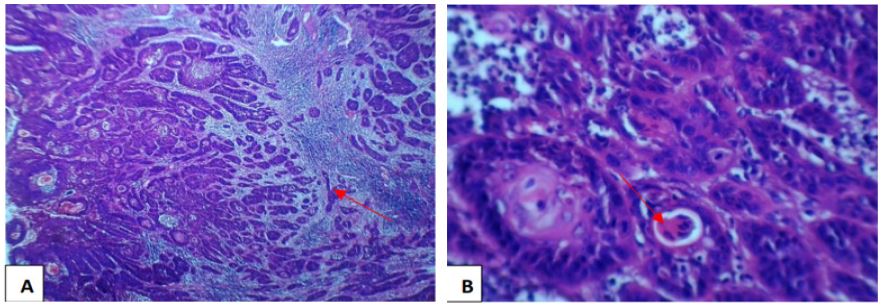
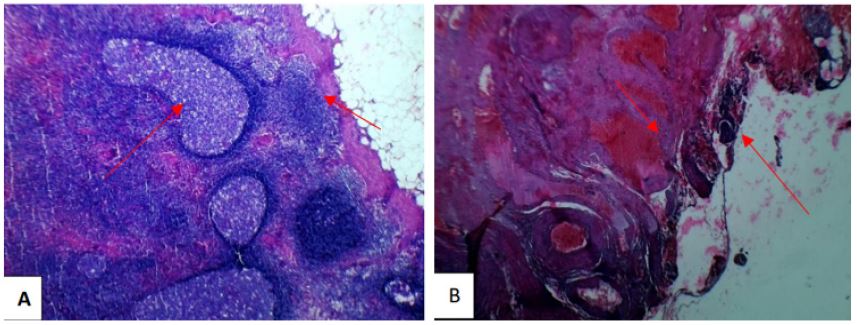
The final pathological report of radical trachelectomy revealed an invasive squamous cell carcinoma, keratinizing large cell type grade 1 with 2 cm in widest diameter, infiltration on the ectocervical stroma with no involvement of endocervical canal. Para-cervical resection margin and all pelvic lymph nodes resected were free from tumor. Also, the vaginal extension sample submitted was free from tumor cell invasion (Figures 2 and 3). This is a rare example of trachelectomy as a fertility-preserving treatment in early cervical cancer in a resource-constrained context.

Discussion
Childbearing is one of the most essential goals in life, and fertility preservation surgery has become an integral part of enhancing the quality of life for young cancer survivors. This component was disregarded in the past, but in recent decades it has garnered increased attention. Before cancer therapies, it is necessary for the physician to address the issue of fertility in patients of reproductive age [3].
Cervical cancer is the fourth most common cancer affecting women worldwide, after breast, colorectal, and lung cancers, accounting for nearly 570,000 new cases every year diagnosed and over 311,000 deaths reported annually [4]. But a wide variation of cervical cancer was observed in lower resource countries where the highest incidence rates were picked in Sub-Saharan Africa and with 85% of deaths occurring annually in developing regions. Inadequate screening and limited access to standard treatment options explain the large geographic variation in cervical cancer rates. Persistent infection with high-risk Human Papillomavirus (HPV) types is the major risk factor for cervical cancer. High parity, long-term use of oral contraceptive pills, tobacco consumption, co-infection with other sexually transmitted agents, lifestyle factors such as multiple sexual partners, younger age at first sexual intercourse, immunosuppression, and diet has been identified as the co-factors most likely to influence the risk of acquisition of HPV infection and its further progress to cervical carcinogenesis [5]. Our patient presents a unique case, as she possesses few of the recognized risk factors associated with the development of cervical cancer. However, two factors stand out: early sexual exposure and the absence of regular cervical cancer screening. It is worth noting that she experienced her first pregnancy at the age of 18, indicating early sexual activity. Additionally, the lack of regular screening for cervical cancer likely contributed to the situation. Fortunately, her diagnosis occurred at an early stage due to the opportunity she received during the infertility evaluation, highlighting the importance of such evaluations in detecting cervical cancer early.
These circumstances should serve as a valuable reminder to clinicians, particularly those operating in resource-limited areas where routine screening may be lacking. It is crucial for clinicians to conduct cervical tests for all women seeking gynecological care, even if they present with other unrelated concerns. By incorporating cervical cancer screening into their practice, clinicians can contribute to the early detection and prevention of this disease, ultimately improving patient outcomes and reducing the burden of cervical cancer in resource-limited settings.
For most women diagnosed with cancer of the cervix at the aged of 35-44, the radical trachelectomy is preserved for highly selected patients with early-stage disease. Although different fertility-sparing options can be selected in these women, among them simple cervical cone biopsy, and cone biopsy with pelvic lymph node assessment, radical trachelectomy with pelvic lymph node assessment is the best option [6]. The radical trachelectomy consists of en bloc removal of the cervix, vaginal margins, and bilateral lymph node dissection while leaving the uterine body and fundus in situ, the uterus is attached to the remaining part of the vagina with the aid of a special stitch on the uterus to help keep the uterus closed during pregnancy [7]. Concerning our case, she had a lesion of 2 cm hyperemic, swollen cervical lesion, clinical stage 1B1, and a punch biopsy of the lesion confirmed grade 1 invasive squamous cell carcinoma of the cervix [8]. Radical trachelectomy is an acceptable surgery when it does not appear that the selected patient will impair the cure rate of early-stage malignancies, and it allows for the retention of reproductive potential. Because of concerns about the oncologic safety of larger tumors, initial eligibility criteria were restricted to patients with no more than stage IB1 tumors with good histology and a size of less than 2 cm [9]. Our patient met the criteria for radical trachelectomy since she was stage IB1, had a tumor smaller than 2 cm in diameter, was restricted to the uterine cervix, and histology confirmed grade 1 squamous cell carcinoma.
