
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Acute left vertebral artery dissection and right vertebral artery occlusion in a middle-aged man: A case report
Seyed Mohammad Mousavi; Elnaz Vafadar Moradi*
Department of Emergency Medicine, Faculty of Medicine, Mashhad university of Medical Science, Mashhad, Iran.
*Corresponding Author : Elnaz Vafadar Moradi
Department of Emergency Medicine, Faculty of Medicine, Mashhad university of Medical Science, Mashhad, Iran.
Tel: +98-51-38525312;
Email: Vafadarme@mums.ac.ir
Received : Jul 10, 2023
Accepted : Aug 15, 2023
Published : Aug 22, 2023
Archived : www.jcimcr.org
Copyright : © Moradi EV (2023).
Abstract
Spontaneous left Vertebral Artery Dissection (VAD) is an uncommon but very important etiology of acute posterior circulation stroke. We reported a case of a 43 years old man, who came with the complaint of chest pain with sudden onset, severe sweating, and dizziness. After 12 hours of the patient’s admission, he had tonic-colonic generalized seizure, generalized ataxia and new onset headache. His neurologic status deteriorated while on admission since at the consequent patients’ examination, a new onset left hemiparesis was stated by the patient, which on neuroimaging revealed a left VAD which led to cerebellar infarction. Imaging modality such as CTA and MRI can reliably and safely demonstrate the direct and indirect features of spontaneous VAD. The routine use of CTA and MRI in stroke increases the detection of VAD, therefore, promotes early diagnosis of VAD, facilitating prompt initiation of appropriate management. Concomitant connective tissue disease should be evaluated in these patients.
Keywords: Vertebral artery dissection; Stroke; Acute coronary syndrome.
Citation: Mousavi SM, Moradi EV. Acute left vertebral artery dissection and right vertebral artery occlusion in a middle-aged man: A case report. J Clin Images Med Case Rep. 2023; 4(8): 2555.
Introduction
Spontaneous Vertebral Artery Dissection (VAD) is a very important etiology of acute posterior circulation infarction and more common in middle-aged patients [1]. Generally, patients with VAD have a poor clinical outcome as the risk of stroke onset is relatively high among these patients in the next few days after VAD [2,3]. It is commonly stated that patients with unruptured VAD might have a better prognosis than those with a ruptured and hemorrhagic VAD [4]. Therefore, early diagnosis of VAD and treatment is very crucial since it can reduce major stroke or transient ischemic attack complications [5]. Whereas some studies suggested that in some patients, a history of trauma or connective tissue disease might be helpful in the diagnosis of VAD, due to the non-specific presentations of VAD, an early diagnosis of VAD seems to be difficult [6]. Digital Subtraction Angiography (DSA) has been the gold standard for the evaluation of intracranial artery disease [7]. We report a young man, who came to our emergency department complaining of chest pain with sudden onset, severe sweating, and dizziness whose neurologic status deteriorate during examination.
Case presentation
A 43-year-old healthy man developed acute onset chest pain that radiates to back and shoulders after 30 minutes of walking, sweating along with nausea and vomiting. Chest pain altered with the positional changes. General examination was normal. Cranial nerve examination was normal. Our first impression was acute coronary syndrome. Patient’s serial electrocardiograms and consequent cardiac enzymes were normal. After 12 hours of the patient’s admission, he had tonic-colonic generalized seizure. Then, generalized ataxia was also observed. Patient was also complained from the new onset headache. His neurologic status deteriorated while on admission since at the consequent patients’ examination, a new onset left hemiparesis was stated by the patient. He denied a history of hypertension, seizures, epilepsy, tobacco, alcohol, and recreational drug use or head trauma. The family history was unremarkable. On physical examination, vital signs were normal. There was no evidence of skin lesions, musculoskeletal abnormalities, lymphadenopathy, splenomegaly, or hepatomegaly. On neurologic examination, cognition was normal. Complete Blood Count (CBC), blood sugar, serum electrolytes, lipid profile, kidney and liver function tests, Erythrocyte Sedimentation Rate (ESR), and Antinuclear Antibody (ANA), Perinuclear Anti-Neutrophil Cytoplasmic Antibody (P-ANCA) and C-ANCA were all normal. The serum C-Reactive Protein (CRP) was above normal limits (56.8 mg/L). Anti-double stranded DNA (anti-dsDNA) antibodies were positive (136.8 IU/mL). There were no renal abnormalities such as proteinuria or cellular casts in the urine analysis.
