
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Tumor thrombosis in transit
Azin Alizadehasl, MD, FACC, FASE1,2; Leila Aliabadi, MD2; Mahsa Akbarian, MD2; Somaye Mohebi, MD2*; Maryam-Sadat Alavi, MD2; Alia Bahramnejad, MD1; Amir Dousti, MD3; Kamran Roudini, MD4; Mina Mohseni, MD1; Masoud Sayyad, MD1; Parisa ahmadi, MD2
1Cardio-Oncology Research Center, Rajaie Cardiovascular Medical & Research Center, Iran University of Medical Sciences, Tehran, Iran.
2Echocardiography Research Center, Rajaie Cardiovascular Medical & Research Center, Iran University of Medical Sciences, Tehran, Iran.
3Interventional Cardiology Research Center, Rajaie Cardiovascular Medical and Research Center, Iran University of Medical Sciences, Tehran, Iran.
4Cancer institute, Imam Khomeini hospital, Tehran University of Medical Sciences, Tehran, Iran.
*Corresponding Author : Somaye Mohebi
Echocardiography Research Center, Rajaie CardioVascular Medical & Research Center, Iran University of Medical Sciences, Tehran, Iran.
Email: somayemohebbi57@gmail.com
Received : Jul 11, 2023
Accepted : Aug 15, 2023
Published : Aug 22, 2023
Archived : www.jcimcr.org
Copyright : © Mohebi S (2023).
Abstract
Hepatocellular Carcinoma (HCC) is a poor prognosis cancer of liver which could be associated with venous thrombo-emboli but cardiovascular metastasis is rare; Here we present a case of HCC with tumor thrombosis and clot in transit who managed conservatively with anticoagulation.
Citation: Alizadehasl A, Aliabadi L, Akbarian M, Mohebi S, Alavi MS, et al. Tumor thrombosis in transit. J Clin Images Med Case Rep. 2023; 4(8): 2556.
Introduction
Hepatocellular carcinoma is most common primary liver malignancy. Advanced hepatocellular carcinomas represent a disease with poor prognosis [1]. Sixth most prevalent cancer and fourth most common cause of cancer mortality worldwide and a median survival time of four to seven months [2]. Intra cardiac involvement and invasion of the hepatic vein, inferior vena cava, pulmonary artery, and right atrium is rather rare with poor Prognosis [3]. The major risk factors include chronic liver disease leading to cirrhosis, and most common etiologies are viral hepatitis (HBV and HCV), heavy alcohol consumption, and fatty liver disease [4]. Increased alpha fetoprotein with 60% sensitivity and 90% specificity and also elevated liver enzymes are commonly used for hepatocellular carcinoma detection [5]. For staging the tumor and defining the best therapeutic, Barcelona Clinic Liver cancer (BCLC) algorithm is the most widely applied Hepatocellular carcinoma management system. Criteria of advance stage (c) are portal invasion, extra hepatic spread and preserved liver function [6]. A review of 14 cases of HCC patients with pulmonary thrombo-emboli showed the one-year survival was higher for those who had surgery (40%) and lower for whom didn’t (0%). So, hepatic resection and removal of tumor thrombi should be considered to prolong the patient’s life span [7]. HCC patients with pulmonary thrombo-emboli and IVC invasion have been reported to survive less than two months without surgery [7]. Pulmonary thromboembolism and right atrium mass as the first manifestation of HCC is rare (2%) [3]. Here we report a 56 -year- old man with right atrial mass and pulmonary thromboembolism as a first manifestation of HCC.
Case presentation
A 56 -year-old man with lower extremities edema that was started from three weeks ago.
In his medical history he had a history of diabetes mellitus, hypertension, dyslipidemia. He was current smoker. There is no Hepatitis or any other liver dysfunction in his history.
Physical examination on admission was unremarkable except for pitting lower extremities edema. A 12 - lead ECG revealed normal sinus rhythm with no specific change. The results of the laboratory test were as follows: Hemoglobin: 12.1 mg/dl, leukocytes count: 7900, Platelet count: 135000, Prothrombin time: seconds, Prothrombin International normalized ratio, Activated partial thromboplastin time: Aspartate aminotransferase: 130, Total bilirubin: 1.2. Albumin: 3, Alanine aminotransferase: 117, creatinine: 7.2, BUN:72.