The rate of conception among women who have undergone trachelectomy is experiencing a significant increase of 70%, with 49% of them successfully giving birth at term. However, it is important to note that pregnancy following radical trachelectomy carries an elevated risk of various obstetric complications. These complications include an 8.07% rate of second-trimester pregnancy loss, a 20.5% rate of preterm delivery, occurrences of preterm premature membrane rupture, as well as abnormal bleeding from varices at the site of uterovaginal anastomosis. To mitigate these risks, certain measures should be considered. In the first trimester of pregnancy, expectant management is advisable and can be beneficial. Additionally, a cesarean section may be recommended to prevent the release of the preventive cerclage and minimize the chances of cervical lacerations. It is essential to conduct cervical cytology during and after pregnancy to detect any potential recurrence. Furthermore, it should be noted that preventative cerclage often leads to a narrowing of the cervical canal, which can result in lochiometra. However, surgical dilation can effectively manage this issue. Nevertheless, it is crucial to maintain regular follow-up due to the higher likelihood of cervical stenosis. Overall, while the rate of conception is rising among women who have undergone trachelectomy, it is essential to be aware of and manage the associated obstetric complications. By implementing appropriate measures and closely monitoring the patient’s condition, healthcare professionals can optimize outcomes for these individuals [10].
Conclusion
Radical trachelectomy is a safe and effective treatment for women with early-stage cervical cancer who preserve fertility, but a proper selection of patients, shared decision making and detailed informed consent can help to optimize desired outcomes.
Declarations
Patient’s perspective: The care provided was timely with a full explanation of the diagnosis and prognosis and a follow-up plan explained.
Acknowledgments: We are humbly grateful for the support and encouragement given by the Obstetrics/gynecology, pathology, and radiology departments at Bugando Medical Centre and the Catholic University of Health & Allied Sciences.
Timeline: The patient was consulted in our hospital and management was initiated. The intervention was done, and the patient was admitted for ten days for radical trachelectomy Preparation and completion of the case took four months. She is currently on surveillance to see if there will be any relapse and while continuing with fertility treatment.
Author’s contribution: FM authored the initial draft, evaluated the relevant literature, and contributed to patient management. On separate occasions, GN, JM, RK, FJ, AK, and DM managed the patient, read the manuscript, and approved the final draft. OO interpreted all pathological findings, examined the manuscript, and offered his professional opinion. EN wrote the initial draft, managed the patient, evaluated the literature, provided writing assistance, edited and proofread the technical language, and is the corresponding author. The final manuscript was read and endorsed by all authors.
Funding: This patient’s medical insurance covered all of the rendered services. There was no financial support from any organization.
Ethical approval and consent to participate: Written informed consent was obtained from the patient for publication of this case report, and ethical clearance was granted by the joint Catholic University of Health and Allied Sciences/ Bugando Medical Centre Research and Ethical review committee.
Consent for publication: Written informed consent was obtained from the patient for publication of this case and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal. Additionally, consent was sought and granted by the Catholic University of Health and Allied Sciences Directorate of Research and Publication to publish this work. A copy of the clearance document is also available for review by the Editor-in-Chief of this journal.
Competing interests: The authors declare that they have no competing interests.
References
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet‐Tieulent J, et al. Global cancer statistics, 2012. CA: A cancer journal for clinicians. 2015; 65: 87-108.
- Bruni L, Barrionuevo-Rosas L, Serrano B, Brotons M, Cosano R, et al. ICO Information Centre on HPV and Cancer (HPV Information Centre). Human papillomavirus and related diseases in India. Summary Report 2014; 2018.
- Lee SJ, Schover LR, Partridge AH, Patrizio P, Wallace WH, et al. American Society of Clinical Oncology recommendations on fertility preservation in cancer patients. Journal of clinical oncology. 2006; 24: 2917-31.
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A cancer journal for clinicians. 2018; 68: 394-424.
- Castellsagué X, Munoz N. Chapter 3: Cofactors in human papillomavirus carcinogenesis-the role of parity, oral contraceptives, and tobacco smoking. JNCI monographs. 2003; 2003: 20-8.
- Smith ES, Moon AS, O’Hanlon R, Leitao Jr MM, Sonoda Y, et al. Radical trachelectomy for the treatment of early-stage cervical cancer: A systematic review. Obstetrics and Gynecology. 2020; 136: 533.
- Dargent D. La tracheléctomie élargie. Cancers et grossesse. 2002: 57.
- Bhatla N, Aoki D, Sharma DN, Sankaranarayanan R. Cancer of the cervix uteri: 2021 update. International Journal of Gynecology & Obstetrics. 2021; 155: 28-44.
- Xu L, SUN FQ, WANG ZH. Radical trachelectomy versus radical hysterectomy for the treatment of early cervical cancer: A systematic review. Acta obstetricia et Gynecologica Scandinavica. 2011; 90: 1200-9.
- Bernardini M, Barrett J, Seaward G, Covens A. Pregnancy outcomes in patients after radical trachelectomy. American Journal of Obstetrics and gynecology. 2003; 189: 1378-82.