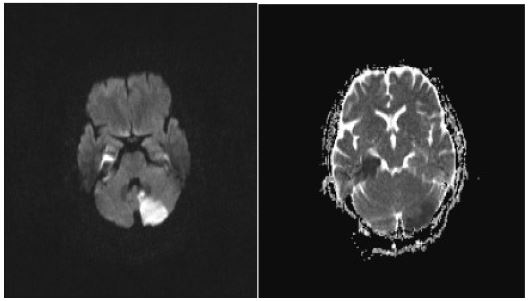
A Magnetic Resonance Imaging (MRI) of the brain showed acute ischemic lesions within the cerebellum and the right hippocampus (Figure 1).
ADC at the skull base level revealed acute infarction of cerebellum.
A CT angiography showed increased thickness along with partially mural thrombosed left vertebral artery at v2 segment without completed stenosis, which was suggestive for a dissection and right vertebral artery thrombosis (Figure 2).

Based on his clinical presentation and radiological findings, he was diagnosed with a left vertebral artery dissection and right vertebral artery thrombosis and received intravenous heparin. He was discharged home with Enoxaparin and referred to rheumatologic specialist.
Discussion
VAD is a rare, life-treating pathology with a range of symptoms, including, severe back pain, headache, dizziness, Focal Neurologic Deficit (FND), Acute Coronary Syndrome (ACS), nausea and vomiting [7]. A high clinical suspicion of a clinician in patients with nonspecific symptoms may help the diagnosis [8]. Some studies have suggested that cardiac symptoms, including ECG changes and ischemic heart disease, are secondary to excessive stimulation of the sympathetic system in the hypothalamus, leading to cardiac catecholamine’s release [9]. Herein, the patient admitted with ACS and neurological symptoms developed subsequently. VAD neurological presentation include hemorrhage, ischemia or mass effect and according to this clinical presentation, there were variable imaging findings [8]. Imaging modality such as CTA and MRI are useful to demonstrate the direct and indirect features of spontaneous VAD. Increasing use of these modalities in the evaluation of patients with acute stroke increases the detection of VAD [9,10). In this report, we could diagnose based on the clinical presentations and MRI/CT angiography findings.
Management of spontaneous VAD can be conservative or surgical treatment [1]. Our patient was treated conservatively with heparin followed by warfarin, and after 6 months follow up, his general condition was quite good. Concomitant connective tissue disease should be evaluated in these patients [11]. Our patients ANA was positive and he was referred to rheumatologist after discharge.
Conclusion
The emergency medicine specialist must have strong clinical suspicion in dealing with patients. Patient’s symptoms may be misleading, therefore good suspicion and appropriate use of diagnostic modality helps proper decision making.
Ethical review: Written informed consent was obtained from the patient.
References
- Deshmukh M, Wadhwa A, Rajdeo R. Spontaneous vertebral artery dissection: posterior circulation stroke. Journal of craniovertebral junction & spine. 2015; 6: 206.
- Czechowsky D, Hill MD. Neurological outcome and quality of life after stroke due to vertebral artery dissection. Cerebrovascular diseases. 2002; 13: 192-197.
- Chang FC, Yong CS, Huang HC, et al. Posterior circulation ischemic stroke caused by arterial dissection: characteristics and predictors of poor outcomes. Cerebrovascular Diseases. 2015; 40: 144-150.
- Park KW, Park JS, Hwang SC, Im SB, Shin WH, et al. Vertebral Artery Dissection: Natural History, Clinical Features and Therapeutic Considerations. J Korean Neurosurg Soc. 2008; 44: 109-115.
- Bachmann R, Nassenstein I, Kooijman H, et al. High-resolution magnetic resonance imaging (MRI) at 3.0 Tesla in the short-term follow-up of patients with proven cervical artery dissection. Investigative radiology. 2007; 42: 460-466.
- Gottesman RF, Sharma P, Robinson KA, et al. Clinical characteristics of symptomatic vertebral artery dissection: a systematic review. Neurologist. 2012; 18: 245-254.
- Yun SY, Heo YJ, Jeong HW, et al. Spontaneous intracranial vertebral artery dissection with acute ischemic stroke: High-resolution magnetic resonance imaging findings. The neuroradiology journal. 2018; 31: 262-269.
- Yoon W, Seo JJ, Kim TS, Do HM, Jayaraman MV, et al. Dissection of the V4 segment of the vertebral artery: clinicoradiologic manifestations and endovascular treatment. European radiology. 2007; 17: 983-993.
- Yildiz A, Arat-Ozkan AO, Kilickesmez K, C Sarimehmetoglua, Ayca B. Dissecting aneurysm of the vertebral artery mimicking an acute coronary syndrome. Journal of Cardiovascular Medicine. 2012; 13: 474-477.
- Mizutani T. Natural course of intracranial arterial dissections. Journal of neurosurgery. 2011; 114: 1037-1044.
- Gottesman RF, Sharma P, Robinson KA, et al. Clinical characteristics of symptomatic vertebral artery dissection. A systematic review. Neurologist. 2012; 18: 245.