
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Huge multi-nodular goitre over 50 years: Case report
Olivia Kimario1*; Patric Ngoya2; Osca Otman3; Zephania Saitabau Abraham4; Fabian Massaga5
1Department of Otorhinolaryngology, Catholic University of Health and Allied Sciences, P.O. Box 1464, Mwanza, Tanzania.
2Department of Radiology, Catholic University of Health and Allied Sciences, P.O. Box 1464, Mwanza, Tanzania.
3Department of Pathology, Catholic University of Health and Allied Sciences, Mwanza, Tanzania.
4Department of Surgery, University of Dodoma, School of Medicine and Dentistry, Dodoma, Tanzania.
5Department of Surgery, Catholic University of Health and Allied Sciences, P.O. Box 1464, Mwanza, Tanzania.
*Corresponding Author : Olivia M Kimario
Department of otorhinolaryngology, Catholic University of Health and Allied Sciences, P.O. Box 1464, Mwanza Tanzania.
Email: oliviakimario@yahoo.co.uk
Received : Jul 03, 2023
Accepted : Aug 16, 2023
Published : Aug 23, 2023
Archived : www.jcimcr.org
Copyright : © Kimario OM (2023).
Abstract
Multi-nodular goitre is very common in our environment. Our environment do covers some parts with lack of iodine. Multi-nodular goitre may develop as toxic or non-toxic depending on the thyroid functional status. This disorder has a predilection for females as compared to males due to their body needs that is more on the reproductive system. We are presenting 85 years old female reported to our clinic with complaint of anterior neck swelling for 57 years. The swelling was of gradual onset associated with difficulties in breathing and swallowing. We did investigate the patient and later on operated the patient, whereby total thyroidectomy was done. Histopathological results revealed a calcific multi-nodular goitre. We are concluding by teaching patients to seek medical services whenever see any swelling developing in their body whether it’s painfully or not painfully because chance of causing obstruction and transformation to malignancies is also highly suspected. This case is the first one of its kind to be operated at our hospital as the swelling has existed for more than 50 year old.
Keywords: Huge; Multi-nodular goitre; Thyroid.
Citation: Kimario O, Ngoya P, Otman O, Abraham ZS, Massaga F. Huge multi-nodular goitre over 50 years: Case Report. J Clin Images Med Case Rep. 2023; 4(8): 2557.
Introduction
Multi-Nodular Goitre (MNG) is a common type of thyroid disease that occurs often in our environment. Benign MNG is a common problem affecting 5% of the general population in non-endemic and 15% in endemic areas [1]. However, the incidence of benign goitre causing acute airway obstruction is as low as 0.6% [2]. Many MNGs are nontoxic but may be toxic at times. MNG is thought to arise primarily from two factors. The first factor is genetic heterogeneity of follicular cells with regard to function which is thyroid hormone synthesis and growth. The second factor is the acquisition of new qualities that were not present in mother cells and become inheritable during further replication. Mutations may occur in follicular cells leading to constitutively activated adenomas and to hyperthyroidism. These factors may lead to loss of anatomical and functional integrity of the follicles and of the gland as a whole. These processes ultimately lead to goiter formation and are accelerated by stimulatory factors. These stimulatory factors are based on an elevated serum Thyroid Stimulating Hormone (TSH), brought about by secondary events such as iodine deficiency, inborn errors of thyroid hormone synthesis, goitrogens or local tissue growth-regulating factors. These basic and secondary factors may cause the thyroid to grow and gradually evolve into an organ containing hyperplastic islands of normal glandular elements, together with nodules and cysts of varied histologic pattern.
In general, in iodine sufficient countries the prevalence of multi-nodular goitre is not higher than 4% [3]. In countries with previous deficiency that was corrected by universal salt iodination, elderly subjects may have an incidence of approximately10% of nodular and multi-nodular goitre, attributed to lack of nutritional iodine in early adult life [4].
