
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Rothia mucilaginosa pneumonia developing after COVID-19
Deniz Bilici1; Cansel Peker1; Coskun Dogan2; Burcu Arpınar1
1Istanbul Medeniyet University Faculty of Medicine, Department of Chest Diseases, Istanbul, Turkey.
2Medeniyet University Faculty of Medicine, Department of Chest Diseases, Istanbul, Turkey.
*Corresponding Author : Deniz Bilici
Istanbul Medeniyet University Faculty of Medicine, Department of Chest Diseases, Istanbul, Turkey.
Tel: +90-5057590406;
Email: dr.deniz.bilici@gmail.com
Received : Jul 11, 2023
Accepted : Aug 16, 2023
Published : Aug 23, 2023
Archived : www.jcimcr.org
Copyright : © Bilici D (2023).
Abstract
Rothia Mucilaginosa (RM) is a bacteria found in the flora of the upper respiratory tract that can cause lower respiratory tract infections in immunocompromised individuals or the presence of significant comorbidities. The number of cases reported as a cause of pneumonia in the literature is quite a few. When the literature is examined, it is reported that unexpected pathogens may be a factor in the lungs, especially after COVID-19. This case is presented because it is the first report which is COVID-19 related to RM pneumonia after COVID-19.
Keywords: COVID-19; Pneumonia; Rothia mucoliginosa.
Citation: Bilici D, Peker C, Dogan C, Arpinar B. Rothia mucilaginosa pneumonia developing after COVID-19. J Clin Images Med Case Rep. 2023; 4(8): 2558.
Introduction
Rothia Mucilaginosa (RM) is a gram-positive, aerobic, encapsulated, nonmotile opportunistic pathogen, found in the flora of the upper respiratory tract and nasopharynx, belonging to the family of Micrococcaceae. It has been reported to cause infection mostly in immunocompromised individuals and rarely in patients with chronic diseases who have no immunodeficiency [1,2]. RM pneumonia, which is mostly presented as case reports in the literature, still maintains its rarity, and optimal antimicrobial therapy for RM pneumonia has not been determined yet. It is sensitive to most antibiotics that are generally active against gram-positive cocci [3].
It is known that bacterial respiratory tract infections increase after viral respiratory tract infections [4]. Studies show that the rate of secondary infection developing after COVID-19 varies between 1% and 10% [5-7]. In addition, it was emphasized that the lung microbiota of the cases may change after COVID-19 and that pneumonia can be seen with normally non-pathogenic agents [7,8].
While our case was being treated for COVID-19 pneumonia, it is presented to draw attention to the fact that RM, which grows in the Bronchoalveolar Lavage (BAL) fluid and is normally found in the flora of the upper respiratory tract, may be a cause of pneumonia, especially after COVID-19.
Case presentation
A 44-year-old male patient, who was treated in the intensive care unit for 7 days with the diagnosis of COVID-19 a month ago, presented to the pulmonary medicine polyclinic with complaints of shortness of breath and chest pain. His past medical history was unremarkable except for the diagnosis of Chronic Lymphocytic Leukemia (CLL) 2 years ago. He received his last Chemotherapy (CT) treatment 6 months ago.
Posterior-Anterior (PA) chest X-ray showed non-homogeneous opacities in bilateral mid-lower zones (Figure 1). Laboratory tests revealed White Blood Count (WBC): 11.6 x 103/uL, neutrophil: 8,69 x 103/uL (74,9%), hemoglobin (Hb): 11.7 g/dL, Hematocrit (Htc): 37%, serum reactive protein (CRP): 138.3 mg/L, Sedimentation Rate (ESR): 120 mm/h, urea: 16 mg/dl, creatinine: 0.69 mg/dl, Alanine Aminotransferase (ALT): 15 U/L, Aspartate Aminotransferase (AST): 17 U/L, LDH: 262 U/L, Sodium (Na): 134 mmol/L, Potassium (K): 5.2 mmol/L, Calcium (Ca): 8.6 mg/dl, chloride (Cl): 99 mmol/L. Physical examination (PE) showed moderately good general health, open conscious, and cooperatively oriented, Blood Pressure (BP): 112/76 mmHg, Heart Rate (HR): 94/minute, Respiratory Rate (RR): 20/minute, Oxygen Saturation (SaO2): 95%, temperature: 36.2oC. On auscultation, there were widespread rales in the middle of the lower areas. The patient, who was hospitalized in the chest diseases clinic with the current findings, was started as an empirical treatment with piperacillin, tazobactam 4 x 4.5 gr Intravenous (IV), and ciprofloxacin 2 x 400 mg orally pill combination.