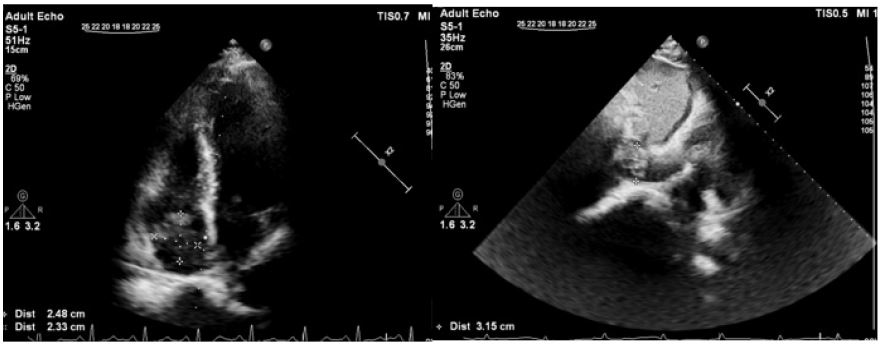
Two-dimensional transthoracic echocardiography was performed in first day of admission and revealed normal left ventricular size with mild systolic dysfunction left ventricular ejection fraction: 50%. Normal right ventricular size and systolic function. Normal bilateral sizes. Valvular had no significant stenosis. Nor regurgitation, no Pericardial effusion. Large mass (4.3 cm x 1.6 cm) in inferior vena cava that extended to right atrium and protrude to right ventricle (Figure 1). Color Doppler echocardiography was repeated in the second day of admission due to patient change symptom and he developed with dyspnea, that the result was different, a mass in right atrium was disappeared (Figure 2), so perfusion ventilation lung scan was performed. Perfusion lung scan by TC99m revealed multiple lung segmental perfusion defect. Abdominopelvic sonography was done for him, heterogeneous mass like lesion is noted in the segment sixth of liver and measures about 40 millimeters diameter. Both kidneys show increased parenchymal echogenicity. Spleen showed normal size and parenchyma echo pattern. Inferior vena cava showed dilated and contains filling defect and without flow. Hepatic veins show hypoechoic material and without obvious flow. Bilateral common iliac veins showed filling defect, mostly suggestive of thrombosis.
According to color Doppler echocardiography, that was highly suspicious to thrombosed tumor and sonography that revealed IVC and common iliac vein thrombosis, and also ventilation perfusion scan that was suggestive for pulmonary thromboembolism, so anticoagulant therapy was started for him. Due to increase in creatinine and the following nephrologist consult, two times hemodialysis was done. Creatinine level was decreased to 2.1 and due to adequate diuresis, dialysis was stopped. Edema was resolved. Oncologist consult was requested. In concordance with abdominal sonography that revealed mass in liver and positive PCR for hepatitis B, alpha fetoprotein was checked that was higher than normal range (47.9). The patient was discharged with amlodipine 5 mg, two times a day, Valsartan 80 mg two times a day. Atorvastatin 40 mg daily and enoxaparin 80 mg two times a day, also he had oncologist and cardiologist follow up.
The patient was admitted one month later with abdominal pain, abdominal protrusion and lower extremities edema. 2D echo color Doppler was performed and revealed RA, IVC mass. Alpha fetoprotein that was 60.6. Liver biopsy was done and HCC was confirmed. After intensive anticoagulant therapy and starting Sorafenib 200 mg 2 times a day, the patient was discharged with warfarin 5 mg daily, ASA 80 mg daily, carvedilol 3.125 mg 2 times a day, furosemide 40 mg 2 times a day, atorvastatin 20 mg daily, gliclazide 30 mg daily.