Case presentation
We are presenting 85 years old female from Geita Region who attended at our otorhinolaryngology clinic with the main complaint of a painless anterior neck swelling for 57 years. She disclosed that the anterior neck swelling was of gradual onset, increased in size with time and was associated with difficulty in breathing ad in swallowing. Patient denied any history of palpitations, cold or heat intolerance, loss of weight, abnormal protrusion of the eyes during the course of illness. There was no familial history, no history of radiation exposure nor predisposing medication use. On review of other systems were essentially normal. She reports past medical history of local herbal use with no improvement. On general examination, patient was stable. On local examination, an anterior neck mass measuring about 12 cm by 10 cm was elucidated. Mass was nodular in texture, firm, non-tender and mobile not fixed to underlying structures.
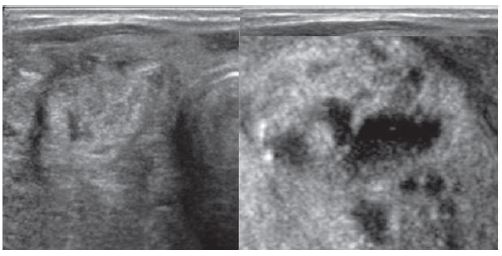
Ultrasound (Figure 1) demonstrated enlarged bilateral (right greater than left) thyroid lobes with areas of heterogeneous nodules, some with cystic degeneration and calcifications. Both lobes were highly vascularized with trachea slightly deviated to the left.
Laboratory investigations were normal including the thyroid function test. Fine needle aspiration cytology revealed no features of malignancy. The hormonal panel T3,T4,TSH was normal. We heard a diagnosis of a benign non-toxic multi-nodular goiter and patient underwent total thyroidectomy as illustrated below.
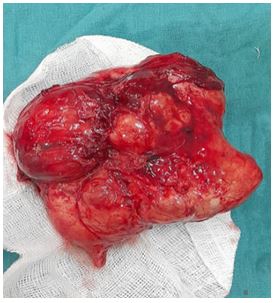
During the procedure, the MNG demonstrated increased vascularity and collateral blood supply to with moderate hemorrhage, however hemostasis was successfully achieved. The right lobe measured about 12 cm by 10 cm whereas the left lobe measured 5 cm by 4 cm (Figure 2). The bilateral recurrent laryngeal nerves and bilateral parathyroid glands were well identified, gently dissected and released. The resected MNG weighed approximately 800 g (Figure 3). The surgical bed is shown after the MNG removal (Figure 4). The surgical bed closed was in layers and a drain left in situ (Figure 5).
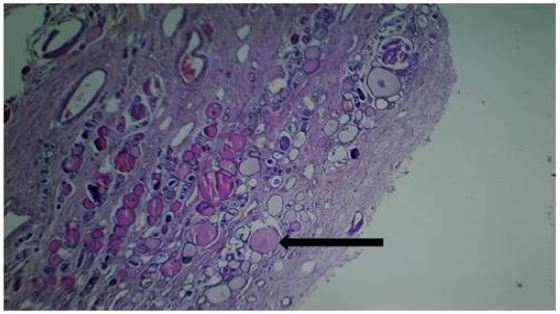
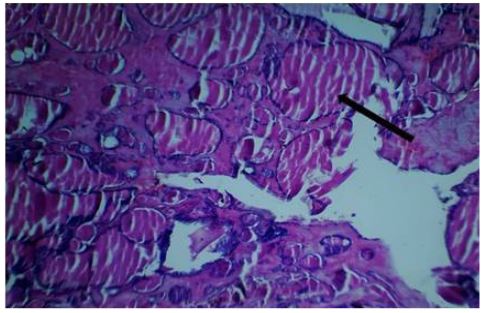
Post-operatively, the patient was kept on analgesia (i/v pethidine 100 mg tds for 24 hrs), antibiotics (i/v ampiclox 500 mg tds for 3 days), i/v dexamethasone 8 mg tds 24 hrs, i/v Dextrose-Normal Saline alternating with Ringer’s Lactate 2 litres for 24 hrs and p.o levothyroxine 0.1 mg daily. Patient progressed well, on the third day was discharged. After discharge patient should come follow up at the clinic after 2 weeks. The histopathology results revealed a benign multi-nodular goiter with areas of calcifications.