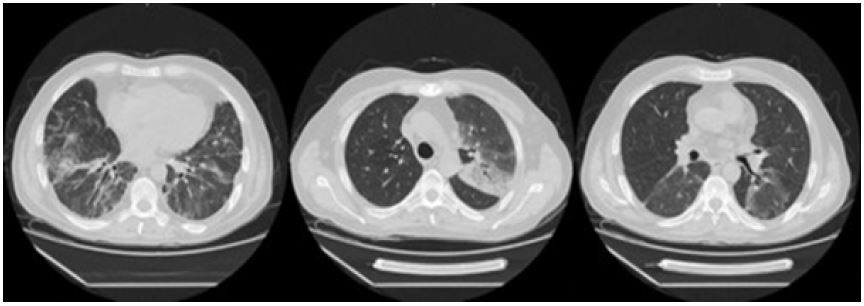
There was a partial regression in the patient’s complaints with the start of antibiotic therapy, however, on the 6th day of the treatment, a progression was detected in the CRP and procalcitonin values, which were measured after fever (CRP: 109.5 mg/L, procalcitonin: 0.081ug/L). Newly developed consolidation was detected in the left upper zone in the control PA chest X-ray (Figure 2). His current antibiotic therapy was stopped and replaced with IV meropenem 3 x 1 g and IV linezolid 2 x 600 mg. Thoracic Computed Tomography (CT) and Fiberoptic Bronchoscopy (FOB) were planned for microbiological sampling since he could not produce sputum. In the thoracic CT, ground-glass densities with a slight consolidation are observed in the right middle lobe and the apicoposterior segment of the left upper lobe along with in both lower lobes interlobar septal thickenings and diffusely blurred ground-glass densities were reported (Figure 3). In the FOB, both bronchial systems, all lobes, bronchi, and segments were seen as open and normal, no endobronchial lesion was observed, and a BAL sample was taken from the left upper lobe. Acid-Resistance Bacillus (ARB), bacteria, and fungal cultures were sent to exclude tuberculosis from the BAL fluid, and cytology was sent to exclude malignancy. On the second day in BAL culture, gray-colored, dense, and sticky colonies grew, and they were defined as RM. No treatment changes were made in the patient whose complaints, CRP values, and fever regressed with the empirical treatment (meropenem and linezolid). On the 7th day of the treatment, the case with a significant improvement in the control PA chest X-ray (Figure 4) and a significant regression in the control laboratory tests (CRP: 6.6 mg/L, WBC: 5.1 x 103/uL, ESR: 23mm/h) was discharged on condition that he comes for a follow-up visit.



Discussion
RM, which is an opportunistic pathogen found in the flora of the upper respiratory tract and nasopharynx, rarely causes pneumonia. It is frequently seen in immunocompromised individuals or patients with comorbidities that suppress immunity. In the series of Ramanan P et al [1], one of the largest published cohorts of RM infections, hematological malignancy predominated in most cases (19 leukemia/4 lymphomas). In this study, it was reported that hematological malignancies are a risk factor for RM infections, also it was emphasized that having a central venous catheter for active chemotherapy and especially with prolonged and deep neutropenia, may be a predisposing factor for serious RM infections. In this study, it was shown that patients with hematological malignancies had neutropenia lasting for approximately 9.5 days. In our case, there was a diagnosis of CLL similar to the literature, but he was diagnosed with CLL 2 years ago, received the last chemotherapy treatment 6 months ago, and neutropenia was not present at the time of RM pneumonia.
Since it is a member of the upper respiratory tract flora, it should be differentiated whether the colonization of the reproducing agent is the cause of active infection in RM pneumonia. For this reason, RM growth should be taken into account in the cultures of bronchoscopic samples taken from the cases. In studies, bronchoscopic sampling is recommended for diagnosis [9,10]. In our case, the growth of RM in the bronchoalveolar lavage culture after clinical-radiological progression supported the diagnosis. Studies have reported that RM is generally sensitive to most beta-lactam antimicrobials, such as rifampin and vancomycin [11,12]. In our case, RM was detected during the beta-lactam group antibiotic treatment, therefore, the treatment was continued in the same way because the clinical and radiological response was good to the empirically initiated meropenem and linezolid treatment.
