Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Vanishing lung: Tuberculosis still can do it
*Corresponding Author : João Paulo Duarte dos Santos Oliveira Rodrigues
Department of Rua de Santa Marta 50, Portugal.
Tel: +351911829533;
Email: joao.oliveira.rodrigues.pneumo@gmail.com
Received : Jul 17, 2023
Accepted : Aug 11, 2023
Published : Aug 18, 2023
Archived : www.jcimcr.org
Copyright : © Rodrigues JP (2023).
Citation: Rodrigues JP. Vanishing lung: Tuberculosis still can do it. J Clin Images Med Case Rep. 2023; 4(8): 2550.
Clinical image description
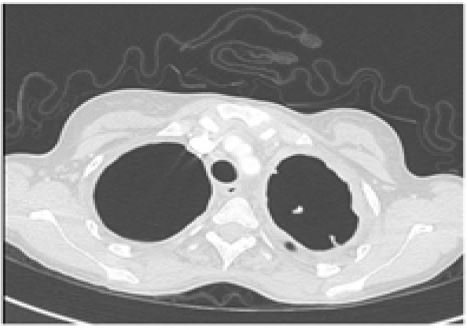
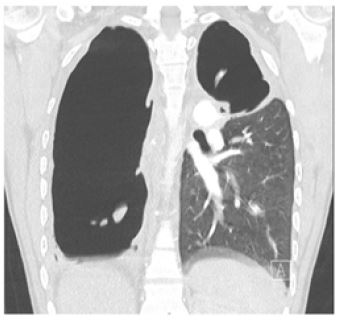
A 22-year-old female patient sought emergency medical services because she was complaining of asthenia, cough and haemoptysis for one month. She had a past medical history of a pulmonary tuberculosis four years ago while she was living abroad. The treatment was administered only for three months but isolates, antibiotic sensitivity and exact therapeutic regimen were not known. Upon clinical examination, patient exhibited sings of respiratory distress, lung sounds were abolished in the right hemithorax and diminished in the left hemithorax. Recurrent episodes of hemoptysis were evident. The chest-x-ray upon admission revealed a complete absence of lung parenchyma in the right hemithorax and in the upper half of the left hemithorax. For differential diagnosis with other common entities (eg. Pneumothorax) a CT scan was conducted. It confirmed the absolute absence of lung parenchyma both on the right hemithorax and the upper part of the left hemithorax. Pseudomonas aeruginosa was isolated in the sputum and a regimen with Piperacillin-Tazobactam was initiated. Direct smear microscopy for acid-fast bacilli, PCR testing for Mycobacterium tuberculosis, and mycobacterial culture results were all negative. Since the episodes of recurrent haemoptysis were refractory to tranexamic acid and to the antibiotic regiment, after performing a CT pulmonary angiogram, arterial embolizations were performed in two different sessions. As the patient continued to experience successive haemoptysis episodes with increased blood volume in each one and the need for blood transfusion, a rigid bronchoscopy was performed. During the procedure, the origin of the haemorrhage was identified in the right upper lobar bronchus. Unfortunately, due to a cardiac arrest, the procedure hat to be stopped with no return of spontaneous circulation.