In the follow up clinic patient was well with calcium and hormonal panel T3,T4 and TSH within the normal range.
Post-operatively, the patient was kept on analgesia (i/v pethidine 100 mg tds for 24 hrs), antibiotics (i/v ampiclox 500 mg tds for 3 days), i/v dexamethasone 8 mg tds 24 hrs, i/v Dextrose-Normal Saline alternating with Ringer’s Lactate 2 litres for 24 hrs and p.o levothyroxine 0.1 mg daily. Patient progressed well, on the third day was discharged. After discharge patient should come follow up at the clinic after 2 weeks. The histopathology results revealed a benign multi-nodular goiter with areas of calcifications.


In the follow up clinic patient was well with calcium and hormonal panel T3,T4 and TSH within the normal range


Discussion
Most of the patients develop MNG due to iodine deficiency (endemic goiter) or medication use, growth-stimulating antibodies, and inherited defects in thyroid hormone synthesis [1]. Many patients present with huge thyroid enlargement resulting in pressure symptoms like dyspnea and dysphagia. As presented in this case, the patient presented with pressure symptoms but was in euthyroid free state. We operate the patient in order to allievate the pressure symptoms. Intra-operatively, we achieved adequate haemostasis despite moderate hemorrhage due to increased vascularity and collateral blood supply to the MNG. We managed to totally resect the MNG without injury to the recurrent laryngeal nerves or the parathyroid glands. This was evident post-operatively i.e. patient voice was unchanged and the serum calcium levels were within normal limits. We kept the patient on daily life-long levothyroxine supplements as per post-total thyroidectomy protocol [5]. The histopathology results of our patient revealed a benign multi-nodular goiter with calcifications. Calcifications were due to the chronicity of the MNG. The percentage of MNGs that undergo malignant degeneration is about 4% to 17% [3], which our patient was in the luck side.
Conclusion and recommendation
Multi-nodular goiter is common in our geographical setting predominantly due to the iodine deficiency. We urge patient to be given supplements that contain iodine to bridge this problem. A neglected multi-nodular goitre has a risk of developing complications such as pressure symptoms or malignant trasformation. Therefore, patients are advised to actively seek early medical services.
Declaration of competing interest
The authors declare that they have no competing interests.
Funding: CUHAS.
Ethical approval: Approval for the publication of this case series was sought from the Joint CUHAS/BMC Ethics and Review Committee.
Consent: Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal upon request.
Author contributions: OMK participated in managing the patient and in preparation of the original of manuscript.
PNS management of the patient and revision of the manuscript.
OO participated in management of the patient and contribute to the manuscript.
ZSA contributed to the over view of the manuscript.
Acknowledgements: I would like to extend my sincere gratitude to all department members and all who contributed on one way or another in continuous support and inputs in this case report.
References
- Abraham D, Singh N, Lang B, Chan WF, Lo CY. Benign nodular goitre presenting as acute airway obstruction. ANZ journal of surgery. 2007; 77: 364-7.
- Ríos A, Rodríguez JM, Canteras M, Galindo PJ, Tebar FJ, et al. Surgical management of multinodular goiter with compression symptoms. Archives of Surgery. 2005; 140: 49-53.
- Pinchera A, Aghini-Lombardi F, Antonangeli L, Vitti P. Multinodular goiter. Epidemiology and prevention. AnnaliItaliani di Chirurgia. 1996; 67: 317-25.
- Jarløv AE, Nygaard B, Hegedüs L, Hartling SG, Hansen JM. Observer variation in the clinical and laboratory evaluation of patients with thyroid dysfunction and goiter. Thyroid. 1998; 8: 393-8.
- Roos A, Linn-Rasker SP, van Domburg RT, Tijssen JP, Berghout A. The starting dose of levothyroxine in primary hypothyroidism treatment: A prospective, randomized, double-blind trial. Archives of internal medicine. 2005; 165: 1714-20.