COVID-19 disease, which first spread to the world from Wuhan, province of China, in 2019, is a disease with high morbidity and mortality that commonly affects the lungs. The widespread involvement in the lungs suggested that it may also change the microbiota of the lungs. For this purpose, Han Y et al [8] analyzed the microbiological data of BAL fluid of COVID-19 and healthy control and concluded that passing COVID-19 profoundly changes the lung microbiota. In this study, it is important to find significantly increased RM in the lungs of patients with COVID-19. The authors concluded that the RM they encountered in COVID-19 cases, although part of the normal oropharyngeal flora, may be the result of the effect of COVID-19 on the immune system. The fact that our case had COVID-19, was hospitalized in the COVID intensive care unit, and RM was produced in the BAL fluid made us think of RM pneumonia when we evaluated the current clinical, radiological, and laboratory findings together.
It is known that there are close interactions such as symbiosis and competition between microorganisms in the human body [13,14]. It is possible that COVID-19 disease, which is a disease with widespread involvement in the lungs, affects/changes the microbiota of the lungs. In severe COVID-19 cases, this should be kept in mind in unexpected clinical and radiological situations, and diagnosis and treatment should be re-evaluated considering this information.
Declarations
Author contributions:
Literature search: Cansel Peker, Burcu Arpınar Yiğitbaş.
Manuscript preparation: Coşkun Doğan, Deniz Bilici, Cansel Peker.
Review of manuscript: Deniz Bilici, Coşkun Doğan.
Support: This manuscript is not supported by material or other forms of support.
Conflicts of interest: We declare that we have no conflicts of interest.
References
- Ramanan P, Barreto JN, Osmon DR, Tosh PK. Rothia bacteremia: A 10-year experience at Mayo Clinic, Rochester, Minnesota. J Clin Microbiol. 2014; 52: 3184-3189.
- Fanourgiakis P, Georgala A, Vekemans M, Daneau D, Heymans C, et al. Bacteremia due to Stomatococcus mucilaginosus in neutropenic patients in the setting of a cancer institute. Clin Microbiol Infect. 2003; 9: 1068-1072.
- Maraki S, Papadakis IS. Rothia mucilaginosa pneumonia: A literature review. Infectious Diseases. 2015; 47: 125-129.
- Hendaus MA, Jomha FA, Alhammadi AH. Virus-induced secondary bacterial infection: A concise review. Ther Clin Risk Manag 2015; 24: 1265-1271.
- Chen NZM, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. The Lancet. 2020; 395: 507-513.
- Huang C, Wang Y, Li X, Ren L, Zhao J, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020; 395: 497-506.
- Shen Z, Xiao Y, Kang L, Ma W, Shi L, et al. Genomic diversity of SARS-CoV-2 in Coronavirus Disease 2019 patients. Clin Infect Dis. 2020; 71: 713-720.
- Han Y, Jia Z, Shi J, Wang W, He K. The active lung microbiota landscape of COVID-19 patients through the metatranscriptome data analysis, Bioimpacts. 2022; 12: 139-146.
- Martinez CB, Molina LZ, Sevila LG, Carbonell JG, Rincon JMN, et al. Rothia mucilaginosa Pneumonia in an Immunocompetent Patient, Arch Bronconeumol. 2014; 50: 493-495.
- de Ayala Fernández JÁ, Galán Ros J, Tamayo L. Acute respiratory distress syndrome due to severe community-acquired pneumonia caused by Rothia mucilaginosa in an immunocompetent patient. Med Clin (Barc). 2021; 156: 198-199.
- Lambotte O, Debord T, Soler C, Roue R. Pneumonia Due To Stomatococcus Mucilaginosus in an AIDS Patient Case Report And Literature Review, Clin Microbiol Infec.t 1999; 5: 112-114.
- von Eiff C, Herrmann M, Peters G. Antimicrobial susceptibilities of Stomatococcus mucilaginosus and of Micrococcus spp. Antimicrob Agents Chemother. 1995; 39: 268-270.
- Pickard JM, Zeng MY, Caruso R, Núñez G. Gut microbiota: Role in pathogen colonization, immune responses, and inflammatory disease. Immunological Reviews. 2017; 279: 70-89.
- Zuo T, Liu Q, Zhang F, Lui GC-Y, Tso EY, et al. Depicting SARS-CoV-2 faecal viral activity in association with gut microbiota composition in patients with COVID-19. Gut. 2021; 70: 276-284.