Discussion
Compared with older series, there was a significant increase in the incidence of cardiac metastasis in cancer patients after 1970, probably related to improvements in technique and availability of cardiac imaging modalities [8]. Acute pulmonary thrombo-emboli as the primary manifestation of HCC with tumor associated thrombosis in the IVC and the right atrium is rare [3]. However, metastatic spread of malignancies to lung is common, pulmonary tumor embolism is not frequent.
In this case, creatinine was increased transiently. Normal hematocrit, and high alpha fetoprotein level was detected. Serological examinations disclosed hepatitis B infection. Brain CT scan was performed for him that had no pathologic finding. Sonography of the abdomen showed, heterogenous mass like lesion about 40 millimeter diameter. Spiral CT scan of the thorax without contrast reveals a solid parenchymal nodule measured 4.5 mm in left upper lobe of lung, sub segmental wedge-shaped consolidation in left lower lobe highly compatible with infarction. The diagnosis of HCC is typically determined by radiological liver imaging in combination with Alpha Fetoprotein without the need for biopsy. As there is a consensus that biopsy proof of HCC is not required in patients with chronic hepatitis B infection or cirrhosis [8,9]. Cancer associated thrombosis is a well-known condition, and hepatic carcinoma is highly associated with venous thromboembolism [10]. Intra atrial manifestation of the HCC is a life -threatening condition. In such situation, cause of death mostly is due to pulmonary embolism or obstruction of the tricuspid valve. In these conditions hepatic tumor resection can provide relatively good long- term survival (not more than two years) [11]. Optimal decision making in rare cases is a complicated task. In our case, right atrial mass was resolved by anticoagulation therapy, temporary. For HCC management, the patient referred to oncologist.
References
- Zhu AX, Park JO, Ryoo BY, Yen CJ, Poon R, et al. Ramucirumab versus placebo as second-line treatment in patients with advanced hepatocellular carcinoma following first-line therapy with sorafenib (REACH): A randomised, double-blind, multicentre, phase 3 trial. The lancet oncology. 2015; 16: 859-70.
- Yang JD, Hainaut P, Gores GJ, Amadou A, Plymoth A, et al. A global view of hepatocellular carcinoma: trends, risk, prevention and management. Nature reviews Gastroenterology & hepatology. 2019; 16: 589-604.
- Sempokuya T, Bolger Jr DT. Right atrium invasion of tumor thrombus from hepatocellular carcinoma incidentally found on transthoracic echocardiogram. Hawai’i Journal of Medicine & Public Health. 2018; 77: 131.
- Kar P. Risk factors for hepatocellular carcinoma in India. Journal of clinical and experimental hepatology. 2014; 4: S34-42.
- Daniele B, Bencivenga A, Megna AS, Tinessa V. α-fetoprotein and ultrasonography screening for hepatocellular carcinoma. Gastroenterology. 2004; 127: S108-12.
- Lee YS, Seo YS, Kim JH, Lee J, Kim HR, et al. Can more aggressive treatment improve prognosis in patients with hepatocellular carcinoma? A direct comparison of the Hong Kong Liver Cancer and Barcelona Clinic Liver Cancer Algorithms. Gut and liver. 2018; 12: 94.
- Lin HH, Hsieh CB, Chu HC, Chang WK, Chao YC, et al. Acute pulmonary embolism as the first manifestation of hepatocellular carcinoma complicated with tumor thrombi in the inferior vena cava: Surgery or not?. Digestive diseases and sciences. 2007; 52: 1554-7.
- Al-Mamgani A, Baartman L, Baaijens M, de Pree I, Incrocci L, et al. Cardiac metastases. International journal of clinical oncology. 2008; 13: 369-72.
- McMahon BJ. The natural history of chronic hepatitis B virus infection. Hepatology. 2009; 49: S45-55.
- Tandon P, Garcia‐Tsao G. Prognostic indicators in hepatocellular carcinoma: A systematic review of 72 studies. Liver International. 2009; 29: 502-10.
- Fukuda S, Okuda K, Imamura M, Imamura I, Eriguchi N, et al. Surgical resection combined with chemotherapy for advanced hepatocellular carcinoma with tumor thrombus: report of 19 cases. Surgery. 2002; 131: 300-10.